You might also like
- Dermatomes and Myotomes of LLDocument30 pagesDermatomes and Myotomes of LLو عجلت اليك ربي لترضيNo ratings yet
- Medical AbbreviationDocument13 pagesMedical AbbreviationRaf Luis100% (1)
- Mobile Blood DonationDocument10 pagesMobile Blood DonationChristine ApoloNo ratings yet
- Psych 36 Traumatic Brain Injury Lecture SlidesDocument23 pagesPsych 36 Traumatic Brain Injury Lecture SlidesJennifer Isom SchmidtkeNo ratings yet
- Functional organization of the cardiovascular systemDocument19 pagesFunctional organization of the cardiovascular systemIbtesam Mohammed100% (2)
- StrokeDocument16 pagesStrokeFahmi AbdullaNo ratings yet
- IvdpDocument89 pagesIvdpFelix SabuNo ratings yet
- Cervical PainDocument15 pagesCervical Painsteffiecruz06No ratings yet
- Spinal Cord Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSpinal Cord Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Physiotherapy For Parkinsons DiseaseDocument19 pagesPhysiotherapy For Parkinsons Diseasesurender_singh_43No ratings yet
- Traumatic Brain Injury ThesisDocument34 pagesTraumatic Brain Injury Thesisafisher4297100% (1)
- The Klinghardt Neurotoxin Elimination ProtocolDocument14 pagesThe Klinghardt Neurotoxin Elimination Protocolddmorar486100% (3)
- Stroke RehabilitationDocument43 pagesStroke RehabilitationHashini Vjkmr100% (4)
- Hand and Upper Extremity Review for NBCOT ExamDocument59 pagesHand and Upper Extremity Review for NBCOT ExamJenny RajanNo ratings yet
- Stroke RehabilitationDocument59 pagesStroke Rehabilitationnukareva100% (1)
- Neurological Manifestations of Vascular DementiaDocument5 pagesNeurological Manifestations of Vascular DementiaDumitruAuraNo ratings yet
- Mrs - Neriza G. Mamasabulod, RN, MANDocument26 pagesMrs - Neriza G. Mamasabulod, RN, MANNess G. MamasabulodNo ratings yet
- Cervical RadiculopathyDocument181 pagesCervical RadiculopathyE=MC2100% (2)
- Stroke RehabDocument51 pagesStroke RehabchillycrabNo ratings yet
- What Is A Physiatrist PowerpointDocument17 pagesWhat Is A Physiatrist PowerpointsirniravNo ratings yet
- Genu Recurvatum SyndromDocument7 pagesGenu Recurvatum SyndromRoxana RascaNo ratings yet
- Brunnstrom Approach to Stroke RehabilitationDocument32 pagesBrunnstrom Approach to Stroke RehabilitationTalha ParkarNo ratings yet
- 2012-04-24 FK PainDocument49 pages2012-04-24 FK PainYanis Widhiya NingrumNo ratings yet
- Assessment of Back Pain-BMJDocument30 pagesAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNo ratings yet
- Musculoskeletal TraumaDocument103 pagesMusculoskeletal TraumaJona Kristin EnclunaNo ratings yet
- Therapeutic Exercise Foundations and Techniques 5th Ed Part3Document88 pagesTherapeutic Exercise Foundations and Techniques 5th Ed Part3Alice GiffordNo ratings yet
- Stoke Rehabilitation NICE GuidelinesDocument591 pagesStoke Rehabilitation NICE GuidelinesHardeep Singh BaliNo ratings yet
- Rehabilitation of Spinal Cord InjuriesDocument10 pagesRehabilitation of Spinal Cord InjuriesShl Kapre100% (1)
- Stroke RehabilitationDocument10 pagesStroke RehabilitationPethuel Pomaloy100% (1)
- Radicular SyndromeDocument40 pagesRadicular Syndromeainulhawa89No ratings yet
