You might also like
- Cranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Document262 pagesCranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Alvaro RivCalle87% (15)
- Wilson - Cranial NervesDocument243 pagesWilson - Cranial NervesBiblioteca CSNT100% (13)
- Bickerstaff Neurological ExaminationDocument386 pagesBickerstaff Neurological ExaminationSwarnadeep Mani100% (5)
- Bell's Palsy - Treatment GuidelinesDocument4 pagesBell's Palsy - Treatment GuidelinessevattapillaiNo ratings yet
- 1 - Orientation, History Taking and ExaminationDocument96 pages1 - Orientation, History Taking and ExaminationHari ShresthaNo ratings yet
- MCQs NeuroDocument2 pagesMCQs NeuroBagadi Suneel100% (2)
- Critical Care in NeurologyDocument65 pagesCritical Care in NeurologydrbhawnavermaNo ratings yet
- Speech Characteristics of Different Types of Dysarthria: by Dr. Somesh Maheshwari, IndoreDocument21 pagesSpeech Characteristics of Different Types of Dysarthria: by Dr. Somesh Maheshwari, IndoreDr. Somesh MaheshwariNo ratings yet
- Exit Hesi Study GuideDocument67 pagesExit Hesi Study GuideMonel Benjamin100% (26)
- Cranial Nerve LabDocument3 pagesCranial Nerve LabSteve Sullivan100% (3)
- Tensile Testing Asm StandardDocument13 pagesTensile Testing Asm StandardNinad PawarNo ratings yet
- PEAC OphthalmologyDocument45 pagesPEAC OphthalmologySdNo ratings yet
- Visual Field Defect Case ReportDocument25 pagesVisual Field Defect Case Report033010969No ratings yet
- Bell's Palsy: Signs and SymptomsDocument9 pagesBell's Palsy: Signs and SymptomsMd.Sharifuzzaman FarabiNo ratings yet
- When, Why and Where in Oral and Maxillofacial SurgeryDocument346 pagesWhen, Why and Where in Oral and Maxillofacial Surgeryতৌহিদ তপু0% (1)
- Medical Surgical Nursing 64 PagsDocument64 pagesMedical Surgical Nursing 64 Pagstanya nNo ratings yet
- Facial Nerve Paralysis 2Document44 pagesFacial Nerve Paralysis 2Omowole GbengaNo ratings yet
- Facial ParalysisDocument59 pagesFacial ParalysisSUnil Kumar100% (1)
- Diagnosis Approach of Optic Neuritis 2155 9562 1000345Document13 pagesDiagnosis Approach of Optic Neuritis 2155 9562 1000345Juaan AvilaNo ratings yet
- Ei 2311 Biomedical Instrumentation 2 MarDocument41 pagesEi 2311 Biomedical Instrumentation 2 MarVel MuruganNo ratings yet
- Chapter 14 15 16 PDFDocument158 pagesChapter 14 15 16 PDFmp1757No ratings yet
- Smile Restoration After Facial PalsyDocument6 pagesSmile Restoration After Facial PalsyJimmie CooperNo ratings yet
- Ophthalmology Case Write UpDocument15 pagesOphthalmology Case Write UpSalsabila Al-Basheer100% (4)
- Soal Pretes Calon PPDS Ilmu Bedah SarafDocument6 pagesSoal Pretes Calon PPDS Ilmu Bedah SarafdewiNo ratings yet
- Neurology of Swallowing and DysphagiaDocument24 pagesNeurology of Swallowing and DysphagiaMaríaFernandaCampanoGacitúaNo ratings yet
- A Systemic Approach To Facial Nerve ParalysisDocument11 pagesA Systemic Approach To Facial Nerve Paralysissudheer joelNo ratings yet
- Practice EssentialsDocument10 pagesPractice EssentialsAnonymous gMLTpER9IUNo ratings yet
- Jurnal Saraf 5Document5 pagesJurnal Saraf 5Suci MayveraNo ratings yet
- Brainstem and Cranial Nerves: Diplopia, Abducens Nerve, Bell's PalsyDocument55 pagesBrainstem and Cranial Nerves: Diplopia, Abducens Nerve, Bell's PalsynilaahanifahNo ratings yet
- PrintDocument32 pagesPrintnewtonNo ratings yet
- Facial Nerve PalsyDocument3 pagesFacial Nerve PalsySusan BensonNo ratings yet
- 1 s2.0 S2090074015000833 MainDocument3 pages1 s2.0 S2090074015000833 MainMuhammad Fuad MahfudNo ratings yet
