You might also like
- Children's Contact With The Outdoors and Nature: A Focus On Educators and Educational SettingsDocument54 pagesChildren's Contact With The Outdoors and Nature: A Focus On Educators and Educational SettingsChildren & Nature Network Resource LibraryNo ratings yet
- The Cult and Science of Public Health: A Sociological InvestigationFrom EverandThe Cult and Science of Public Health: A Sociological InvestigationNo ratings yet
- Influence of An Outdoor Garden On Mood and Stress in Older AdultsDocument13 pagesInfluence of An Outdoor Garden On Mood and Stress in Older Adultsmiščafl (Miro)No ratings yet
- Mental Health and Green SpaceDocument20 pagesMental Health and Green SpaceQasim ChacharNo ratings yet
- Norwood 220256Document34 pagesNorwood 220256Emad ElmaghrabyNo ratings yet
- Community and Environmental Benefits of Parks and RecreationDocument26 pagesCommunity and Environmental Benefits of Parks and RecreationltreyzonNo ratings yet
- Pag 31 3 249 PDFDocument6 pagesPag 31 3 249 PDFbobNo ratings yet
- Muñoz - Children in The OutdoorsDocument40 pagesMuñoz - Children in The Outdoorssmara_dgNo ratings yet
- Aging and The Environment: A Research Framework: Environmental Health Perspectives October 2005Document7 pagesAging and The Environment: A Research Framework: Environmental Health Perspectives October 2005Miguel Angel Telles TorresNo ratings yet
- Childhood Overweight and The Built Environment Making Technology Part of The SolutionRather Than Part of The Problem Author(s) Amy HillierDocument28 pagesChildhood Overweight and The Built Environment Making Technology Part of The SolutionRather Than Part of The Problem Author(s) Amy HillierEDWARD BOTNo ratings yet
- Understanding Urban Green SpaceDocument26 pagesUnderstanding Urban Green SpaceshereenNo ratings yet
- Outdoor Recreation For Every Body An Examination of Constraints ToDocument6 pagesOutdoor Recreation For Every Body An Examination of Constraints Toperakang00No ratings yet
- How Does The Environment Affect One's Health Both Physically and Mentaly?Document9 pagesHow Does The Environment Affect One's Health Both Physically and Mentaly?api-551760684No ratings yet
- DustinDocument12 pagesDustina1743019029No ratings yet
- Ijerph 18 02563 v3Document27 pagesIjerph 18 02563 v3Hoàng DiệpNo ratings yet
- Behavior Analysis in Public Health Fact Sheet - 220901Document1 pageBehavior Analysis in Public Health Fact Sheet - 220901javier plazaNo ratings yet
- People Value Green Surrounding As Important Part of Their Well BeingDocument4 pagesPeople Value Green Surrounding As Important Part of Their Well BeingRashid57% (58)
- Environmental Influences On Children'S Physical Activity and Diets in Rural Oregon: Results of A Youth Photovoice ProjectDocument10 pagesEnvironmental Influences On Children'S Physical Activity and Diets in Rural Oregon: Results of A Youth Photovoice Project7601235No ratings yet
- Final Draft W PaperDocument27 pagesFinal Draft W Paperapi-391688113No ratings yet
- Contribution of LeisureDocument13 pagesContribution of LeisureTaavonNo ratings yet
- Important Park Features For Encouraging Park VisitationDocument13 pagesImportant Park Features For Encouraging Park VisitationArturo Eduardo Villalpando FloresNo ratings yet
- Childrens Time OutdoorDocument20 pagesChildrens Time OutdoorIrisha AnandNo ratings yet