- Diff Diag PDFDocument16 pagesDiff Diag PDFDana Ysabelle IbarraNo ratings yet
- Balance and Vestibular Rehabilitation: Presented By: Neha Tabbassum Khan M.P.T. 1 Yr (Neuro)Document25 pagesBalance and Vestibular Rehabilitation: Presented By: Neha Tabbassum Khan M.P.T. 1 Yr (Neuro)Vidya VenkitaramanNo ratings yet
- Different Orthotic Management of Stroke & Brain Injury Patients With Its Biomechanical Efficiency - DevadriDocument34 pagesDifferent Orthotic Management of Stroke & Brain Injury Patients With Its Biomechanical Efficiency - DevadriDevadri DeyNo ratings yet
- CVAD For NursesDocument54 pagesCVAD For NursesRitaLakhaniNo ratings yet
- Exercise After Stroke GuidelinesDocument67 pagesExercise After Stroke GuidelinesMTEMEINo ratings yet
- EU Physiotherapy Guideline For Parkinson's DiseaseDocument29 pagesEU Physiotherapy Guideline For Parkinson's DiseaseAulia Zerlinda SyihabNo ratings yet
- How to use an incentive spirometer for COPDDocument19 pagesHow to use an incentive spirometer for COPDKoleen KirstenNo ratings yet
- Rancho Los Amigos ScaleDocument3 pagesRancho Los Amigos ScaleYnez PolisticoNo ratings yet
- Rehabilitation Protocol For ACLDocument9 pagesRehabilitation Protocol For ACLgb tradeNo ratings yet
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care PlanJasonlee Baluyot100% (2)
- 50 Item Medical-Surgical Nursing Practice TestDocument13 pages50 Item Medical-Surgical Nursing Practice TestReymund Timog TalarocNo ratings yet
- Final Stroke MBDocument79 pagesFinal Stroke MBVanessa Yvonne GurtizaNo ratings yet
- Role of Physiotherapy in Neurological RehabilitationDocument17 pagesRole of Physiotherapy in Neurological RehabilitationMaheen AnwaarNo ratings yet
- A. D. TBI, Rehabilitation of Traumatic Brain InjuryDocument68 pagesA. D. TBI, Rehabilitation of Traumatic Brain InjuryRupali Raut100% (1)
- Typhoid FeverDocument44 pagesTyphoid FeverLoreth Aurea OjastroNo ratings yet
- Full Guideline PDF 4538466253Document243 pagesFull Guideline PDF 4538466253RizqiKholifaturrahmyNo ratings yet
- A Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Anders Holtz MD PHD, Richard Levi MD PhD-Spinal Cord Injury (2010)Document328 pagesAnders Holtz MD PHD, Richard Levi MD PhD-Spinal Cord Injury (2010)Mikki MoriNo ratings yet
- Bladder and Bowel Dysfunction in SCI Patients: Management StrategiesDocument45 pagesBladder and Bowel Dysfunction in SCI Patients: Management StrategiesAbbas JafarzadehabbasNo ratings yet
- An 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearDocument8 pagesAn 8 Week Scapular Stabilization Exercise Program in An Elite Archer With Scapular Dyskinesis Presenting Joint Noise A Case Report With One YearAmbrogio Orsini100% (1)
- Medical Emergencies in Rehabilitation MedicineDocument24 pagesMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- Designing Motivational Games For Stroke RehabilitationDocument6 pagesDesigning Motivational Games For Stroke RehabilitationSudipta PradhanNo ratings yet
- Low Back Pain Presentation IMPDocument114 pagesLow Back Pain Presentation IMPrapannika100% (3)
- Neurogenic BowlDocument21 pagesNeurogenic BowlFaridatul IsniyahNo ratings yet