- Bell's PalsyDocument37 pagesBell's PalsyobligatraftelNo ratings yet
- Central Serous Chorioretinopathy Induced by Work StressDocument16 pagesCentral Serous Chorioretinopathy Induced by Work StressVincent RoorohNo ratings yet
- Bilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanDocument3 pagesBilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanmimicamasoNo ratings yet
- Bilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case ReportDocument3 pagesBilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case Reportokto namikaNo ratings yet
- A Review of Neuro-Ophthalmologic EmergenciesDocument5 pagesA Review of Neuro-Ophthalmologic EmergenciesZakiyul FuadNo ratings yet
- Aetiologies and Pathophysiological Basis of Monocular Visual AuraDocument6 pagesAetiologies and Pathophysiological Basis of Monocular Visual AuraIJAR JOURNALNo ratings yet
- Multiple Sclerosis With Ophthalmologic Onset - Case ReportDocument5 pagesMultiple Sclerosis With Ophthalmologic Onset - Case ReportVannyNo ratings yet
- Neuro-Ophthalmology at The Bedside A Clinical GuidDocument13 pagesNeuro-Ophthalmology at The Bedside A Clinical GuidHasan Masud RahmanNo ratings yet
- Bells PalsyDocument32 pagesBells PalsymallikmcNo ratings yet
- J Survophthal 2019 06 001Document25 pagesJ Survophthal 2019 06 001Serque777No ratings yet
- Bell Palsy: Clinical Examination and Management: ReviewDocument8 pagesBell Palsy: Clinical Examination and Management: ReviewCitraNo ratings yet
- Referat Diplopia (Neuro)Document23 pagesReferat Diplopia (Neuro)Nadira DanataNo ratings yet
- What Is Facial PalsyDocument9 pagesWhat Is Facial Palsymayonour22No ratings yet
- Neuro-Ophthalmology: Simon J HickmanDocument10 pagesNeuro-Ophthalmology: Simon J Hickmanhalvi89No ratings yet
- Test Bank For Advanced Practice Nursing in The Care of Older Adults 2nd by Kennedy Malone DownloadDocument10 pagesTest Bank For Advanced Practice Nursing in The Care of Older Adults 2nd by Kennedy Malone Downloadericgoodmanfaszgwponk100% (30)
- Bell's Palsy or Idiopathic Facial ParalysisDocument6 pagesBell's Palsy or Idiopathic Facial ParalysisFarheen FatimaNo ratings yet
- Laporan Kasus NeurooftalmologiDocument12 pagesLaporan Kasus NeurooftalmologiPradistya Syifa YudiasariNo ratings yet
- Facial Paralysis Reconstruction in Children and Adolescents With Central Nervous System TumorsDocument12 pagesFacial Paralysis Reconstruction in Children and Adolescents With Central Nervous System TumorsCarlos Ageno AlemánNo ratings yet
- Facial PalsyDocument37 pagesFacial PalsyamshaydeeNo ratings yet
- A Rare Cause of Hearing Loss: Susac SyndromeDocument3 pagesA Rare Cause of Hearing Loss: Susac SyndromeBeny Pratama SidabutarNo ratings yet
- Migraña RetinianaDocument4 pagesMigraña RetinianaJZHZL QNo ratings yet
- Conditions With Unilateral Presentation A Diagnostic ChallengeDocument7 pagesConditions With Unilateral Presentation A Diagnostic ChallengeEditor IJTSRDNo ratings yet
- Visual Findings As Primary Manifestations in Patients With Intracranial TumorsDocument4 pagesVisual Findings As Primary Manifestations in Patients With Intracranial TumorsScoalaAuto AutoSorNo ratings yet
- 138975-Article Text-370968-1-10-20160708Document5 pages138975-Article Text-370968-1-10-20160708john smithNo ratings yet
- Traumatic Optic NeuropathyDocument32 pagesTraumatic Optic NeuropathyGeraldi Ayub Fujiwan TombeNo ratings yet
- Migrena OftalmicaDocument8 pagesMigrena OftalmicaIulia MoldovanNo ratings yet
