You might also like
- Pap Smear - Overview, Indications, PreparationDocument11 pagesPap Smear - Overview, Indications, PreparationBayu Surya DanaNo ratings yet
- B SC Nursing Syllabus INC PDFDocument183 pagesB SC Nursing Syllabus INC PDFsohini bhattacharyaNo ratings yet
- Identification of Microorganisms: Unknown SpecimensDocument10 pagesIdentification of Microorganisms: Unknown SpecimensAnonymous wVgEAr6No ratings yet
- 847 - Protein Energy MalnutritionDocument20 pages847 - Protein Energy MalnutritionPriyanka Vikas TakNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Assignment On Pharamcological Aspects - BY KAMINI2Document9 pagesAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyNo ratings yet
- Esophageal CancerDocument25 pagesEsophageal CancerK poojithaNo ratings yet
- Lesson PlanDocument8 pagesLesson PlanUpendra Nayka50% (2)
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad PrasadNo ratings yet
- Displacement of The UterusDocument32 pagesDisplacement of The UterusRaja100% (1)
- Nosocomial Infections in NewbornsDocument10 pagesNosocomial Infections in NewbornsAntony Rose AbyNo ratings yet
- Procedures and Nurses' Role in Material ManagementDocument28 pagesProcedures and Nurses' Role in Material ManagementbabyNo ratings yet
- Epidemiological Traid JayaDocument25 pagesEpidemiological Traid JayajayalakshmiNo ratings yet
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDocument24 pagesNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarNo ratings yet
- Universal PrecautionDocument10 pagesUniversal PrecautionParth VasaveNo ratings yet
- Hap PDFDocument17 pagesHap PDFRishu Rishma100% (1)
- Antenatal Diag - Prac.teach Lesson PlanDocument16 pagesAntenatal Diag - Prac.teach Lesson Planvikas takNo ratings yet
- Failure to Thrive TeachingDocument10 pagesFailure to Thrive TeachingSAYMABANUNo ratings yet
- Tamilnadu Nurses Council Inspection ReportDocument43 pagesTamilnadu Nurses Council Inspection ReportchrisNo ratings yet
- Health Problems MyselfDocument54 pagesHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Communicable DiseasesDocument56 pagesCommunicable DiseasesLili Nini100% (1)
- SarcomaDocument2 pagesSarcomaedrichaNo ratings yet
- Time Specific Objective Content Teaching Learning Activities Evaluati ONDocument20 pagesTime Specific Objective Content Teaching Learning Activities Evaluati ONAnnette BainesNo ratings yet
- A Visit Report To Water Treatment Plant, Bhubaneswar Water Works, Palasuni, Bhubaneswa, OdishaDocument14 pagesA Visit Report To Water Treatment Plant, Bhubaneswar Water Works, Palasuni, Bhubaneswa, OdishaANISH MISHRANo ratings yet
- Complications of Third Stage of Labour NishaDocument21 pagesComplications of Third Stage of Labour NishaSonia SapehiaNo ratings yet
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanNo ratings yet
- Vijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyDocument3 pagesVijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyReshma Rinu50% (2)
- Infection Control - LESSON PLANDocument53 pagesInfection Control - LESSON PLANJincy JohnyNo ratings yet
- IUCD Manual EnglishDocument194 pagesIUCD Manual EnglishHarshaWakodkarNo ratings yet
- BSC Nursing Syllabus First YearDocument22 pagesBSC Nursing Syllabus First YearDiksha chaudharyNo ratings yet
- Congenital AbnormalitiesDocument45 pagesCongenital AbnormalitiesSaad AbdullahNo ratings yet
- Diagnosis of PregnancyDocument16 pagesDiagnosis of PregnancySùjâl PätídàrNo ratings yet
