Professional Documents
Culture Documents
Metanálisis en Red BRAF MT 2017 PDF
Uploaded by
CARLOS DURANOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Metanálisis en Red BRAF MT 2017 PDF
Uploaded by
CARLOS DURANCopyright:
Available Formats
Research
JAMA Oncology | Original Investigation
Systemic Therapy for Previously Untreated Advanced
BRAF-Mutated Melanoma
A Systematic Review and Network Meta-Analysis
of Randomized Clinical Trials
Tahira Devji, BSc; Oren Levine, MD; Binod Neupane, PhD; Joseph Beyene, PhD; Feng Xie, PhD
Supplemental content
IMPORTANCE Multiple effective first-line systemic treatment options are available for patients
with advanced BRAF-mutated melanoma. A lack of head-to-head randomized clinical trials
(RCTs) comparing targeted and immunotherapies leaves uncertainty regarding optimal
first-line treatment.
OBJECTIVE To estimate the relative efficacy and safety of systemic therapies for advanced,
treatment-naive, BRAF-mutated melanoma.
DATA SOURCES We searched MEDLINE, Embase, and the Cochrane Central Registry of
Controlled Trials for phase 2 or 3 RCTs published up until April 29, 2016.
STUDY SELECTION We included RCTs in which at least 1 intervention was a targeted (BRAF or
MEK) or an immune checkpoint (cytotoxic T-lymphocyte–associated antigen 4 [CTLA-4] or
programmed cell death 1 [PD-1]) inhibitor.
DATA EXTRACTION AND SYNTHESIS Two reviewers performed study selection, data
abstraction, and risk of bias assessment. We performed a Bayesian network meta-analysis
using a fixed-effect model to combine direct comparisons with indirect evidence. We
estimated hazard ratios (HRs) for overall survival (OS) and progression-free survival (PFS),
and odds ratios (OR) for objective response rate (ORR) and serious adverse events.
RESULTS Sixteen eligible articles reporting 15 RCTs involving 6662 patients assigned to 1 of 10
treatment strategies were included. Both BRAF/MEK and PD-1 were associated with improved
OS benefit compared with all other treatments except CTLA-4/granulocyte macrophage
colony-stimulating factor. There was no significant difference in OS between BRAF/MEK and
PD-1 (HR, 1.02; 95% credible interval [CrI], 0.72-1.45). The network meta-analysis showed a
significant advantage of BRAF/MEK compared with all other treatment strategies for PFS.
BRAF/MEK was associated with higher ORR (OR, 2.00; 95% CrI, 1.64-2.45) compared with
BRAF alone, with both being superior in achieving ORR compared with other treatments.
Chemotherapy and PD-1 were associated with lowest risk of serious adverse events. There
was no significant difference in the risk of serious adverse events between chemotherapy and
PD-1 (OR, 1.00; 95% CrI, 0.74-1.34). Author Affiliations: Department of
Clinical Epidemiology & Biostatistics,
McMaster University, Hamilton,
CONCLUSIONS AND RELEVANCE Compared with other treatments, BRAF/MEK and PD-1 Ontario, Canada (Devji, Levine,
inhibition significantly improved OS. The favorable safety profile of PD-1 inhibitors supports Neupane, Beyene, Xie); Department
of Oncology, McMaster University,
using this option as first-line therapy in circumstances where rapid response is not a priority.
Hamilton, Ontario, Canada (Levine);
Father Sean O’Sullivan Research
Centre, St Joseph’s
Healthcare-Hamilton, Hamilton,
Ontario, Canada (Xie).
Corresponding Author: Feng Xie,
PhD, Department of Clinical
Epidemiology & Biostatistics,
McMaster University, 50 Charlton
Ave E, Rm H306 Martha Wing,
JAMA Oncol. doi:10.1001/jamaoncol.2016.4877 Hamilton L8N 4A6 (fengxie
Published online October 27, 2016. @mcmaster.ca).
(Reprinted) E1
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Research Original Investigation Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma
C
utaneous melanoma is an aggressive and deadly form
of skin cancer. Incidence rates of melanoma have Key Points
rapidly risen over the last 30 years with an annual in-
Question What is the relative efficacy and safety of systemic
crease of 3% to 7% worldwide.1,2 Early stage melanoma is of- therapies for advanced, treatment-naive, BRAF-mutated
ten cured with surgery alone; however, most patients present- melanoma?
ing with advanced-stage disease are not candidates for surgical
Findings In this systematic review and network meta-analysis,
resection and thus systemic therapy is the main treatment mo-
BRAF/MEK and programmed cell death protein 1 (PD-1) inhibition
dality. Prognosis for patients with unresectable or metastatic were associated with improved overall survival benefit compared
melanoma is poor, with a 5-year survival rate of 24% to 29% with all treatments except cytotoxic T-lymphocyte–associated
and 10% to 19% for patients with stage IIIC and IV disease, antigen 4/granulocyte macrophage colony–stimulating factor.
respectively.3 Until recently, treatment options were limited There was no significant difference in overall survival between
for advanced disease. Multiple developments in understand- BRAF/MEK and PD-1; BRAF/MEK conferred a significant advantage
over all other treatments for progression-free survival;
ing the molecular mechanisms of melanoma oncogenesis and
chemotherapy and PD-1 were associated with lowest risk of
immune evasion have revolutionized the standard of care for serious adverse events, with no significant difference in risk
patients with advanced melanoma. between treatments.
The mitogen-activated protein (MAP) kinase signaling
Meaning The favorable efficacy and safety profile of PD-1
pathway is an important mediator of cell proliferation and dif-
inhibitors supports using this option as first-line therapy.
ferentiation in melanoma.4,5 Approximately 40% to 60% of cu-
taneous melanomas harbor a mutation in the BRAF gene that
leads to constitutive activation of downstream signaling notherapy (eTable 1 in the Supplement). We limited our search
through the MAP kinase pathway.6,7 In addition, immune to randomized clinical trials (RCTs) by applying a filter devel-
checkpoint inhibitors including cytotoxic T-lymphocyte– oped by the Health Information Research Unit at McMaster
associated antigen 4 (CTLA-4) and programmed cell death pro- University.27 There were no language or date restrictions made.
tein 1 (PD-1) have been identified as key coregulatory mol- We manually searched the reference lists of included studies
ecules responsible for down-regulation of T-cell activation.8-10 and consulted with experts to search for additional studies.