- Guidelines For The Initial Management of Acute Facial PalsyDocument14 pagesGuidelines For The Initial Management of Acute Facial Palsy郭品榆No ratings yet
- Abstract 5Document7 pagesAbstract 5rluiknagwa lingNo ratings yet
- Work Stress Induced CSCDocument15 pagesWork Stress Induced CSCVincent Rooroh0% (1)
- MuscleDocument7 pagesMuscleasenamNo ratings yet
- Disorders of Optic Nerve and Visual Pathways: Ipek MidiDocument24 pagesDisorders of Optic Nerve and Visual Pathways: Ipek MidiEcaterina ChiriacNo ratings yet
- Wang.2008.Central Serous ChorioretinopathyDocument20 pagesWang.2008.Central Serous ChorioretinopathyRohit GuptaNo ratings yet
- Herpes Zoster Lyme Disease Syphilis Epstein-Barr Viral Infection Cytomegalovirus HIV Mycoplasma Diabetes Mellitus HypertensionDocument14 pagesHerpes Zoster Lyme Disease Syphilis Epstein-Barr Viral Infection Cytomegalovirus HIV Mycoplasma Diabetes Mellitus HypertensionShasha ShakinahNo ratings yet
- Orbital Apex Syndrome With Encephalitis A Rare and Serious Complication of Herpes Zoster Opthalmicus - Ludwig Melino Tjokrovonco 2Document12 pagesOrbital Apex Syndrome With Encephalitis A Rare and Serious Complication of Herpes Zoster Opthalmicus - Ludwig Melino Tjokrovonco 2Handi KrisnaniNo ratings yet
- Journal Article 17 263 PDFDocument5 pagesJournal Article 17 263 PDFwolfang2001No ratings yet
- E RefdDocument13 pagesE RefdGabriella TjondroNo ratings yet
- Traumatic Optic NeuropathyDocument2 pagesTraumatic Optic NeuropathyIJAR JOURNALNo ratings yet
- Bells PalsyDocument6 pagesBells PalsyElisabeth TikalakaNo ratings yet
- Orbital/Periorbital Plexiform Neuro Fibromas in Children With Neuro Fibromatosis Type 1 Multidisciplinary Recommendations For CareDocument10 pagesOrbital/Periorbital Plexiform Neuro Fibromas in Children With Neuro Fibromatosis Type 1 Multidisciplinary Recommendations For CareYesicaNo ratings yet
- Neuro OphthalmologyDocument2 pagesNeuro OphthalmologyJovan Z. PopovićNo ratings yet
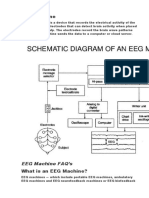
- EEG MachineDocument3 pagesEEG MachineOlea ScorpanNo ratings yet
- Activitatea Electrodermala in Stres. DR - CorneliuMoldovanDocument16 pagesActivitatea Electrodermala in Stres. DR - CorneliuMoldovanMariaNo ratings yet
- Electrical Modalities Basic Principles of Electricity - : ObjectivesDocument19 pagesElectrical Modalities Basic Principles of Electricity - : ObjectivesOlea ScorpanNo ratings yet
- DegradationDocument2 pagesDegradationOlea ScorpanNo ratings yet
- Electrical Modalities Basic Principles of Electricity - : ObjectivesDocument19 pagesElectrical Modalities Basic Principles of Electricity - : ObjectivesOlea ScorpanNo ratings yet
- Suture MaterialDocument76 pagesSuture MaterialOlea ScorpanNo ratings yet
- Biomedical Instrumentation NotesDocument13 pagesBiomedical Instrumentation NotesashvathNo ratings yet
- Working Principle of Biosensors: Respiratory System Renal SystemDocument2 pagesWorking Principle of Biosensors: Respiratory System Renal SystemOlea ScorpanNo ratings yet
- Neuropatia SciaticaDocument2 pagesNeuropatia SciaticaOlea ScorpanNo ratings yet
- Biomedical Instrumentation NotesDocument13 pagesBiomedical Instrumentation NotesashvathNo ratings yet
- Bio InstrumentationDocument15 pagesBio InstrumentationOlea ScorpanNo ratings yet
- Facial Nerve Palsy: Original Article Contributed byDocument8 pagesFacial Nerve Palsy: Original Article Contributed byOlea ScorpanNo ratings yet
- Intraperitoneal Injection IP Intravenous InjectionDocument13 pagesIntraperitoneal Injection IP Intravenous InjectionOlea ScorpanNo ratings yet
