You might also like
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentFrom EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNo ratings yet
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementFrom EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreNo ratings yet
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocument59 pagesWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNo ratings yet
- Sitbat 16item FinalDocument6 pagesSitbat 16item FinalMae NocheNo ratings yet
- Upper Extremity Range of Motion Chart Name: Dob: School Years: Left RightDocument2 pagesUpper Extremity Range of Motion Chart Name: Dob: School Years: Left RightNatasya SetyamartaNo ratings yet
- Classification of Upper Limb OrthosesDocument16 pagesClassification of Upper Limb Orthoseszoha hassanNo ratings yet
- Chapter 10 Upper Extremity Interventions PDFDocument208 pagesChapter 10 Upper Extremity Interventions PDFRonny Méndez VasconcellosNo ratings yet
- Module 10 Upper Extremity FINAL 16edDocument163 pagesModule 10 Upper Extremity FINAL 16edgialinuNo ratings yet
- Design of A Hand OrthosisDocument251 pagesDesign of A Hand OrthosisIsrael BlancoNo ratings yet
- Examine Cervical Spine Range MotionDocument16 pagesExamine Cervical Spine Range MotionlecturioNo ratings yet
- Patterns of Triangular Fibrocartilage Complex (TFCC) Injury Associated WithDocument7 pagesPatterns of Triangular Fibrocartilage Complex (TFCC) Injury Associated WithCésarLópezNo ratings yet
- Muscle Grading and Testing ProceduresDocument5 pagesMuscle Grading and Testing Proceduresshodhganga100% (1)
- Gait in Children With Cerebral PalsyDocument5 pagesGait in Children With Cerebral PalsyvarahamihirNo ratings yet
- Neuro-Developmental Clinical ObservationsDocument2 pagesNeuro-Developmental Clinical ObservationsAmitesh NarayanNo ratings yet
- Neurological ExaminationDocument13 pagesNeurological Examinationsaveetha purushothamanNo ratings yet
- Department of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017Document24 pagesDepartment of Orthopaedic and Traumatology Faculty of Medicine - Hasanuddin University Makassar 2017aritrisnawatiNo ratings yet
- Cardio Pulmonary AssessmentDocument8 pagesCardio Pulmonary AssessmentSHAIK SHABEENANo ratings yet
- Hemispatial Neglect LDHDocument20 pagesHemispatial Neglect LDHAldersleyNo ratings yet
- SCALE-Selective Control Assesment PDFDocument3 pagesSCALE-Selective Control Assesment PDFjinil raj j.r.No ratings yet
- Hanger PDRDocument63 pagesHanger PDRTetay JavierNo ratings yet
- Physiotherapy Assessment for CP ChildrenDocument5 pagesPhysiotherapy Assessment for CP ChildrenAnonymous cCy8GpNo ratings yet
- Walking AidsDocument38 pagesWalking AidsMurad KurdiNo ratings yet
- Prosthetic Case PresentationsDocument19 pagesProsthetic Case PresentationsptannenbaumNo ratings yet
- De Quervain SyndromeDocument5 pagesDe Quervain Syndromebangla018No ratings yet
- Lateral Epicondylitis - Tennis Ellbow HandoutDocument5 pagesLateral Epicondylitis - Tennis Ellbow Handoutgermany23No ratings yet
- Shoulder Impingement GuidelinesDocument3 pagesShoulder Impingement GuidelinesTasha MillerNo ratings yet
- Tennis Elbow PDFDocument2 pagesTennis Elbow PDFSabau PetreNo ratings yet
- Guide to Ankle Foot Orthoses (AFOsDocument2 pagesGuide to Ankle Foot Orthoses (AFOsAbdul Razzaq AfridiNo ratings yet
- Pediatrics FracturesDocument14 pagesPediatrics Fracturesخالد الغامديNo ratings yet
- Pediatric SplintingDocument51 pagesPediatric SplintingNathalie Michelle HenriquezNo ratings yet
- Foot and Ankle ArthrokinematicsDocument6 pagesFoot and Ankle ArthrokinematicsCraig StewartNo ratings yet
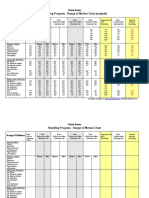
- Standing Program - Range of Motion Chart (Sample) : Client NameDocument2 pagesStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNo ratings yet