- Assignment ON Observation ChecklistDocument7 pagesAssignment ON Observation ChecklistParbati samantaNo ratings yet
- Cervicitis Causes, Symptoms, Diagnosis and TreatmentDocument7 pagesCervicitis Causes, Symptoms, Diagnosis and TreatmentElaisa Mae Delos SantosNo ratings yet
- Epidemilogy Measurment MethodsDocument100 pagesEpidemilogy Measurment MethodsKailash NagarNo ratings yet
- Women &mental HealthDocument16 pagesWomen &mental HealthDhAiRyA ArOrANo ratings yet
- Treatment Aspects in Perioperative NursingDocument51 pagesTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- Case Study 2Document37 pagesCase Study 2api-391842100No ratings yet
- ICDS Scheme ExplainedDocument59 pagesICDS Scheme ExplainedRamniwasMahoreNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- National Health Programs for Cardiovascular and Respiratory ConditionsDocument7 pagesNational Health Programs for Cardiovascular and Respiratory ConditionsJyoti singhNo ratings yet
- Certificate in Paediatric Nursing: ProgrammeDocument67 pagesCertificate in Paediatric Nursing: ProgrammeWOne WannNo ratings yet
- National Health Programmes For Children in IndiaDocument79 pagesNational Health Programmes For Children in IndiashahnazNo ratings yet
- A Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiDocument4 pagesA Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Seminar On Fluid-and-Electrolyte-ImbalanceDocument35 pagesSeminar On Fluid-and-Electrolyte-Imbalancemohamad dildarNo ratings yet
- Nephro Case StudyDocument26 pagesNephro Case Studyanimesh pandaNo ratings yet
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 pagesRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaNo ratings yet
- Overview of India's Revised National Tuberculosis Control ProgrammeDocument65 pagesOverview of India's Revised National Tuberculosis Control Programmecatalyst1986100% (1)
- Journal Club PresentationDocument1 pageJournal Club Presentationmelancholia98No ratings yet
- ENT Nursing Care GuideDocument32 pagesENT Nursing Care GuideabdulNo ratings yet
- Newborn Osce Checklist: A. For StudentsDocument2 pagesNewborn Osce Checklist: A. For Studentsshubham vermaNo ratings yet
- TB MeningitisDocument17 pagesTB MeningitisSylvan LaminaNo ratings yet
- CTG Booklet: A Quick Reference Guide For Managing CtgsDocument16 pagesCTG Booklet: A Quick Reference Guide For Managing Ctgscirlce:twoworldsconnectedNo ratings yet
- Job Description of Nursing OfficerDocument12 pagesJob Description of Nursing OfficerPunam DuwalNo ratings yet
- India's Growing Cervical Cancer EpidemicDocument54 pagesIndia's Growing Cervical Cancer EpidemicJetty Elizabeth JoseNo ratings yet
- Baby Friendly Hospital InitiativeDocument38 pagesBaby Friendly Hospital InitiativeSudhir SinghNo ratings yet
- PLACENTA CLINICAL ASSESSMENT GUIDEDocument18 pagesPLACENTA CLINICAL ASSESSMENT GUIDEAbi RajanNo ratings yet
- Standard Precautions PolicyDocument8 pagesStandard Precautions PolicyMasrov TukirovNo ratings yet
- Pathophysiology On ArrhythmiaDocument34 pagesPathophysiology On ArrhythmiaYhr Yh100% (1)
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Dca NewDocument5 pagesDca NewOm Prakash SinghNo ratings yet
- Indian NavyDocument1 pageIndian NavyOm Prakash SinghNo ratings yet
- Project Report On: Centre For Examination Accredited "A" Grade by NaacDocument1 pageProject Report On: Centre For Examination Accredited "A" Grade by NaacOm Prakash SinghNo ratings yet
- Sr. No. Student Name Father Name Roll No.-Guide NameDocument3 pagesSr. No. Student Name Father Name Roll No.-Guide NameOm Prakash SinghNo ratings yet