- BMC Public HealthDocument13 pagesBMC Public HealthBrittney Verine Dyhan HandoyoNo ratings yet
- Walk in The Park Final IWADocument10 pagesWalk in The Park Final IWAgamer juiceNo ratings yet
- Clare Cooper Marcus WCDH2000Document11 pagesClare Cooper Marcus WCDH2000JardimDeCalateiaNo ratings yet
- Environmental Identity, Well-Being, and MeaningDocument6 pagesEnvironmental Identity, Well-Being, and MeaningcristamborNo ratings yet
- Consumption of Nutritional Supplements Among Adolescents: Usage and Perceived BenefitsDocument10 pagesConsumption of Nutritional Supplements Among Adolescents: Usage and Perceived BenefitsKatyushaIvanovaNo ratings yet
- Proenvironmental Behaviour in Environmental Education ProgrammesDocument11 pagesProenvironmental Behaviour in Environmental Education ProgrammesBismah TayyabNo ratings yet
- The Relationship Between Built Environments and Physical Activity: A Systematic ReviewDocument7 pagesThe Relationship Between Built Environments and Physical Activity: A Systematic Reviewsole nav navNo ratings yet
- AVDs Complejas TestDocument17 pagesAVDs Complejas TestninafranNo ratings yet
- Environmental AwarenessDocument34 pagesEnvironmental Awarenesslourene100% (1)
- The Mental and Physical Health Outcomes of Green Exercise: Jules Pretty, Jo Peacock, Martin Sellens, & Murray GriffinDocument20 pagesThe Mental and Physical Health Outcomes of Green Exercise: Jules Pretty, Jo Peacock, Martin Sellens, & Murray GriffinAnonymous b2k9ABe7eNo ratings yet
- International Journal of Behavioral Nutrition and Physical ActivityDocument10 pagesInternational Journal of Behavioral Nutrition and Physical Activityriri sariNo ratings yet
- Got The Blues, Then Find Some Greenspace: The Mental Health Benefits of Green Exercise Activities and Green CareDocument49 pagesGot The Blues, Then Find Some Greenspace: The Mental Health Benefits of Green Exercise Activities and Green Carecalderdavid35No ratings yet
- Ijbt 1 - 3 - 3 - 423-433Document11 pagesIjbt 1 - 3 - 3 - 423-433Shamerra SabtuNo ratings yet
- Urban Biodiversity and Adolescent Mental Health and Well-BeingDocument9 pagesUrban Biodiversity and Adolescent Mental Health and Well-BeingAndrés SmithNo ratings yet
- Gerontology Individual Assignment 1Document14 pagesGerontology Individual Assignment 1Innocent T SumburetaNo ratings yet
- Environmental Factors Associated With Physical Activity in Childcare CentersDocument9 pagesEnvironmental Factors Associated With Physical Activity in Childcare Centersriri sariNo ratings yet
- The Effect of Physical Activity and Diet in Primary School ChildrenDocument7 pagesThe Effect of Physical Activity and Diet in Primary School ChildrenMuhammad Faraz HasanNo ratings yet
- Zhang Et Al 2017Document15 pagesZhang Et Al 2017Mahmoud Abdelfatah MahgoubNo ratings yet
- Descriptive and Injunctive NormsDocument13 pagesDescriptive and Injunctive NormskyzzzNo ratings yet
- Review 2008 enDocument6 pagesReview 2008 envimlenNo ratings yet
- The Health Benefits of Parks by Erica GiesDocument26 pagesThe Health Benefits of Parks by Erica GiesJohnz2No ratings yet
- Understanding Barriers and Facilitators of Fruit and Vegetable Consumption Among A Diverse Multi-Ethnic Population in The USADocument11 pagesUnderstanding Barriers and Facilitators of Fruit and Vegetable Consumption Among A Diverse Multi-Ethnic Population in The USAicanupinNo ratings yet
