You might also like
- Rotator Cuff Assessment PDFDocument11 pagesRotator Cuff Assessment PDFMichele MarengoNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Time Code Title Author: Date: 30-07-2021Document4 pagesTime Code Title Author: Date: 30-07-2021siddhartha senNo ratings yet
- Mobilization and Stimulation of Neuromuscular Tissue (MaSoNT)From EverandMobilization and Stimulation of Neuromuscular Tissue (MaSoNT)No ratings yet
- Walking AidsDocument38 pagesWalking AidsMurad KurdiNo ratings yet
- Walking Aids KinesiologyDocument26 pagesWalking Aids Kinesiologyfarwafurqan1No ratings yet
- Pathomechanics of Structural Foot Deformities NotesDocument1 pagePathomechanics of Structural Foot Deformities NotesMorgan LeeNo ratings yet
- Exercise For Impaired BalanceDocument43 pagesExercise For Impaired BalanceGildarts KunNo ratings yet
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- Tos PDFDocument12 pagesTos PDFDiana ChirilăNo ratings yet
- Rehab Hamstring InjuriesDocument9 pagesRehab Hamstring InjuriesPascu MariusNo ratings yet
- ICUDocument12 pagesICUNabilahNo ratings yet
- Restricted Ankle Dorsiflexion: Methods To Assess and Improve Joint FunctionDocument9 pagesRestricted Ankle Dorsiflexion: Methods To Assess and Improve Joint FunctionJorge Lucas JimenezNo ratings yet
- Range of Motion Exercises With PhotosDocument12 pagesRange of Motion Exercises With PhotosSherly L WaromiNo ratings yet
- Malignant Spinal Cord Compression - Dealing The Most Common - MetsDocument60 pagesMalignant Spinal Cord Compression - Dealing The Most Common - MetsDr Sasikumar Sambasivam100% (2)
- Examine Cervical Spine Range MotionDocument16 pagesExamine Cervical Spine Range MotionlecturioNo ratings yet
- Hemispatial Neglect LDHDocument20 pagesHemispatial Neglect LDHAldersleyNo ratings yet
- Cardio Pulmonary AssessmentDocument8 pagesCardio Pulmonary AssessmentSHAIK SHABEENANo ratings yet
- 2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDocument3 pages2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDi CanNo ratings yet
- Department of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017Document24 pagesDepartment of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017aritrisnawatiNo ratings yet
- HydrotherapyDocument21 pagesHydrotherapy7e9oo90% (1)
- Activacion AbdominalDocument7 pagesActivacion AbdominalArmandoRiosNo ratings yet
- Stroke Rehab, Info Proving PNF To Improve Upper Limb Function - FullDocument6 pagesStroke Rehab, Info Proving PNF To Improve Upper Limb Function - FullThomas CorbettNo ratings yet
- The Hamstrings Anatomic and Physiologic Variations and Their Potential Relationships With Injury RiskDocument22 pagesThe Hamstrings Anatomic and Physiologic Variations and Their Potential Relationships With Injury RiskHugo TintiNo ratings yet
- Shoulder Impingement GuidelinesDocument3 pagesShoulder Impingement GuidelinesTasha MillerNo ratings yet
- Knee BiomechanicsDocument32 pagesKnee BiomechanicsnishantsinghbmeNo ratings yet
- Orthosisofhandppt 181202162551Document65 pagesOrthosisofhandppt 181202162551Khageswar SamalNo ratings yet
- Knee Biomechanics: Mark Arthur Martinez Trauma 1 April 5, 2018Document7 pagesKnee Biomechanics: Mark Arthur Martinez Trauma 1 April 5, 2018Juan Alvaro EstradaNo ratings yet
- Baseline Bubble Inclinometer User ManualDocument2 pagesBaseline Bubble Inclinometer User Manualphcproducts100% (2)
- Clinical Examination of The Sacroiliac JointDocument7 pagesClinical Examination of The Sacroiliac Jointthe_walnutNo ratings yet