- Cauda Equina and Conus Medullaris Syndromes Clinical PresentationDocument9 pagesCauda Equina and Conus Medullaris Syndromes Clinical PresentationhoneyworksNo ratings yet
- Lec 3 Definition of PhysioDocument18 pagesLec 3 Definition of PhysioBhargav100% (1)
- Dr. M. FaheemDocument28 pagesDr. M. FaheemSuganya BalachandranNo ratings yet
- 6 - Lumbar Disc HerniationDocument24 pages6 - Lumbar Disc HerniationHADI BADWANNo ratings yet
- Scales To Assess Gross Motor Function in Stroke Patients: A Systematic ReviewDocument10 pagesScales To Assess Gross Motor Function in Stroke Patients: A Systematic ReviewAngie TarazonaNo ratings yet
- SPONDYLOLISTHESISDocument46 pagesSPONDYLOLISTHESISJino Alex100% (1)
- Pre-Prosthetic Rehabilitation Involving Strength and Positional TDocument13 pagesPre-Prosthetic Rehabilitation Involving Strength and Positional TditaNo ratings yet
- Stroke RehabDocument20 pagesStroke Rehabapi-214830806No ratings yet
- Pain Management in the Elderly: A ReviewDocument9 pagesPain Management in the Elderly: A ReviewDara Agusti MaulidyaNo ratings yet
- Pulmonary Rehabilitation ExercisesDocument28 pagesPulmonary Rehabilitation ExercisesAdrian AlzNo ratings yet
- Butler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialDocument12 pagesButler's Neuromobilizations Combined With Proprioceptive Neuromuscular Facilitation Are Effective in Reducing of Upper Limb Sensory in Late-Stage Stroke Subjects: A Three-Group Randomized TrialCarmen Menaya FernandezNo ratings yet
- Cervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension HeadachesDocument10 pagesCervicogenic Headache Diagnosis and Symptoms Compared to Migraine and Tension Headachespuchio100% (1)
- 5 6323480972671058006Document195 pages5 6323480972671058006Anonymous QOCn5dNo ratings yet
- Hemispatial Neglect LDHDocument20 pagesHemispatial Neglect LDHAldersleyNo ratings yet
- Rotator Cuff Assessment PDFDocument11 pagesRotator Cuff Assessment PDFMichele MarengoNo ratings yet
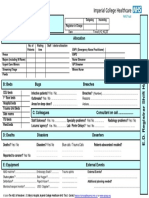
- ABC of Hand Over SheetDocument1 pageABC of Hand Over SheetDiahNiatiNo ratings yet
- The Abc of Handover: E.D. Registrar A: Areas AllocationDocument1 pageThe Abc of Handover: E.D. Registrar A: Areas AllocationDiahNiatiNo ratings yet
- Balut Bidai: (Luthfi Fauzy Asriyanto)Document63 pagesBalut Bidai: (Luthfi Fauzy Asriyanto)DiahNiatiNo ratings yet
- Rajapakse Dengue ShockDocument9 pagesRajapakse Dengue ShockrantiadrianiNo ratings yet
- Lampiran LeafletDocument1 pageLampiran LeafletDiahNiatiNo ratings yet
- Jurnal Maternitas Fix 3Document5 pagesJurnal Maternitas Fix 3DiahNiatiNo ratings yet
- Hand Hygiene To Reduce Ispa TransmissionDocument12 pagesHand Hygiene To Reduce Ispa TransmissionDiahNiatiNo ratings yet
- 2014 AHA-ACC-HRS Guidelines For The Management of Patients With Atrial Fibrillation PDFDocument76 pages2014 AHA-ACC-HRS Guidelines For The Management of Patients With Atrial Fibrillation PDFEvi Furi AmaliaNo ratings yet
- Jurnal Maternitas Fix 3Document5 pagesJurnal Maternitas Fix 3DiahNiatiNo ratings yet
- A PDFDocument5 pagesA PDFDiahNiatiNo ratings yet