- Personal DetailsDocument1 pagePersonal DetailsOm Prakash SinghNo ratings yet
- CISFDocument1 pageCISFOm Prakash SinghNo ratings yet
- Certificate of Surveyed Institution: Vinod Tiwari B.Sc. (Hon's) VI Sem. Has Visited OurDocument3 pagesCertificate of Surveyed Institution: Vinod Tiwari B.Sc. (Hon's) VI Sem. Has Visited OurOm Prakash SinghNo ratings yet
- A Project Report ON: Online Examination SystemDocument4 pagesA Project Report ON: Online Examination SystemOm Prakash SinghNo ratings yet
- Water Level Indicator PDFDocument4 pagesWater Level Indicator PDFKeith brylleNo ratings yet
- Construction of Automatic Water Level Controller For Both Overhead and Underground TanksDocument70 pagesConstruction of Automatic Water Level Controller For Both Overhead and Underground Tanksmyhomenet119188125% (4)
- Automatic Water Level Indicator: March 2016Document5 pagesAutomatic Water Level Indicator: March 2016Om Prakash SinghNo ratings yet
- Origin and Evolution of Chordates: Source: Zoological Science, 18 (4) : 447-464 Published By: Zoological Society of JapanDocument19 pagesOrigin and Evolution of Chordates: Source: Zoological Science, 18 (4) : 447-464 Published By: Zoological Society of JapanOm Prakash SinghNo ratings yet
- DynamoDocument25 pagesDynamoOm Prakash SinghNo ratings yet
- Review of Literature 3. Materials and Methods 4. Results and Analysis 5. Conclusion 6. ReferenceDocument60 pagesReview of Literature 3. Materials and Methods 4. Results and Analysis 5. Conclusion 6. ReferenceOm Prakash SinghNo ratings yet
- Ek (Kuyky Fo"Ofo - Ky Hkksiky E0Iz0 : Vksiu CQD I/Nfr Ds VRXZR 2019&20 MRRJ I''Bksa Ds Izfke I''B DK Izk:IDocument3 pagesEk (Kuyky Fo"Ofo - Ky Hkksiky E0Iz0 : Vksiu CQD I/Nfr Ds VRXZR 2019&20 MRRJ I''Bksa Ds Izfke I''B DK Izk:IOm Prakash SinghNo ratings yet
- Arpit 2Document7 pagesArpit 2Om Prakash SinghNo ratings yet
- Entrepreneurship Exam QuestionsDocument1 pageEntrepreneurship Exam QuestionsOm Prakash SinghNo ratings yet
- 15 Page Document SampleDocument17 pages15 Page Document SampleOm Prakash SinghNo ratings yet
- Agro Bacterium 02Document20 pagesAgro Bacterium 02Om Prakash SinghNo ratings yet
- Declaration: Industry in Municipal Corporation Rewa" Prepared by Me Is MyDocument6 pagesDeclaration: Industry in Municipal Corporation Rewa" Prepared by Me Is MyOm Prakash SinghNo ratings yet
- Vo/Ks"K Izrki Flag Fo"Ofo - Ky Jhok E0Iz0 Vksiu CQD I/Nfr Ds VRXZR 2019&20 MRRJ I''Bksa Ds Izfke I''B DK Izk:IDocument3 pagesVo/Ks"K Izrki Flag Fo"Ofo - Ky Jhok E0Iz0 Vksiu CQD I/Nfr Ds VRXZR 2019&20 MRRJ I''Bksa Ds Izfke I''B DK Izk:IOm Prakash SinghNo ratings yet
- Transfer RNADocument11 pagesTransfer RNAOm Prakash SinghNo ratings yet
- SolutionDocument11 pagesSolutionOm Prakash SinghNo ratings yet
- VolleyballDocument4 pagesVolleyballOm Prakash SinghNo ratings yet
- Meaning of YogaDocument29 pagesMeaning of YogaOm Prakash SinghNo ratings yet
- OogenesisDocument10 pagesOogenesisOm Prakash SinghNo ratings yet
- 02Document4 pages02Om Prakash SinghNo ratings yet
- Analysis of the Autonomous System Network TopologyDocument4 pagesAnalysis of the Autonomous System Network TopologyOm Prakash SinghNo ratings yet
- Bore WellDocument4 pagesBore WellOm Prakash SinghNo ratings yet
- Summary of IMCI Case ManagementDocument2 pagesSummary of IMCI Case Managementjanesky09100% (1)
- In-Vitro Toxicity Assessment of Antimalarial Drugs On Cultured Embryonic Rat Neurons, Macrophage (RAW 264.7), and Kidney Cells (VERO - CCl-81)Document1 pageIn-Vitro Toxicity Assessment of Antimalarial Drugs On Cultured Embryonic Rat Neurons, Macrophage (RAW 264.7), and Kidney Cells (VERO - CCl-81)WUSA9 TVNo ratings yet