- 2003 - Gillian King - AConceptualModeloftheFactorsAffectingtheRecreationretrieved-2014!02!15Document28 pages2003 - Gillian King - AConceptualModeloftheFactorsAffectingtheRecreationretrieved-2014!02!15Gurbaani MaahiNo ratings yet
- FDQ 068Document11 pagesFDQ 068Jaspreet KaurNo ratings yet
- Has El Wand Terja Gin Gpa 2015Document9 pagesHas El Wand Terja Gin Gpa 2015PHOEBE BACUNLAYNo ratings yet
- How Natural and Built Environments Impact Human Health: Dr. Nancy WellsDocument4 pagesHow Natural and Built Environments Impact Human Health: Dr. Nancy WellsBettina TiongcoNo ratings yet
- City Trees, Nature and Physical Activity: Keeping People Fit and HealthyDocument4 pagesCity Trees, Nature and Physical Activity: Keeping People Fit and HealthyNeroulidi854No ratings yet
- Factors Related To Physically Active Leisure Among College StudentsDocument18 pagesFactors Related To Physically Active Leisure Among College StudentsYong YangNo ratings yet
- What Is The Best Dose of Nature and Green Exercise For Improving Mental Health? A Multi-Study AnalysisDocument9 pagesWhat Is The Best Dose of Nature and Green Exercise For Improving Mental Health? A Multi-Study Analysisapi-285793142No ratings yet
- April Researchfile enDocument2 pagesApril Researchfile ensummer123No ratings yet
- STA 13 (hw1)Document10 pagesSTA 13 (hw1)Jelly Jelly JamjamNo ratings yet
- An Introduction To Global Health EthicsDocument228 pagesAn Introduction To Global Health EthicsRiyadh ArtworkNo ratings yet
- Driving: A Road To Unhealthy Lifestyles and Poor Health OutcomesDocument5 pagesDriving: A Road To Unhealthy Lifestyles and Poor Health OutcomesLuis Ángel RuizNo ratings yet
- NIH Public AccessDocument27 pagesNIH Public AccessAlinaNo ratings yet
- The Healing Power of Nature: The Need For Nature For Human Health, Development, and WellbeingDocument55 pagesThe Healing Power of Nature: The Need For Nature For Human Health, Development, and WellbeingKlausEllegaard11100% (2)
- ArticleDocument19 pagesArticleKITTIVONGSAK VONGSUTHEP KEITHNo ratings yet
- Promoting Physical Activity in Preschoolers To Prevent Obesity: A Review of The LiteratureDocument17 pagesPromoting Physical Activity in Preschoolers To Prevent Obesity: A Review of The LiteratureSufi IndrainiNo ratings yet
- Plants An International Scientific Open Access Jou PDFDocument6 pagesPlants An International Scientific Open Access Jou PDFSaahndong RansomNo ratings yet
- The Morphology of PlantsDocument2 pagesThe Morphology of PlantsMuhammad Jamshaid RasheedNo ratings yet
- Tasks For Online Lab 3Document3 pagesTasks For Online Lab 3Muhammad Jamshaid RasheedNo ratings yet
- Lab 1Document3 pagesLab 1Muhammad Jamshaid RasheedNo ratings yet
- SE Assignment 01Document4 pagesSE Assignment 01Muhammad Jamshaid RasheedNo ratings yet
- Channel EncodingDocument1 pageChannel EncodingMuhammad Jamshaid RasheedNo ratings yet
- Trewavas 2003 1Document20 pagesTrewavas 2003 1Wendell SoaresNo ratings yet
- DB-Lab No 2Document8 pagesDB-Lab No 2Muhammad Jamshaid RasheedNo ratings yet
- DB-Lab No 1Document15 pagesDB-Lab No 1Muhammad Jamshaid RasheedNo ratings yet
- Local Park Use and Personal Health Among Older Adults: An Exploratory StudyDocument20 pagesLocal Park Use and Personal Health Among Older Adults: An Exploratory StudyMuhammad Jamshaid RasheedNo ratings yet