Targeted therapies, including selective BRAF and MEK in-
hibitors, have drastically improved rates of progression-free Study Selection
survival (PFS) and overall survival (OS) in patients with meta- We included phase 2 or 3 RCTs that met the following criteria:
static melanoma harboring a BRAF V600 mutation.11-15 Im- (1) the study enrolled treatment-naive adult patients with un-
mune checkpoint inhibitors have also shown significant ben- resectable lymph node metastasis (American Joint Commit-
efit over conventional chemotherapies in randomized trials,16-21 tee on Cancer [AJCC] TNM Stage IIIC) or distant metastatic
regardless of BRAF mutation status.18,22,23 Thus, in the case (AJCC TNM stage IV) melanoma; (2) at least 1 of the interven-
of advanced BRAF-mutated melanoma, multiple effective tions compared in the trial was either a targeted (BRAF or MEK)
first-line treatment options are available. No head-to-head ran- or an immune checkpoint (CTLA-4 or PD-1) inhibitor; and (3)
domized trials of targeted agents and immunotherapies have the study reported on at least 1 of the following outcomes: OS,
been conducted, and thus the optimal treatment is un- PFS, objective response rate (ORR), and/or serious adverse
known. Our aim was to systematically review the literature and events (SAEs) defined as greater than or equal to grade 3 ac-
determine the relative efficacy and safety of systemic treat- cording to the National Cancer Institute Common Terminol-
ment options for advanced BRAF-mutated melanoma in the ogy Criteria for Adverse Events.28
first-line setting. To obtain the estimates of relative treat- Although our population of interest is BRAF-mutated mela-
ment effects for all possible comparisons, we employed a net- noma, we did not restrict study eligibility by BRAF mutation
work meta-analysis (NMA) technique, which simultaneously status. Targeted therapies (BRAF or MEK inhibitors) have gen-
integrates direct evidence from head-to-head trials and indi- erally been studied in a selected population of patients with
rect evidence (relative treatment effects between 2 treat- tumors harboring the mutation of interest. Immunothera-
ments derived from a common comparator).24,25 pies (CTLA-4 or PD-1 inhibitors) have been studied either in a
mixed population or in a BRAF wild-type population. Based
on proven efficacy of immunotherapy in melanoma regard-
less of BRAF mutation status,18,22,23 these treatments have be-
Methods come important options even for the BRAF-mutated cancers.
Literature Search To generate a comprehensive network of trials comparing all
We conducted this study according to the methods outlined treatment options of current clinical relevance, it was neces-
in the Cochrane Handbook for Systematic Reviews of sary to capture immunotherapy trials. Hence, we were inclu-
Interventions.26 MEDLINE, EMBASE, and Cochrane Central sive of trials irrespective of the BRAF mutation status.
Registry of Controlled Trials (CENTRAL) were systematically Two reviewers (T.D. and O.L.) independently screened
searched from inception up to and including April 29, 2016. titles and abstracts in duplicate, obtained full texts of articles
Search terms included extensive controlled vocabulary (MeSH that either reviewer considered potentially eligible, and de-
and EMTREE) in various combinations, supplemented with termined eligibility from the full texts independently and in
keywords including melanoma, targeted therapy, and immu- duplicate. All discrepancies were resolved by consensus or with
E2 JAMA Oncology Published online October 27, 2016 (Reprinted) jamaoncology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma Original Investigation Research
a third adjudicator (F.X.). Interobserver agreement for the re- surface under the cumulative ranking curve (SUCRA) for each.35
viewers’ assessments of study eligibility was calculated with The SUCRA index ranges between 0 (or 0%) and 1 (or 100%),
the Cohen κ coefficient of agreement. where the treatments with highest and lowest SUCRA are con-
sidered to be the best and worst treatments, respectively.
Data Extraction and Risk of Bias Assessment We combined different drugs of the same class within a
The same 2 reviewers used a pilot-tested, standardized form to single treatment category, which may have introduced hetero-
independently extract information from each eligible study. Data geneity in our NMA. In the trial by Ribas et al,36 tremeli-
regarding study and population characteristics, as well as treat- mumab, a fully human monoclonal antibody against CTLA-4,
ments and outcomes (PFS, OS, ORR, and SAEs) were ab- did not show significant benefit for OS over chemotherapy. This
stracted. For PFS and OS, we extracted the hazard ratio (HR) and trial is discordant with results of ipilimumab, a similar CTLA-
confidence interval (CI) when available. When HRs and corre- 4-directed molecule. Tremelimumab was administered ev-
sponding CIs were not reported, we estimated them by recon- ery 90 days, and based on early progression most patients re-
structing individual patient data from published Kaplan- ceived only 1 dose.36 At the time, risk of pseudo-progression
Meier cur ves with methods desc ribed by Guyot and and immune-related response criteria had not been well
colleagues.29 Authors of included studies were contacted if im- established.37 The dosing schedule and early discontinuation
portant data were unclear or not reported. For multiple reports of treatment may have limited the benefit of tremelimumab.38
of the same trial, we used longest follow-up data for analysis. We performed a sensitivity analysis excluding this trial from
Risk of bias of individual studies was assessed independently the network to determine the impact of combining results for
by the reviewers (T.D. and O.L.) using the Cochrane Collabora- both CTLA-4 agents.
tion risk-of-bias tool,26 and interrater agreement was calcu- Network meta-analysis was performed in WinBUGS soft-
lated by weighted κ.30,31 Any disagreements were resolved by ware (version 1.4.3, MRC Biostatistics Unit) interfacing through
consensus. R software.