- Clasificarea CelulelorDocument60 pagesClasificarea CelulelorOlea ScorpanNo ratings yet
- The Portal Vein, The Main Blood Supply To The Liver. Clear Evidence That Cells Delivered Via TheDocument4 pagesThe Portal Vein, The Main Blood Supply To The Liver. Clear Evidence That Cells Delivered Via TheOlea ScorpanNo ratings yet
- Aspectul Terapeutic Al NeiromidineiDocument3 pagesAspectul Terapeutic Al NeiromidineiOlea ScorpanNo ratings yet
- Zhongguo Zhen JiuDocument2 pagesZhongguo Zhen JiuOlea ScorpanNo ratings yet
- Freezing !!! PDFDocument9 pagesFreezing !!! PDFOlea ScorpanNo ratings yet
- !!!randomized Controlled Comparative Study On e Ect of Training To Improve Lower Limb Motor Paralysis in Convalescent Patients With Post-Stroke HemiplegiaDocument4 pages!!!randomized Controlled Comparative Study On e Ect of Training To Improve Lower Limb Motor Paralysis in Convalescent Patients With Post-Stroke HemiplegiaOlea ScorpanNo ratings yet
- Comorbidity IndexDocument145 pagesComorbidity IndexOlea ScorpanNo ratings yet
- Comorbidity IndexDocument145 pagesComorbidity IndexOlea ScorpanNo ratings yet
- Acupunture For Premenstrual SindromeDocument17 pagesAcupunture For Premenstrual SindromeOlea ScorpanNo ratings yet
- 1472 6963 10 213 2Document10 pages1472 6963 10 213 2Olea ScorpanNo ratings yet
- Classi Cation of Subtypes of Ischemic Stroke History of The Trial of Org 10172 in Acute Stroke Treatment Classi CationDocument9 pagesClassi Cation of Subtypes of Ischemic Stroke History of The Trial of Org 10172 in Acute Stroke Treatment Classi CationOlea ScorpanNo ratings yet
- Brain & Behavior Lecture NotesDocument2 pagesBrain & Behavior Lecture NotesmcginnisstudioNo ratings yet
- Cranial NeuralgiasDocument14 pagesCranial NeuralgiasHabib G. Moutran BarrosoNo ratings yet
- 10 The Nervous System 2Document6 pages10 The Nervous System 2Cristina AdolfoNo ratings yet
- Multiple Cranial NeuropathyDocument13 pagesMultiple Cranial NeuropathyChaerani SalamNo ratings yet
- Internal Medicine (I) Log Book Black Color TypingDocument48 pagesInternal Medicine (I) Log Book Black Color TypingQasim HaleimiNo ratings yet
- Therefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishDocument66 pagesTherefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishBaishakhi ChakrabortyNo ratings yet
- Nervous System Anatomy and FunctionsDocument26 pagesNervous System Anatomy and FunctionsSyifa KaniaNo ratings yet
- Acoustic Reflex Threshold (ART) Patterns: An Interpretation Guide For Students and Supervisors: Course Material and Exam Questions Course MaterialDocument17 pagesAcoustic Reflex Threshold (ART) Patterns: An Interpretation Guide For Students and Supervisors: Course Material and Exam Questions Course Materialn_almagroNo ratings yet
- NUR260 Exam 3 Study Guide FA20 TTNDocument4 pagesNUR260 Exam 3 Study Guide FA20 TTNclarimerNo ratings yet
- ACTIVITY On Neuro AssessmentDocument25 pagesACTIVITY On Neuro AssessmentGuillana Mae CastellonNo ratings yet
- Brain CancerDocument74 pagesBrain CancerDan EvanzNo ratings yet
- Icd 9 CM (Tabulasi) 2012Document263 pagesIcd 9 CM (Tabulasi) 2012M Taufik Harahap100% (1)
- LinksDocument24 pagesLinksTrisNo ratings yet
- Aiims Anatomy NotesDocument46 pagesAiims Anatomy Notesshalialoo22No ratings yet
- Test QuestionsDocument28 pagesTest QuestionsJerson CastroNo ratings yet
- Exam MCQ Clinanatomy 2022-23Document21 pagesExam MCQ Clinanatomy 2022-23CHoudhary Hassan WarraichNo ratings yet
- There Are 12 Pairs of Cranial NervesDocument6 pagesThere Are 12 Pairs of Cranial NervesJessica RebbenNo ratings yet