- Introductio To OrthoticsDocument8 pagesIntroductio To OrthoticsGopi Krishnan100% (1)
- Grade 4 Chondromalacia Patella TreatmentDocument3 pagesGrade 4 Chondromalacia Patella TreatmentTroy0% (1)
- Joint Range of Motion Assessment GuideDocument16 pagesJoint Range of Motion Assessment GuideAlice Gifford100% (1)
- Ijspt-Biomechanics and Pathomechanics of The Patellofemoral JointDocument11 pagesIjspt-Biomechanics and Pathomechanics of The Patellofemoral JointDevi MigiekaNo ratings yet
- Rehabilitation: Walking After Total Knee ReplacementDocument10 pagesRehabilitation: Walking After Total Knee ReplacementSandeep DhimanNo ratings yet
- GWS Total Hip ReplacementDocument17 pagesGWS Total Hip ReplacementRadu MoglanNo ratings yet
- Jurnal Frozen ShoulderDocument21 pagesJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNo ratings yet
- Muscle Grading and Testing ProceduresDocument5 pagesMuscle Grading and Testing Proceduresshodhganga100% (1)
- Running Gait AnalysisDocument24 pagesRunning Gait Analysisapi-339139744No ratings yet
- Poster PresentationDocument1 pagePoster PresentationAayat KhanNo ratings yet
- Shoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFDocument31 pagesShoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFRulyNo ratings yet
- Restore Scapula Control for Thoracic Outlet SyndromeDocument10 pagesRestore Scapula Control for Thoracic Outlet Syndromercastello20No ratings yet
- Low Back Pain Presentation IMPDocument114 pagesLow Back Pain Presentation IMPrapannika100% (3)
- Tennis Elbow PDFDocument2 pagesTennis Elbow PDFSabau PetreNo ratings yet
- SPONDYLOLISTHESISDocument46 pagesSPONDYLOLISTHESISJino Alex100% (1)
- De Quervain SyndromeDocument5 pagesDe Quervain Syndromebangla018No ratings yet
- Biomechanics of MovementDocument17 pagesBiomechanics of Movements_chandrubioNo ratings yet
- Lower Limb Orthosis Types and UsesDocument44 pagesLower Limb Orthosis Types and UsesRakesh shahNo ratings yet
- ApproachDocument37 pagesApproachAshu AshNo ratings yet
- Home Exercise Program: Hands On TherapyDocument10 pagesHome Exercise Program: Hands On TherapyCatrinel ȘupialăNo ratings yet
- Gait in Children With Cerebral PalsyDocument5 pagesGait in Children With Cerebral PalsyvarahamihirNo ratings yet
- SCI Acute Care and Rehabilitation PT 2009Document265 pagesSCI Acute Care and Rehabilitation PT 2009api-3822828No ratings yet
- Clinical Biomechanics of Gait: OutlineDocument7 pagesClinical Biomechanics of Gait: Outlinechacho1971100% (1)
- Gait BiomechDocument77 pagesGait BiomechVidhya anand MNo ratings yet
- Bio Mechanics and Motor Control of Human Movement 4editionDocument13 pagesBio Mechanics and Motor Control of Human Movement 4editionStanko.Stuhec8307100% (2)
- KMC Dept of Orthopaedics Floor Reaction OrthosisDocument5 pagesKMC Dept of Orthopaedics Floor Reaction OrthosischinmayghaisasNo ratings yet
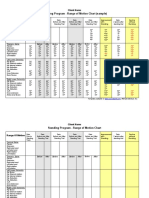
- Standing Program - Range of Motion Chart (Sample) : Client NameDocument2 pagesStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNo ratings yet
- SpondylosisDocument3 pagesSpondylosisNovia Diba100% (1)
- Trauma 1 ShoulderDocument61 pagesTrauma 1 ShoulderDr Abdallah BahaaNo ratings yet
- Rotator Cuff TearsDocument5 pagesRotator Cuff TearsdrjorgewtorresNo ratings yet
- Pathomechanics of the Shoulder: Factors, Causes, EffectsDocument27 pagesPathomechanics of the Shoulder: Factors, Causes, EffectsVenkat RamanaNo ratings yet