- Introductio To OrthoticsDocument8 pagesIntroductio To OrthoticsGopi Krishnan100% (1)
- Exit Project Workbook Complete Draft 2Document2 pagesExit Project Workbook Complete Draft 2vladNo ratings yet
- Proc RangeOfMotionDocument4 pagesProc RangeOfMotionSri KuspartianingsihNo ratings yet
- OT8 - Thumb Immobilization SplintDocument4 pagesOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
- Understanding ACL Injuries and SurgeryDocument38 pagesUnderstanding ACL Injuries and SurgerySzilvia MartonosNo ratings yet
- F16 Stroke Positioning ChartDocument1 pageF16 Stroke Positioning ChartSue Verge0% (1)
- Gmi PDFDocument71 pagesGmi PDFAlma GlinacNo ratings yet
- Splinting and Orthotics JMBDocument48 pagesSplinting and Orthotics JMBRudiyantoNo ratings yet
- September2010 Clinical GuidelinesDocument26 pagesSeptember2010 Clinical GuidelinesFabianinhoLacerdaNo ratings yet
- Evaluation of The Hand!Document84 pagesEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- JOSPT Shoulder Pain and Mobility Deficitis Adhesive Capsulitis PDFDocument33 pagesJOSPT Shoulder Pain and Mobility Deficitis Adhesive Capsulitis PDFAbdul Wahid ShaikhNo ratings yet
- Passive MovementsDocument1 pagePassive MovementsomhreemaimhreemNo ratings yet
- GAIT 2 - Clinical Gait Analysis - HandoutDocument32 pagesGAIT 2 - Clinical Gait Analysis - Handoutj100% (1)
- FIM ManualDocument24 pagesFIM ManualAnshuman MihirNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Spinal Cord InjuryDocument39 pagesSpinal Cord InjuryrahatNo ratings yet
- Cervicothoracic Regional Exam FindingsDocument1 pageCervicothoracic Regional Exam FindingsChristopher NotleyNo ratings yet
- Task-Specific TrainingDocument16 pagesTask-Specific Trainingapi-293223028No ratings yet
- P&O Elementary MathematicsDocument22 pagesP&O Elementary MathematicsrrutayisireNo ratings yet
- Biomechanics & Pathomechanics of HandDocument81 pagesBiomechanics & Pathomechanics of HandAmrita L. Tomar67% (3)
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- Bio Mechanics and Pathomechanics of Ankle JointDocument35 pagesBio Mechanics and Pathomechanics of Ankle Joint56 Vignesh j 079No ratings yet
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- Osteoarthritis 2018Document45 pagesOsteoarthritis 2018Rizcky Naldy Eka PutraNo ratings yet
- Assessing Functional AbilityDocument15 pagesAssessing Functional AbilitySonali Soumyashree100% (2)
- Knee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsDocument36 pagesKnee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsdedsnetNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Wrist Hand OrthosisDocument7 pagesWrist Hand OrthosisKhageswar SamalNo ratings yet
- Reducing Hypertonia in Stroke PatientsDocument3 pagesReducing Hypertonia in Stroke PatientsKhageswar SamalNo ratings yet
- A Structured Overview of Trends and Technologies Used in Dynamic Hand OrthosesDocument25 pagesA Structured Overview of Trends and Technologies Used in Dynamic Hand OrthosesKhageswar SamalNo ratings yet
- Wrist Hand OrthosisDocument1 pageWrist Hand OrthosisKhageswar SamalNo ratings yet
- Electrical Protective Equipment: Fuses, MCBs, ELCBs and Their Working PrinciplesDocument17 pagesElectrical Protective Equipment: Fuses, MCBs, ELCBs and Their Working PrinciplesKhageswar SamalNo ratings yet
- IVDP: Inter Vertebral Disc ProlapseDocument34 pagesIVDP: Inter Vertebral Disc ProlapseShibinNo ratings yet
- Journal Reading-DM Hennie Bertha O-16711067Document56 pagesJournal Reading-DM Hennie Bertha O-16711067Suwandi BaskoroNo ratings yet
- The Knee and The Cruciate Ligaments Anatomy Biomechanics Clinical Aspects Reconstruction Complications Rehabilitation by H.-U. Stäubli, R. P. Jakob (Auth.), Prof. Dr. R. P. Jakob, PD Dr. H.-U. StäuDocument633 pagesThe Knee and The Cruciate Ligaments Anatomy Biomechanics Clinical Aspects Reconstruction Complications Rehabilitation by H.-U. Stäubli, R. P. Jakob (Auth.), Prof. Dr. R. P. Jakob, PD Dr. H.-U. StäuemilNo ratings yet