Data Synthesis and Analysis
Given the limited number of RCTs for any individual treat-
ment, we categorized therapies by drug class: targeted therapy
Results
(BRAF, MEK, combined BRAF and MEK [BRAF/MEK]), immu- Study Characteristics
notherapy (CTLA-4, PD-1, CTLA-4/PD-1), chemotherapy, and Of the 2546 citations identified through our literature search
combinations of these treatment groups (MEK/CHEMO, CTLA- (1848 after duplicates were removed), 1750 were deemed in-
4/CHEMO, CTLA-4/granulocyte macrophage colony– eligible after title and abstract screening, leaving 98 studies
stimulating factor [GM-CSF]). We synthesized evidence for 4 plus 1 identified from the relevant article search for full-text
outcomes: PFS, OS, ORR, and any SAEs. For each outcome, we review (eFigure 1 in the Supplement). Sixteen eligible publi-
performed a Bayesian NMA using a Markov Chain Monte Carlo cations reporting 15 RCTs12-15,17,18,20,36,39-45 were included in
(MCMC) simulation technique with 100 000 iterations in each the review and NMA (eTable 2 in the Supplement). Overall
of the 4 chains. Noninformative priors (ie, N[0, 10000]) were agreement between the 2 reviewers for final eligibility was ex-
chosen for the effect parameters. The analysis was per- cellent (κ = 0.87;, 95% CI, 0.79-0.94).
formed under the fixed-effect model, as only 1 trial provided eTable 2 in the Supplement summarizes the characteris-
direct evidence for most of the treatment comparisons. How- tics of the 15 RCTs involving 6662 patients. All studies were
ever, a random-effects (RE) model was also performed as sen- multicenter (13 conducted internationally) and published be-
sitivity analysis and model fits were compared using devi- tween 2011 and 2015. Five RCTs17,18,20,41,44 focused on both pa-
ance information criteria (DIC).32 In the comparison of any 2 tients with BRAF mutations and wild-type tumors, 2 RCTs39,44
models, we deemed a better fit model if its DIC was less than on patients with wild-type tumors only, 6 RCTs12-15,42,43 on pa-
the DIC of the other model by at least 5. Heterogeneity in the tients with BRAF mutations, and 2 trials36,40 did not specify
network was assessed with the Cochrane Q (χ2) test and quan- the BRAF status. Ten treatment strategies were compared. No
tified using the I2 statistic within each pairwise comparison RCTs directly compared immunotherapies with targeted thera-
when 2 or more trials were available for the comparison.33 Be- pies; eFigure 2 in the Supplement provides the network
cause it was uncommon to have both direct and indirect evi- geometries for all 4 outcomes.
dence for most comparisons in our networks, we assumed co-
herence for our analysis (ie, direct and indirect evidence, when Quality of Evidence
both available for a given comparison, were statistically simi- The overall risk of bias was low and agreement between re-
lar). To test the robustness of this assumption we used the viewers in this assessment was excellent (κ = 0.90; 95% CI,
node-splitting method to assess whether there was incoher- 0.80-0.96). The detailed risk of bias assessment can be found
ence in any closed loops.32,34 in eFigure 3 in the Supplement. For all outcomes, most of the
Relative effects of treatments are reported as HR for sur- direct treatment comparisons had only 1 trial providing evi-
vival outcomes (PFS and OS) and odds ratio (OR) for binary dence; hence heterogeneity was not estimable for such
outcomes (ORR and SAEs) along with corresponding 95% cred- comparisons. We found minimal heterogeneity (I2 = 0%) in all
ible intervals (CrIs), the Bayesian equivalent of 95% CIs. We direct comparisons with 2 or more trials in the OS and PFS net-
estimated the overall ranks of treatments by calculating the works. However, heterogeneity was detected for the PD-1/
jamaoncology.com (Reprinted) JAMA Oncology Published online October 27, 2016 E3
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Research Original Investigation Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma
CTLA-4 vs CTLA-4 comparison (I2 = 51%, 2 trials) in the ORR BRAF/MEK is likely the best treatment in achieving an
network, and for the BRAF/MEK vs BRAF comparison objective response (SUCRA: 100%) followed by BRAF
(I2 = 88%, 2 trials) in the SAEs network. The fit of the fixed- (SUCRA: 87%) and PD-1/CTLA-4 (SUCRA: 75%) (eTable 3 in
effect model was similar or better than that of RE model in the the Supplement). Sensitivity analysis with the removal of
OS, PFS and ORR networks. Although the RE model was a bet- the Ribas et al36 trial did not affect the results of our pri-
ter fit for the SAEs network, 8 of 9 direct comparisons each had mary analysis.
just 1 trial, hence heterogeneity was driven entirely by the com-
parison of BRAF/MEK vs BRAF from just 2 trials. Therefore, Serious Adverse Events
the fixed-effect model was a practical choice for analysis of all Only 8 trials (4395 patients) comparing 8 treatment strategies
outcomes including SAEs. reported adverse events of grade 3 or higher (eFigure 2D in the
Supplement). Rates of SAEs ranged from 38.4% for chemo-
Overall Survival therapy to 68.7% for CTLA-4/PD-1 (eTable 4 in the Supple-
Thirteen trials (5361 patients) comparing 9 treatments were in- ment). As shown in eTable 5 in the Supplement, chemo-
cluded in the OS analysis (eFigure 2A in the Supplement). We therapy and PD-1 were associated with lowest risk of SAEs
obtained extended follow-up (5-year) data of 1 trial20 from a compared with all other treatments. There was no significant
second publication.46 Both BRAF/MEK and PD-1 were associ- difference in the risk of SAEs between chemotherapy and PD-1
ated with improved OS benefit compared with all other treat- (OR, 1.00; 95% CrI, 0.74-1.34). Among the immunothera-
ments except CTLA-4/GM-CSF (key comparisons include pies, CTLA-4/PD-1 was associated with higher risk of SAEs
BRAF/MEK vs BRAF: HR, 0.69; 95% CrI, 0.59-0.82 and PD-1 compared with CTLA-4 (OR, 1.63; 95% CrI, 1.19-2.26) and
vs CTLA-4: HR, 0.58; 95% CrI, 0.47-0.71) (Figure, A). There was PD-1 (OR, 2.99; 95% CrI, 2.18-4.12). Among the targeted
no significant difference in OS between BRAF/MEK and PD-1 therapies, BRAF/MEK was associated with lower risk of
(HR, 1.02; 95% CrI, 0.72-1.45). The SUCRA values of 92% and SAEs compared with BRAF (OR, 0.84; 95% CrI, 0.66-1.06).