- The Source of Shoulder Pain in Hemiplegia: Robert L. Joynt, MDDocument5 pagesThe Source of Shoulder Pain in Hemiplegia: Robert L. Joynt, MDSahithya MNo ratings yet
- Hip Bone Marrow Edema Presenting As Low Back Pain A Case ReportDocument10 pagesHip Bone Marrow Edema Presenting As Low Back Pain A Case ReportVizaNo ratings yet
- 1.20 (Surgery) Orthopedics Sports - PediatricsDocument8 pages1.20 (Surgery) Orthopedics Sports - PediatricsLeo Mari Go LimNo ratings yet
- Hegedus 2012Document16 pagesHegedus 2012jose perezNo ratings yet
- Does Hand Grip Strength Correlate With Shoulder Rotator Cuff FunctionDocument6 pagesDoes Hand Grip Strength Correlate With Shoulder Rotator Cuff FunctionsoylahijadeunvampiroNo ratings yet
- Shoulder Tests: Neer, Hawkins-Kennedy, Drop Arm & MoreDocument5 pagesShoulder Tests: Neer, Hawkins-Kennedy, Drop Arm & MoreYusrah SaniNo ratings yet
- Gian Luigi Canata, Henrique Jones - Epidemiology of Injuries in Sports-Springer (2022)Document157 pagesGian Luigi Canata, Henrique Jones - Epidemiology of Injuries in Sports-Springer (2022)Renan Sequini Favaro100% (1)
- Dirkwinkel Johanna Sophie Mefst 2017 Diplo SveucDocument59 pagesDirkwinkel Johanna Sophie Mefst 2017 Diplo SveucJulenda CintarinovaNo ratings yet
- Intern's Guide to ED OrthopedicsDocument28 pagesIntern's Guide to ED OrthopedicsAmir AliNo ratings yet
- Cools 2008 Screening The Athletes Shoulder ForDocument9 pagesCools 2008 Screening The Athletes Shoulder ForLucyFloresNo ratings yet
- Reinold - Glenohumeral and Scapulothoracic RehabDocument45 pagesReinold - Glenohumeral and Scapulothoracic Rehabshivnair100% (2)
- 01 sports PT MCQsDocument13 pages01 sports PT MCQsayeshamumtazkakakhel322No ratings yet
- Rotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsDocument9 pagesRotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsmatteoNo ratings yet
- Supraspinatus Tendon Pathomechanics: A Current Concepts ReviewDocument12 pagesSupraspinatus Tendon Pathomechanics: A Current Concepts Reviewgia purnamaNo ratings yet
- Ephe 355 Assignment 2 Orrin Parker and AmiraliDocument9 pagesEphe 355 Assignment 2 Orrin Parker and Amiraliapi-541137581No ratings yet
- Dynamic Neuromuscular Stabilization & Sports RehabilitationDocument13 pagesDynamic Neuromuscular Stabilization & Sports RehabilitationHONGJYNo ratings yet
- Clinical Science Anatomy MRCP 1 Pastest 2019 Q BankDocument140 pagesClinical Science Anatomy MRCP 1 Pastest 2019 Q BankRuby BhattyNo ratings yet
- 8 Proses Fisioterpi Anggota Gerak, Temu 8Document61 pages8 Proses Fisioterpi Anggota Gerak, Temu 8oetari putriNo ratings yet
- Rafii Khairuddin Mahfuzh-1810301069-Pr Manipulasi Upper-DikonversiDocument5 pagesRafii Khairuddin Mahfuzh-1810301069-Pr Manipulasi Upper-Dikonversiraden ayu putri suryaniNo ratings yet
- Prentice9e Im Chap18Document6 pagesPrentice9e Im Chap18api-281340024100% (1)
- Uk BakalaurasDocument68 pagesUk BakalaurasAquaNo ratings yet
- Shoulder Joint (MSPT SPT)Document99 pagesShoulder Joint (MSPT SPT)Khushboo IkramNo ratings yet
- Powerpoint Scap. Rehab Ann CoolsDocument9 pagesPowerpoint Scap. Rehab Ann CoolsWalter PelaezNo ratings yet
- Fraktur HumerusDocument9 pagesFraktur Humerusagung pratamaNo ratings yet
- MRI Findings of 26 Patients With Parsonage-Turner SyndromeDocument6 pagesMRI Findings of 26 Patients With Parsonage-Turner SyndromeTopciu Mihaela FeliciaNo ratings yet
- Sindrome Impacto Acta Orto Bras 2011 InglDocument5 pagesSindrome Impacto Acta Orto Bras 2011 InglMichele GonçalvesNo ratings yet