- Calypso Knee SystemDocument14 pagesCalypso Knee Systemapi-467445554No ratings yet
- Lower Limb BlocksDocument5 pagesLower Limb BlocksParvathy R NairNo ratings yet
- Consent To Surgery/Anaesthesia: Ilocos Sur Provincial Hospital-Gabriela SilangDocument1 pageConsent To Surgery/Anaesthesia: Ilocos Sur Provincial Hospital-Gabriela SilangRyrey Abraham PacamanaNo ratings yet
- Nursing Notes for Mrs. Dee's Pre-Op AnxietyDocument1 pageNursing Notes for Mrs. Dee's Pre-Op AnxietyIrish Eunice FelixNo ratings yet
- EB05 Electrosurgical Generator FeaturesDocument1 pageEB05 Electrosurgical Generator FeaturesViviana Albornoz100% (1)
- How To Avoid Varus Stem in THRDocument6 pagesHow To Avoid Varus Stem in THRPoliceNo ratings yet
- How Dutch Hospitals Make Value-Based Health Care WorkDocument24 pagesHow Dutch Hospitals Make Value-Based Health Care WorkElik MəmmədovNo ratings yet
- Nathalia Gouin Resume For SchoolDocument2 pagesNathalia Gouin Resume For Schoolapi-529657256No ratings yet
- Nonunions: Dr. Ivan Wong July 19, 2006Document20 pagesNonunions: Dr. Ivan Wong July 19, 2006Ega NoristaNo ratings yet
- IPSG GoalslDocument10 pagesIPSG GoalsljebashanthiniNo ratings yet
- Hip Fracture Programme: A Guide For Patients Following SurgeryDocument20 pagesHip Fracture Programme: A Guide For Patients Following SurgeryDruga DanutNo ratings yet
- Kenneth A - Dubaj: Objective EducationDocument1 pageKenneth A - Dubaj: Objective Educationapi-508681333No ratings yet
- Test Bank For Introductory Medical Surgical Nursing 10th Edition Barbara TimbyDocument8 pagesTest Bank For Introductory Medical Surgical Nursing 10th Edition Barbara Timbycoopeeglottishe6y1No ratings yet
- Multiloop PDFDocument10 pagesMultiloop PDFAstrid Carolina HerreraNo ratings yet
- Preoperative Nursing Care ExplainedDocument3 pagesPreoperative Nursing Care ExplainedJmarie Brillantes PopiocoNo ratings yet
- Atlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFDocument795 pagesAtlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFOanaDavid100% (3)
- Anatomical Landmark PPT. TGL 25Document7 pagesAnatomical Landmark PPT. TGL 25Pink MeNo ratings yet
- Posterior Capsular CalcificationDocument4 pagesPosterior Capsular CalcificationNurulSyaidahNo ratings yet
- PIL Paliganj PatnaDocument8 pagesPIL Paliganj PatnaVishal Kumar SinghNo ratings yet
- PPNLISTDocument64 pagesPPNLISTvramkrishnNo ratings yet
- Chapter 43: Musculoskeletal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument4 pagesChapter 43: Musculoskeletal Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Product Catalog 2015: Implants & InstrumentationsDocument16 pagesProduct Catalog 2015: Implants & Instrumentationsjangum herminayogyaNo ratings yet
- SINGLE BOUGIE AND DOUBLE TUBE TECHNIQUE'-A NOVEL APPROACH TO DIFFICULT NASAL INTUBATIONDocument1 pageSINGLE BOUGIE AND DOUBLE TUBE TECHNIQUE'-A NOVEL APPROACH TO DIFFICULT NASAL INTUBATIONRavikiran SuryanarayanamurthyNo ratings yet
- NJR 19th Annual Report 2022Document374 pagesNJR 19th Annual Report 2022JD2750No ratings yet
- Emergency Medical Care Libro CAp 1Document19 pagesEmergency Medical Care Libro CAp 1Angel ArreolaNo ratings yet
- Guidelines For Hospital Regarding Claim Prepration For Payment Clearance - SSPDocument1 pageGuidelines For Hospital Regarding Claim Prepration For Payment Clearance - SSPumayrh@gmail.comNo ratings yet
- Course Title Book Author Publisher Isbn: Chatterjea, M. N Shinde, Rana Brothers Medical PubDocument8 pagesCourse Title Book Author Publisher Isbn: Chatterjea, M. N Shinde, Rana Brothers Medical PubhdthhhhNo ratings yet