90% for BRAF/MEK and PD-1, respectively, suggested that The SUCRA analysis suggested that chemotherapy and PD-1
these were the 2 treatments with the highest chance of im- had the lowest risk of SAEs with SUCRA values of 93%
proving OS in advanced melanoma (eTable 3 in the Supple- (eTable 3 in the Supplement).
ment). The sensitivity analysis by removing the Ribas et al36
trial resulted in a ranking order with PD-1 higher than BRAF/
MEK, SUCRA of 93% and 84%, respectively. The analysis of this
outcome does not include CTLA-4/PD-1 because OS data are
Discussion
awaited from landmark trials. Until recently, therapeutic options for patients with ad-
vanced melanoma were limited, and the prognosis was guarded
Progression-Free Survival at best. With the advent of targeted therapies and immune
Fourteen trials (6738 patients) comparing 10 treatments were checkpoint inhibitors, the treatment landscape has changed
included in the PFS analysis (eFigure 2B in the Supplement). dramatically, complicating decision making for patients and
The results of NMA showed a significant advantage of BRAF/ clinicians. In this systematic review and NMA focusing on tar-
MEK compared with all other treatment strategies for PFS geted and immunotherapies for treatment-naive patients with
(Figure, B). Overall, PD-1/CTLA-4 showed a significant im- advanced BRAF-mutated melanoma, we found that BRAF/
provement in PFS compared with PD-1 alone (HR, 0.75; 95% MEK and PD-1 inhibitors showed significant survival benefit
CrI, 0.62-0.91) and all other treatments except BRAF/MEK (HR, over all other treatments with the only exception of CTLA-4/
1.49; 95% CrI, 1.03-2.18). For PFS, BRAF/MEK was most likely GM-CSF therapy where there was no difference in OS. In our
the best treatment (SUCRA: 100%), followed by PD-1/CTLA-4 primary and sensitivity analyses of OS, there was no statisti-
(SUCRA: 87%) and BRAF (SUCRA: 78%), whereas MEK was least cally significant difference between BRAF/MEK and PD-1 in-
likely to be the best treatment strategy (SUCRA: 7%) (eTable 3 hibitors. We therefore conclude that these treatment strate-
in the Supplement). gies should be considered equivalent with respect to survival
benefit based on current evidence. A caveat in interpreting our
Objective Response Rate analysis is the lack of OS data for CTLA-4/PD-1. The combina-
Thirteen trials (5580 patients) comparing 9 treatment strat- tion immunotherapy shows promise in early outcomes and
egies were included in the ORR analysis (eFigure 2C in the could change the treatment landscape once longer-term re-
Supplement). As shown in Figure, C, BRAF/MEK was associ- sults are published.
ated with a higher ORR compared with BRAF alone (OR, Only 1 randomized phase 2 trial addressed CTLA-4/GM-
2.00; 95% CrI, 1.64-2.45); both treatments, however, con- CSF treatment showing an OS benefit with the addition of sar-
ferred a significant improvement in ORR compared with all gramostim to ipilimumab. There is potential synergy be-
other interventions included in the network (BRAF/MEK vs tween GM-CSF (which augments antigen presentation) and
PD-1/CTLA-4 OR, 0.26; 95% CrI 0.14-0.48). Among the CTLA4 inhibition (which promotes T-cell proliferation) in im-
immunotherapies, PD-1/CTLA-4 was associated with higher mune response. Additionally, reduced toxic effects with the
ORR when compared with PD-1 alone (OR, 1.82; 95% CrI, combination compared to CTLA-4 monotherapy likely con-
1.34-2.47), which in turn was better than CTLA-4 (with or tributes to improved survival. Further phase 3 evidence will
without chemotherapy). The SUCRA analysis suggested that be required to confirm the efficacy of this therapy.40
E4 JAMA Oncology Published online October 27, 2016 (Reprinted) jamaoncology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma Original Investigation Research
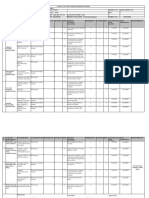
Figure. Pooled Estimates for All Possible Treatment Effects for Each Outcome
A Overall survival
BRAF
0.69
BRAF/MEK
(0.59-0.82)
1.22 1.76
CTLA-4
(0.94-1.58) (1.29-2.40)
0.99 1.43 0.81
CTLA-4/CHEMO
(0.75-1.32) (1.03-2.00) (0.64-1.05)
0.90 1.31 0.74 0.91
CTLA-4/GM-CSF
(0.50-1.64) (0.70-2.43) (0.44-1.26) (0.51-1.64)
1.94 2.81 1.59 1.96 2.15
MEK
(1.29-2.92) (1.80-4.37) (1.08-2.34) (1.31-2.92) (1.12-4.13)
1.47 2.12 1.20 1.47 1.62 0.75
MEK/CHEMO
(0.96-2.26) (1.33-3.36) (0.80-1.80) (0.97-2.26) (0.83-3.15) (0.45-1.27)
0.71 1.02 0.58 0.71 0.78 0.36 0.48
PD-1
(0.52-0.96) (0.72-1.45) (0.47-0.71) (0.53-0.96) (0.44-1.38) (0.24-0.55) (0.31-0.75)
1.44 2.08 1.18 1.45 1.59 0.74 0.98 2.04
CHEMO
(1.17-1.77) (1.59-2.71) (1.01-1.38) (1.19-1.76) (0.92-2.76) (0.52-1.06) (0.68-1.42) (1.62-2.57)
B Progression-free survival
BRAF
0.58
BRAF/MEK
(0.51-0.66)
2.13 3.65
CTLA-4
(1.52-2.97) (2.56-5.21)
2.05 3.52 0.96
CTLA-4/CHEMO
(1.58-2.66) (2.63-4.71) (0.68-1.36)
2.19 3.76 1.03 1.07
CTLA-4/GM-CSF
(1.30-3.69) (2.19-6.44) (0.69-1.54) (0.63-1.82)
2.89 4.96 1.36 1.41 1.32
MEK
(1.99-4.17) (3.34-7.32) (0.88-2.09) (0.96-2.07) (0.73-2.39)
1.84 3.15 0.86 0.90 0.84 0.64
MEK/CHEMO
(1.27-2.66) (2.13-4.68) (0.56-1.33) (0.61-1.31) (0.46-1.52) (0.40-1.01)
1.16 1.99 0.55 0.57 0.53 0.40 0.63
PD-1
(0.86-1.57) (1.44-2.76) (0.48-0.63) (0.41-0.77) (0.35-0.82) (0.27-0.61) (0.42-0.96)
0.87 1.49 0.41 0.42 0.40 0.30 0.98 0.75 PD-1/CTL A-4
(0.61-1.24) (1.03-2.18) (0.34-0.49) (0.29-0.61) (0.26-0.62) (0.19-0.47) (0.30-0.75) (0.62-0.91)
2.70 4.63 1.27 1.32 1.23 0.93 1.47 2.32 3.11 CHEMO
(2.27-3.20) (3.73-5.74) (0.95-1.69) (1.08-1.60) (0.75-2.03) (0.67-1.30) (1.06-2.04) (1.81-2.98) (2.26-4.25)
C Objective response rate
BRAF
2.00
BRAF/MEK
(1.64-2.45)
0.08 0.04
CTLA-4
(0.05-0.14) (0.02-0.07)
0.11 0.05 1.35
CTLA-4/CHEMO
(0.06-0.21) (0.03-0.11) (0.70-2.65)
0.04 0.02 0.50 0.37
MEK
(0.01-0.13) (0.01-0.07) (0.15-1.58) (0.11-1.24)