- Upaya Peningkatan Pengetahuan Ketrampilan MasyDocument10 pagesUpaya Peningkatan Pengetahuan Ketrampilan MasyDeddy KhairulNo ratings yet
- Upaya Peningkatan Pengetahuan Ketrampilan MasyDocument10 pagesUpaya Peningkatan Pengetahuan Ketrampilan MasyDeddy KhairulNo ratings yet
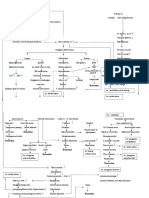
- Pathway DMDocument2 pagesPathway DMDiahNiatiNo ratings yet
- WawancaraDocument8 pagesWawancaraDiahNiatiNo ratings yet
- Logo UbDocument1 pageLogo UbDiahNiatiNo ratings yet
- Repair Cherry Eye in DogsDocument11 pagesRepair Cherry Eye in DogsPambudiNo ratings yet
- Drug Study On PpudDocument3 pagesDrug Study On PpudLezelle Mandane CardinoNo ratings yet
- PHILIPPINE PHYSICIAN LICENSURE EXAMINATION (PLE): A PRIMER FOR SUCCESSDocument43 pagesPHILIPPINE PHYSICIAN LICENSURE EXAMINATION (PLE): A PRIMER FOR SUCCESSChoi SpeaksNo ratings yet
- Rehabilitation Medicine Standards to Protect PatientsDocument13 pagesRehabilitation Medicine Standards to Protect PatientsCobi EstacioNo ratings yet
- Anemia - Ferrum MetDocument6 pagesAnemia - Ferrum MetManali JainNo ratings yet
- Occupational Therapy Rehabilitation Paraplegic PatientDocument7 pagesOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNo ratings yet
- Acetaminophen Suppository Mechanism of Action Side Effects Nursing ResponsibilitiesDocument2 pagesAcetaminophen Suppository Mechanism of Action Side Effects Nursing ResponsibilitiesNiziu BearsNo ratings yet
- Ankylosed Teeth As Abutments For Maxillary Protraction: A Case ReportDocument5 pagesAnkylosed Teeth As Abutments For Maxillary Protraction: A Case Reportdrgeorgejose7818No ratings yet
- Case Log DefinitionsDocument6 pagesCase Log DefinitionsSarah DNo ratings yet
- COVID-19 Infodemic Study Analyzes Virus Naming and Social ContagionDocument10 pagesCOVID-19 Infodemic Study Analyzes Virus Naming and Social Contagionvivitri.dewiNo ratings yet
- Choledochal CystDocument68 pagesCholedochal CystSyed Waqas HasanNo ratings yet
- Label The Diagram of The HeartDocument1 pageLabel The Diagram of The HeartMarie HutsonNo ratings yet
- Implementation of The Filmarray Me Panel in Laboratory Routine Using A Simple Sample Selection Strategy For Diagnosis of Meningitis and EncephalitisDocument9 pagesImplementation of The Filmarray Me Panel in Laboratory Routine Using A Simple Sample Selection Strategy For Diagnosis of Meningitis and EncephalitisMohinish SNo ratings yet
- Biomedical Technology Lecture Notes 2015Document11 pagesBiomedical Technology Lecture Notes 2015Phi NguyenNo ratings yet
- Ancaman Global Kesehatan Dan Finansial Di Era MDRODocument29 pagesAncaman Global Kesehatan Dan Finansial Di Era MDROYusuf AjaNo ratings yet
- OrthodonticDocument3 pagesOrthodonticFirma Nurdinia DewiNo ratings yet
- Biology 12 Unit 9 Assignment 2 Blood Type and Immune Response Virtual LabDocument2 pagesBiology 12 Unit 9 Assignment 2 Blood Type and Immune Response Virtual Labapi-3385788740% (1)
- Jose RDocument17 pagesJose RMineTagraNo ratings yet
- Prevention and Treatment of COVID-19 in Elderly People: September 2020Document8 pagesPrevention and Treatment of COVID-19 in Elderly People: September 2020Dra. Adialys Guevara GonzalezNo ratings yet