- Bibliometric AnalysisDocument6 pagesBibliometric AnalysisMuhammad Jamshaid RasheedNo ratings yet
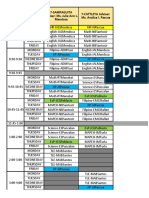
- JHS Class Program S.Y. 2021 2022 SchoolDocument26 pagesJHS Class Program S.Y. 2021 2022 SchooljunapoblacioNo ratings yet
- Tinetti Assessment BalanceDocument3 pagesTinetti Assessment BalanceAlexandra DeacNo ratings yet
- 8607 Field Notes-2Document39 pages8607 Field Notes-2Wasim SajjadNo ratings yet
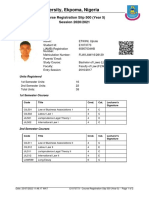
- Course Registration SlipDocument2 pagesCourse Registration SlipEmmanuel EmilolarNo ratings yet
- CB Recruitment Promotion Policy 2020 12 6 2020Document34 pagesCB Recruitment Promotion Policy 2020 12 6 2020Wasii KhanNo ratings yet
- Lipmans Thinking in Education PDFDocument7 pagesLipmans Thinking in Education PDFLaura Nicoleta BorhanNo ratings yet
- Part 1 - Nsdga Faculty Orientation - School Profile & FacilitiesDocument35 pagesPart 1 - Nsdga Faculty Orientation - School Profile & FacilitiesPaul Gian UrrutiaNo ratings yet
- Btech CGPA Calculation BookDocument5 pagesBtech CGPA Calculation BookvijayaNo ratings yet
- PLC StrategiesDocument3 pagesPLC StrategiesGan Zi XiNo ratings yet
- BMMS5103 Full Version Study Guide PDFDocument211 pagesBMMS5103 Full Version Study Guide PDFWill NguyenNo ratings yet
- Virginia Tech April 16 - Handwritten Notes (Part 3)Document300 pagesVirginia Tech April 16 - Handwritten Notes (Part 3)PrevailArchive100% (1)
- Npcil RecruitmentDocument2 pagesNpcil RecruitmentAnshul SharmaNo ratings yet
- Horsemanship Merit Badge WorksheetDocument5 pagesHorsemanship Merit Badge WorksheetsrcouncilNo ratings yet
- The Kano Model - A Review of Its Application in Marketing Research From 1984 To 2006Document10 pagesThe Kano Model - A Review of Its Application in Marketing Research From 1984 To 2006gschiroNo ratings yet
- Specialty Coffee Training PrinciplesDocument49 pagesSpecialty Coffee Training PrinciplesMinh Dai NguyenNo ratings yet
- Syllabus Advanced Dynamics 2018Document5 pagesSyllabus Advanced Dynamics 2018mikeNo ratings yet
- Chapter IvDocument10 pagesChapter IvJohn Mark Fernandez DanlagNo ratings yet
- NMMSDocument2 pagesNMMSAllenNo ratings yet
- Alternative Breaks Grant Proposal Executive SummaryDocument7 pagesAlternative Breaks Grant Proposal Executive SummaryMarina KarasikNo ratings yet
- Assignment ProbabilityDocument6 pagesAssignment ProbabilityVarun LalwaniNo ratings yet
- EceDocument67 pagesEceaditya_pundirNo ratings yet
- 807 Unit 3 Weebly ScheduleDocument6 pages807 Unit 3 Weebly Scheduleapi-330272570No ratings yet
- Dost Form No 2Document6 pagesDost Form No 2Lester OnianaNo ratings yet
- General PsychologyDocument22 pagesGeneral PsychologyZeph DugangNo ratings yet
- The NDA and The IMA...Document18 pagesThe NDA and The IMA...Frederick NoronhaNo ratings yet
- TRANSLATIONassessment CONFERENCEDocument21 pagesTRANSLATIONassessment CONFERENCEgrifonkaNo ratings yet
- ANSCOMBE On Brute Facts PDFDocument5 pagesANSCOMBE On Brute Facts PDFadikarmikaNo ratings yet
- General Knowledge Test Information GuideDocument42 pagesGeneral Knowledge Test Information Guideapi-321973122No ratings yet
- Moral and Legal Issues in EducationDocument9 pagesMoral and Legal Issues in EducationallannaryanadasNo ratings yet
- Drawing, Estimation & Construction (CE-209)Document8 pagesDrawing, Estimation & Construction (CE-209)haseebahmadNo ratings yet