0.16 0.08 1.95 1.45 3.89
MEK/CHEMO
(0.07-0.35) (0.03-0.18) (0.90-4.36) (0.60-3.49) (1.08-15.01)
0.28 0.14 3.54 2.62 7.03 1.82
PD-1
(0.16-0.49) (0.08-0.25) (2.59-4.86) (1.35-5.08) (2.24-23.68) (0.81-3.97)
0.52 0.26 6.45 4.77 12.82 3.30 1.82
PD-1/CTLA-4
(0.28-0.94) (0.14-0.48) (4.67-8.94) (2.37-9.57) (3.99-43.88) (1.44-7.50) (1.34-2.47)
0.07 0.03 0.87 0.64 1.72 0.44 0.24 0.13
CHEMO
(0.05-0.10) (0.02-0.05) (0.59-1.28) (0.37-1.09) (0.58-5.47) (0.22-0.88) (0.17-0.36) (0.09-0.21)
Effect estimates reflect comparison of the treatment in the row heading being compared to the column heading. Overall survival and progression-free survival are
presented with hazard ratios. Objective response rates (C) are presented with odds ratios. Numbers in parentheses are 95% credible intervals. Chemo indicates
chemotherapy; CTLA-4, cytotoxic T-lymphocyte–associated antigen 4; GM-CSF, granulocyte macrophage colony–stimulating factor; PD-1, programmed cell death
protein 1.
jamaoncology.com (Reprinted) JAMA Oncology Published online October 27, 2016 E5
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Research Original Investigation Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma
BRAF/MEK inhibition was most effective with respect to geted and immunotherapies in our network, making
PFS followed by CTLA-4/PD-1 inhibition. Unlike OS, PFS is comparison impossible. Some reports suggest BRAF muta-
not influenced by crossover or postprogression therapies. tion may be a negative prognostic indicator.49,50 In our NMA,
Yet, given the variability in response patterns using studies that included BRAF wild-type tumors were predomi-
immunotherapies,37 PFS may be less robust as an outcome nantly immunotherapy trials. The indirect comparisons could
measure in this setting. therefore be biased by prognostic differences in study popu-
Survival benefit must be balanced against risk of toxic ef- lations. However, evidence regarding the prognostic impor-
fects. In the setting of advanced disease, systemic treatment tance of BRAF status in advanced melanoma is mixed,51 and
is noncurative for most, and thus quality of life is a priority. the influence on our analysis is uncertain.
Rates of SAEs were high for all treatment strategies with the We classified treatments by mechanism of action. This re-
exception of PD-1 inhibitors, which showed no increased risk sulted in a concise network often with multiple trials contrib-
compared with chemotherapy. Among immunotherapies, uting to a comparison between 2 treatment categories. We feel
CTLA-4/PD-1 was associated with a significantly increased this is more informative compared with an alternate design in
risk of toxic effects compared with either monotherapy. which each drug is considered separately yielding a very sparse
Each immune checkpoint inhibitor activates T cells by a network. The inclusion of various drugs within a single net-
unique mechanism, and to see higher rates of immune- work node is a potential source of heterogeneity, although sig-
related toxic effects is expected with the combination. With nificant heterogeneity was not detected or not assessable for
respect to targeted therapy, BRAF/MEK was less toxic than most direct comparisons.
BRAF monotherapy. This is consistent with results of pri-
mary trials and reflects the BRAF-inhibitor–induced para- Limitations
doxical activation of the MAP kinase pathway, which causes Our analysis is limited by sparse networks for all outcomes.
skin-related toxic effects, including secondary cutaneous Imprecise estimates of treatment effects are likely even when
malignancy.47,48 the magnitude of the estimates are important since direct
Our analysis of ORR showed best results with BRAF/MEK evidence for each network was limited. Most direct compari-
inhibition. This supports first-line use of combination tar- sons were based on evidence from a single trial, and around
geted therapy for patients with bulky or highly symptomatic three-fourths of all treatment comparisons were derived
disease, when rapid reduction in tumor volume is necessary from indirect evidence alone, which must be considered
to improve health status. This may also influence choice of when making inferences from our study findings. We did not
treatment in the setting of nondisseminated but unresect- suspect indirectness (related to the question or due to transi-
able disease. Our analysis does not address resection rates fol- tivity) because trial populations and study characteristics
lowing use of systemic treatment, thus clinical significance for were very comparable to the target population of our NMA.
locally advanced disease is tentative. Indirect evidence for most comparisons was derived from the
There are several strengths of our study. Our safety analy- common comparator of chemotherapy. Chemotherapy dose
sis helps provide a uniform assessment of risks of toxic ef- and frequency was similar in all trials, so it is reasonable to
fects across treatment categories. An inadequate number of assume transitivity. All networks had an almost star-shaped
trials (n = 4) reported treatment–related adverse events to pro- geometry, and there were no more than 2 closed loops of evi-
vide a meaningful comparison across treatment categories. For dence formed by different independent trials in these net-
a more comprehensive comparison, we analyzed rates of any works. The node splitting analysis did not detect incoherence
SAE. Treatment-related adverse event rate is a clinically rel- in any closed loop. Publication bias could not be formally
evant safety outcome, but the rate of any adverse event is a assessed due to the small number of trials available for direct
more conservative and pragmatic metric. comparisons.