- KV Ambernath student's biology project on causes, symptoms and diagnosis of AIDSDocument39 pagesKV Ambernath student's biology project on causes, symptoms and diagnosis of AIDSROHIT SIHRANo ratings yet
- Ebm JurnalDocument198 pagesEbm Jurnalcamelia musaadNo ratings yet
- NHP Jugal KishoreDocument1,015 pagesNHP Jugal KishoreStefiSundaranNo ratings yet
- Lesson 39Document10 pagesLesson 39Sambili TonnyNo ratings yet
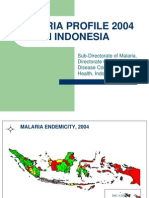
- Malaria Profile and Control Strategies in Indonesia 2004Document40 pagesMalaria Profile and Control Strategies in Indonesia 2004FerdinanNo ratings yet
- Padlet Lesson PlanDocument4 pagesPadlet Lesson Planapi-273579197No ratings yet
- Makalah Keracunan Pestisida (English)Document38 pagesMakalah Keracunan Pestisida (English)iraNo ratings yet
- TOK Essay Rough DraftDocument3 pagesTOK Essay Rough DraftannieNo ratings yet
- Communicablediseaseqa 140829080936 Phpapp02Document20 pagesCommunicablediseaseqa 140829080936 Phpapp02Keiarah Kath Estrada CallaoNo ratings yet
- The Interagency Emergency Health Kit 2011Document72 pagesThe Interagency Emergency Health Kit 2011Cesar Del CastilloNo ratings yet
- What Is Malaria PDFDocument6 pagesWhat Is Malaria PDFtisya f raminNo ratings yet
- Factors Associated With Malaria in Pregnancy Among Women Attending Fort Portal Regional Referral Hospital in Fort Portal City, Western UgandaDocument10 pagesFactors Associated With Malaria in Pregnancy Among Women Attending Fort Portal Regional Referral Hospital in Fort Portal City, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Malaria Treatment TableDocument9 pagesMalaria Treatment Tableاحمد عرفاتNo ratings yet
- A Review On Natural Coagulants in Wastewater TreatmentDocument13 pagesA Review On Natural Coagulants in Wastewater Treatmentahsanur shuvoNo ratings yet
- MODEL SEIRS PENYAKIT MALARIA DENGAN VAKSINASI (38Document47 pagesMODEL SEIRS PENYAKIT MALARIA DENGAN VAKSINASI (38Yuni ArifaNo ratings yet
- ParasitologyDocument27 pagesParasitologyDreyden HaloNo ratings yet
- Health10 - q3 - Mod4 - Adopting Global Health Initiatives To Local or National ContextDocument16 pagesHealth10 - q3 - Mod4 - Adopting Global Health Initiatives To Local or National ContextMark GutangNo ratings yet
- Ethiopia End of Spray Report 2019 Pmi VectorlinkDocument80 pagesEthiopia End of Spray Report 2019 Pmi VectorlinkSamir AwolNo ratings yet
- Four Types of FeversDocument26 pagesFour Types of Feversi210034 Khunsha SalehNo ratings yet
- New Langiage Leader UpperInt StudentbookDocument10 pagesNew Langiage Leader UpperInt StudentbookKeith BrightNo ratings yet
- 2019 November HighlightedDocument76 pages2019 November HighlightedBanana Q100% (4)
- MalariaDocument29 pagesMalariarhimineecat71No ratings yet
- FORMAT LAPORAN MALARIA BARU DinasDocument5 pagesFORMAT LAPORAN MALARIA BARU DinasNoenoeNo ratings yet
- Diagnostic Report: PreliminaryDocument3 pagesDiagnostic Report: Preliminaryekta agarwalNo ratings yet
- JOURNAL READING AnesDocument109 pagesJOURNAL READING AnesIntan AliNo ratings yet
- MSP 3Document15 pagesMSP 3Arunaditya Deshmukh (Adi)No ratings yet
- ALAMIME Call For Applications - Cohort 2 - ENDocument2 pagesALAMIME Call For Applications - Cohort 2 - ENKasozi BakulumpagiNo ratings yet
- Ucmi Newsletter September/october 2023Document5 pagesUcmi Newsletter September/october 2023UCMISTPNo ratings yet