Our analysis is also strengthened by high quality and low
risk of bias in the primary trials. Although the included ran-
domized phase 2 trials offer less precise estimates due to
smaller sample sizes, these studies allow for a comprehen-
Conclusions
sive overview of the current treatment landscape for patients Our systematic review and NMA provides the first compari-
with advanced melanoma. We considered only treatment- son between targeted therapies and immune checkpoint in-
naive patients in an attempt to standardize baseline progno- hibitors for treatment-naive, BRAF-mutated advanced mela-
sis. Moreover, inclusion criteria for primary trials were very nomas. In the absence of a compelling clinical circumstance
similar, producing a homogeneous population for the meta- to guide choice of treatment, it has been unclear which treat-
analysis with the exception of the BRAF status of eligible pa- ment strategy is optimal for patient-important outcomes.
tients. The inclusion of patients with BRAF wild-type tumors Though limited by a sparse network and a lack of OS data for
receiving immunotherapy is justified by the efficacy of im- CTLA-4/PD-1, this analysis provides an evidence-based frame-
mune checkpoint inhibitors regardless of mutation status.17,18,23 work to inform clinical decision making. Our results show that
For trials that included a mixed BRAF population, subgroups OS is best with either PD-1 or combined BRAF/MEK inhibi-
based on mutation status were often not reported. Had we lim- tion. The favorable safety profile of PD-1 inhibitors supports
ited our analysis to patients who were BRAF mutation posi- using this treatment option as first-line therapy in circum-
tive there would be no common reference trial linking tar- stances where rapid response is not a priority.
E6 JAMA Oncology Published online October 27, 2016 (Reprinted) jamaoncology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma Original Investigation Research
ARTICLE INFORMATION 12. Hauschild A, Grob JJ, Demidov LV, et al. 27. Wilczynski NL, McKibbon KA, Haynes RB.
Accepted for Publication: August 30, 2016. Dabrafenib in BRAF-mutated metastatic melanoma: Enhancing retrieval of best evidence for health care
a multicentre, open-label, phase 3 randomised from bibliographic databases: calibration of the
Published Online: October 27, 2016. controlled trial. Lancet. 2012;380(9839):358-365. hand search of the literature. Stud Health Technol
doi:10.1001/jamaoncol.2016.4877 Inform. 2001;84(Pt 1):390-393.
13. Larkin J, Ascierto PA, Dréno B, et al. Combined
Author Contributions: Dr Xie and Ms Devji had full vemurafenib and cobimetinib in BRAF-mutated 28. NCI Common Terminology Criteria for Adverse
access to all the data in the study and take melanoma. N Engl J Med. 2014;371(20):1867-1876. Events (CTCAE) v.4 2010 [April 16, 2016]. http:
responsibility for the integrity of the data and the //evsnci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010
accuracy of the data analysis. 14. Long GV, Stroyakovskiy D, Gogas H, et al.
Dabrafenib and trametinib vs dabrafenib and -06-14_QuickReference_8.5x11.pdf. Accessed
Concept and design: Devji, Levine, Xie. September 21, 2016.
Acquisition, analysis, or interpretation of data: All placebo for Val600 BRAF-mutant melanoma:
Authors. a multicentre, double-blind, phase 3 randomised 29. Guyot P, Ades AE, Ouwens MJ, Welton NJ.
Drafting of the manuscript: Devji, Levine, Neupane. controlled trial. Lancet. 2015;386(9992):444-451. Enhanced secondary analysis of survival data:
Critical revision of the manuscript for important 15. Robert C, Karaszewska B, Schachter J, et al. reconstructing the data from published
intellectual content: All Authors. Improved overall survival in melanoma with Kaplan-Meier survival curves. BMC Med Res Methodol.
Statistical analysis: Devji, Neupane, Beyene, Xie. combined dabrafenib and trametinib. N Engl J Med. 2012;12:9.
Administrative, technical, or material support: Xie. 2015;372(1):30-39. 30. Landis JR, Koch GG. The measurement of
Study supervision: Devji, Xie. 16. Hodi FSOD, O’Day SJ, McDermott DF, et al. observer agreement for categorical data. Biometrics.
Conflict of Interest Disclosures: None reported. Improved survival with ipilimumab in patients with 1977;33(1):159-174.
metastatic melanoma. [Erratum appears in N Engl J 31. Orwin RG. Evaluating coding decisions. In:
REFERENCES Med. 2010 Sep 23;363(13):1290]. N Engl J Med. Cooper H, Hedges LV, eds. The Handbook of
1. Lens MB, Dawes M. Global perspectives of 2010;363(8):711-723. Research Synthesis. New York, NY: Russell Sage
contemporary epidemiological trends of cutaneous 17. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Foundation; 1994:177-200.
malignant melanoma. Br J Dermatol. 2004;150(2): Combined nivolumab and ipilimumab or 32. Higgins J. Identifying and addressing
179-185. monotherapy in untreated melanoma. N Engl J Med. inconsistency in network meta-analysis: Cochrane
2. Little EG, Eide MJ. Update on the current state of 2015;373(1):23-34. comparing multiple interventions methods group
melanoma incidence. Dermatol Clin. 2012;30(3): 18. Postow MA, Chesney J, Pavlick AC, et al. Oxford training event. 2013. http://methods
355-361. Nivolumab and ipilimumab vs ipilimumab in .cochrane.org/cmi/sites/methods.cochrane.org.cmi
untreated melanoma. N Engl J Med. 2015;372(21): /files/uploads/S9-L%20Identifying%20and
3. Survival statistics for melanoma. Toronto, ON: %20addressing%20inconsistency%20in
Canadian Cancer Society; 2015 [July 14, 2014]. 2006-2017.
%20network%20meta-analysis.pdf. Accessed
Available from: http://www.cancer.ca/en/cancer 19. Ribas A, Puzanov I, Dummer R, et al. September 21, 2016.
-information/cancer-type/skin-melanoma Pembrolizumab vs investigator-choice
/prognosis-and-survival/survival-statistics/?region chemotherapy for ipilimumab-refractory melanoma 33. Higgins JP, Thompson SG. Quantifying
=on. (KEYNOTE-002): a randomised, controlled, phase 2 heterogeneity in a meta-analysis. Stat Med. 2002;
trial. Lancet Oncol. 2015;16(8):908-918. 21(11):1539-1558.
4. Grob JJ, Amonkar MM, Martin-Algarra S, et al.
Patient perception of the benefit of a BRAF 20. Robert C, Thomas L, Bondarenko I, et al. 34. Dias S, Welton NJ, Caldwell DM, Ades AE.
inhibitor in metastatic melanoma: quality-of-life Ipilimumab plus dacarbazine for previously Checking consistency in mixed treatment
analyses of the BREAK-3 study comparing untreated metastatic melanoma. N Engl J Med. comparison meta-analysis. Stat Med. 2010;29(7-8):
dabrafenib with dacarbazine. Ann Oncol. 2014;25 2011;364(26):2517-2526. 932-944.
(7):1428-1436. 21. Weber JS, D’Angelo SP, Minor D, et al. 35. Salanti G, Ades AE, Ioannidis JP. Graphical
5. Tsao H, Goel V, Wu H, Yang G, Haluska FG. Nivolumab vs chemotherapy in patients with methods and numerical summaries for presenting
Genetic interaction between NRAS and BRAF advanced melanoma who progressed after results from multiple-treatment meta-analysis: an
mutations and PTEN/MMAC1 inactivation in anti-CTLA-4 treatment (CheckMate 037): overview and tutorial. J Clin Epidemiol. 2011;64(2):
melanoma. J Invest Dermatol. 2004;122(2):337-341. a randomised, controlled, open-label, phase 3 trial. 163-171.
6. Curtin JA, Fridlyand J, Kageshita T, et al. Distinct Lancet Oncol. 2015;16(4):375-384. 36. Ribas A, Kefford R, Marshall MA, et al. Phase III
sets of genetic alterations in melanoma. N Engl J Med. 22. Larkin J, Lao CD, Urba WJ, et al. Efficacy and randomized clinical trial comparing tremelimumab
2005;353(20):2135-2147. safety of nivolumab in patients with BRAF V600 with standard-of-care chemotherapy in patients
mutant and BRAF wild-type advanced melanoma: with advanced melanoma. J Clin Oncol. 2013;31(5):
7. Davies H, Bignell GR, Cox C, et al. Mutations of 616-622.
the BRAF gene in human cancer. Nature. 2002;417 a pooled analysis of 4 clinical trials. JAMA Oncol.
(6892):949-954. 2015;1(4):433-440. 37. Wolchok JDH, Hoos A, O’Day S, et al. Guidelines
23. Shahabi V, Whitney G, Hamid O, et al. for the evaluation of immune therapy activity in
8. O’Day SJ, Hamid O, Urba WJ. Targeting cytotoxic solid tumors: immune-related response criteria. Clin
T-lymphocyte antigen-4 (CTLA-4): a novel strategy Assessment of association between BRAF-V600E
mutation status in melanomas and clinical response Cancer Res. 2009;15(23):7412-7420.
for the treatment of melanoma and other
malignancies. Cancer. 2007;110(12):2614-2627. to ipilimumab. Cancer Immunol Immunother. 2012; 38. Ascierto PA. Is there still a role for
61(5):733-737. tremelimumab in the treatment of cancer? Transl
9. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, Cancer Res. 2013;2(1):48-50.
activity, and immune correlates of anti-PD-1 24. Jansen JP, Crawford B, Bergman G, Stam W.
antibody in cancer. N Engl J Med. 2012;366(26): Bayesian meta-analysis of multiple treatment 39. Gupta A, Love S, Schuh A, et al. DOC-MEK:
2443-2454. comparisons: an introduction to mixed treatment a double-blind randomized phase II trial of
comparisons. Value Health. 2008;11(5):956-964. docetaxel with or without selumetinib in wild-type
10. Wang C, Thudium KB, Han M, et al. In vitro BRAF advanced melanoma. Ann Oncol. 2014;25(5):
characterization of the anti-PD-1 antibody 25. Mills EJ, Ioannidis JP, Thorlund K, Schünemann
HJ, Puhan MA, Guyatt GH. How to use an article 968-974.
nivolumab, BMS-936558, and in vivo toxicology in
non-human primates. Cancer Immunol Res. 2014;2 reporting a multiple treatment comparison 40. Hodi FSL, Lee S, McDermott DF, et al.
(9):846-856. meta-analysis. JAMA. 2012;308(12):1246-1253. Ipilimumab plus sargramostim vs ipilimumab alone
26. Higgins JPT, Green S. Cochrane handbook for for treatment of metastatic melanoma:
11. Chapman PBH, Hauschild A, Robert C, et al; a randomized clinical trial. JAMA. 2014;312(17):
BRIM-3 Study Group. Improved survival with systematic reviews of interventions version 5.1. 0.
[updated March 2011] The Cochrane Collaboration; 1744-1753.
vemurafenib in melanoma with BRAF V600E
mutation. N Engl J Med. 2011;364(26):2507-2516. 2011. 41. Kirkwood JM, Bastholt L, Robert C, et al. Phase
II, open-label, randomized trial of the MEK1/2
jamaoncology.com (Reprinted) JAMA Oncology Published online October 27, 2016 E7
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
Research Original Investigation Therapy for Previously Untreated Advanced BRAF-Mutated Melanoma
inhibitor selumetinib as monotherapy versus advanced melanoma who received ipilimumab plus cutaneous melanoma: an area of ongoing research.
temozolomide in patients with advanced dacarbazine in a phase III trial. J Clin Oncol. 2015;33 Ann Transl Med. 2015;3(2):24.
melanoma. Clin Cancer Res. 2012;18(2):555-567. (10):1191-1196. 52. Atkins MB, Kunkel L, Sznol M, Rosenberg SA.
42. McArthur GAC, Chapman PB, Robert C, et al. 47. Hatzivassiliou G, Song K, Yen I, et al. RAF High-dose recombinant interleukin-2 therapy in
Safety and efficacy of vemurafenib in inhibitors prime wild-type RAF to activate the patients with metastatic melanoma: long-term
BRAF(V600E) and BRAF(V600K) MAPK pathway and enhance growth. Nature. 2010; survival update. Cancer J Sci Am. 2000;6(suppl 1):
mutation-positive melanoma (BRIM-3): extended 464(7287):431-435. S11-S14.
follow-up of a phase 3, randomised, open-label 48. Long GV, Stroyakovskiy D, Gogas H, et al. 53. Agarwala SS. Current systemic therapy for
study. Lancet Oncol. 2014;15(3):323-332. Dabrafenib and trametinib versus dabrafenib and metastatic melanoma. Expert Rev Anticancer Ther.
43. Robert C, Dummer R, Gutzmer R, et al. placebo for Val600 BRAF-mutant melanoma: 2009;9(5):587-595.
Selumetinib plus dacarbazine versus placebo plus a multicentre, double-blind, phase 3 randomised 54. Middleton MR, Grob JJ, Aaronson N, et al.
dacarbazine as first-line treatment for controlled trial. Lancet. 2015;386(9992):444-451. Randomized phase III study of temozolomide
BRAF-mutant metastatic melanoma: a phase 2 49. Long GV, Menzies AM, Nagrial AM, et al. versus dacarbazine in the treatment of patients
double-blind randomised study. Lancet Oncol. 2013; Prognostic and clinicopathologic associations of with advanced metastatic malignant melanoma.
14(8):733-740. oncogenic BRAF in metastatic melanoma. J Clin [Erratum appears in J Clin Oncol 2000
44. Robert C, Long GV, Brady B, et al. Nivolumab in Oncol. 2011;29(10):1239-1246. Jun;18(11):2351]. J Clin Oncol. 2000;18(1):158-166.
previously untreated melanoma without BRAF 50. von Moos R, Seifert B, Simcock M, et al. 55. National Cancer Institute. Dabrafenib and
mutation. N Engl J Med. 2015;372(4):320-330. First-line temozolomide combined with Trametinib Followed by Ipilimumab and Nivolumab
45. Robert C, Schachter J, Long GV, et al; bevacizumab in metastatic melanoma: or Ipilimumab and Nivolumab Followed by
KEYNOTE-006 investigators. Pembrolizumab vs a multicentre phase II trial (SAKK 50/07). Ann Oncol. Dabrafenib and Trametinib in Treating Patients With
Ipilimumab in Advanced Melanoma. N Engl J Med. 2012;23(2):531-536. Stage III-IV BRAFV600 Melanoma. NLM Identifier:
2015;372(26):2521-2532. 51. Bhatia P, Friedlander P, Zakaria EA, Kandil E. NCT02224781. https://clinicaltrials.gov/ct2/show
46. Maio M, Grob JJ, Aamdal S, et al. Five-year Impact of BRAF mutation status in the prognosis of /NCT02224781 Accessed September 21, 2016.
survival rates for treatment-naive patients with
E8 JAMA Oncology Published online October 27, 2016 (Reprinted) jamaoncology.com
Copyright 2016 American Medical Association. All rights reserved.
Downloaded From: http://oncology.jamanetwork.com/ by a University of Tennessee - Knoxville User on 10/28/2016
You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2004 - Quality of Life in Romania I MargineanDocument206 pages2004 - Quality of Life in Romania I Margineandale_titiNo ratings yet
- Journal of Environmental Management: Ajay Singh TDocument7 pagesJournal of Environmental Management: Ajay Singh TNestor Garay CahuanaNo ratings yet
- Tugas Topic 4 Devi PermatasariDocument8 pagesTugas Topic 4 Devi PermatasariMartinaNo ratings yet
- Scan&SolveDocument24 pagesScan&SolveAtul ChauhanNo ratings yet
- Advanced Automatic ControlDocument26 pagesAdvanced Automatic Controlabdullah 3mar abou reashaNo ratings yet
- Daily Lesson Log 4Document5 pagesDaily Lesson Log 4Diane Marr Nicolas Dencio100% (2)
- ASI Hammer Injection Block ManualDocument16 pagesASI Hammer Injection Block ManualGerardo Manuel FloresNo ratings yet
- B11 - Overload Relays (Ref) ENDocument20 pagesB11 - Overload Relays (Ref) ENAhmed AbazaNo ratings yet
- Final Tana Beles - pdf2222Document72 pagesFinal Tana Beles - pdf2222Tiruneh Yeneneh100% (1)
- Ultrasonic Inspection of Welds in Tubes & Pipes: Educational NoteDocument13 pagesUltrasonic Inspection of Welds in Tubes & Pipes: Educational NoteleonciomavarezNo ratings yet
- Formula SheetDocument16 pagesFormula SheetgwerNo ratings yet
- Winter Solstice, CGW 2011Document38 pagesWinter Solstice, CGW 2011Lady HekateShadowMoonfire0% (1)
- Hira - For Shot Blasting & Upto 2nd Coat of PaintingDocument15 pagesHira - For Shot Blasting & Upto 2nd Coat of PaintingDhaneswar SwainNo ratings yet
- CTL Project Developer Perspective Coal - To - Liquids CoalitionDocument27 pagesCTL Project Developer Perspective Coal - To - Liquids Coalitiondwivediashish2No ratings yet
- Jcpenney Roto Tiller Front in e ManualDocument34 pagesJcpenney Roto Tiller Front in e Manualcb4pdfs100% (2)
- SuctioningDocument58 pagesSuctioningAyusa PradhanNo ratings yet
- Dave Graham Literature CatalogDocument640 pagesDave Graham Literature CatalogPierce PetersonNo ratings yet
- Kingspan 30 GSNDocument1 pageKingspan 30 GSNNoella AguiarNo ratings yet
- Strength of Materials: 2. Assume Missing Data, If Any, SuitablyDocument2 pagesStrength of Materials: 2. Assume Missing Data, If Any, SuitablynvnrevNo ratings yet
- The Poet of NatureDocument31 pagesThe Poet of NaturejulyNo ratings yet
- Introduction To Food Analysis2020Document2 pagesIntroduction To Food Analysis2020Ĝĭdęŷ KîřöşNo ratings yet
- Roland RS-5 Manual Del UsuarioDocument180 pagesRoland RS-5 Manual Del Usuariodavevad12345No ratings yet
- Economics 526 - Mathematics For Economists: Day(s) Time LocationDocument5 pagesEconomics 526 - Mathematics For Economists: Day(s) Time LocationGaurav JakhuNo ratings yet
- Mechanical Reasoning - Test 2: 40 QuestionsDocument14 pagesMechanical Reasoning - Test 2: 40 Questionskyloz60% (5)
- Easy Guide For Fujitsu T901 LaptopDocument141 pagesEasy Guide For Fujitsu T901 LaptopElaineNo ratings yet
- Nasua NasuaDocument9 pagesNasua NasuaJetsabellGutiérrezNo ratings yet
- Dynamic Test Report of DECR-S Excitation Devices: ExperimenterDocument14 pagesDynamic Test Report of DECR-S Excitation Devices: ExperimenterSalmanEjazNo ratings yet
- ASD Fan CalculatorsDocument14 pagesASD Fan CalculatorslubricacionNo ratings yet
- Building SOR 01.12.2020 Volume 1Document437 pagesBuilding SOR 01.12.2020 Volume 1Shiv Shankar Shukla82% (11)
- 10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtDocument145 pages10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtVuong DiepNo ratings yet