You might also like
- 10 1097mao 0000000000000390Document4 pages10 1097mao 0000000000000390Meva'a RogerNo ratings yet
- Borgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloDocument13 pagesBorgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloJaime Angel Ortiz DiazNo ratings yet
- Cricchio 2009Document7 pagesCricchio 2009elver galargaNo ratings yet
- Low-Cost Sex Reassignment Synthetic ModelDocument2 pagesLow-Cost Sex Reassignment Synthetic ModelAlexandre SáNo ratings yet
- 86 Ijar-19401Document14 pages86 Ijar-19401Shinta rahma MansyurNo ratings yet
- Ajol File Journals - 520 - Articles - 245255 - Submission - Proof - 245255 6121 588598 1 10 20230406Document11 pagesAjol File Journals - 520 - Articles - 245255 - Submission - Proof - 245255 6121 588598 1 10 20230406John SmithNo ratings yet
- Artigo de Estereologia e CriostatoDocument13 pagesArtigo de Estereologia e CriostatoAndra SilvaNo ratings yet
- Cranioplasty Review of Materials and TechniquesDocument8 pagesCranioplasty Review of Materials and TechniquesCahyo Adi BaskoroNo ratings yet
- Medicina 59 00355Document12 pagesMedicina 59 00355Anuj BhardwajNo ratings yet
- Septoplasty Training During The COVID-19 Era: Development and Validation of A Novel Low-Cost Simulation ModelDocument8 pagesSeptoplasty Training During The COVID-19 Era: Development and Validation of A Novel Low-Cost Simulation ModelFelipe Anduquia GarayNo ratings yet
- Korn 2017Document14 pagesKorn 2017Aris SetyawanNo ratings yet
- 737 Ijar-23255Document7 pages737 Ijar-23255Louis HutahaeanNo ratings yet
- Artigo Ibju Micro Uro 2019-0092 PDFDocument7 pagesArtigo Ibju Micro Uro 2019-0092 PDFDr. Luis Otavio Pinto - Urologia ReconstrutoraNo ratings yet
- Split Technique 3Document13 pagesSplit Technique 3Alejandro RuizNo ratings yet
- Retention of Maxillofacial Prosthesis PDFDocument6 pagesRetention of Maxillofacial Prosthesis PDFBismita PradhanNo ratings yet
- Split Technique 1Document7 pagesSplit Technique 1Alejandro RuizNo ratings yet
- Application of Rapid Prototyping Technology in Maxillofacial ProstheticsDocument7 pagesApplication of Rapid Prototyping Technology in Maxillofacial Prostheticsharshita parasharNo ratings yet
- Thesis Copy 6 CorrectedDocument54 pagesThesis Copy 6 CorrectedanushiNo ratings yet
- Ceo0042 0665Document10 pagesCeo0042 0665walid abdallahNo ratings yet
- The Production of Anatomical Teaching Resources Using Three-Dimensional (3D) Printing TechnologyDocument9 pagesThe Production of Anatomical Teaching Resources Using Three-Dimensional (3D) Printing Technologyfrancisco javier santos ruedaNo ratings yet
- Stereolithography JCDocument14 pagesStereolithography JCpravallika ammuNo ratings yet
- Full Text Article Clinical Oral Invest May 2013Document84 pagesFull Text Article Clinical Oral Invest May 2013謎超人No ratings yet
- Periosteum-Derived Micro-Grafts For Tissue RegenerDocument6 pagesPeriosteum-Derived Micro-Grafts For Tissue RegenerAndrea AriasNo ratings yet
- Novellino 2013Document6 pagesNovellino 2013Glais FerrariNo ratings yet
- Good Maxillofacial ArticleDocument11 pagesGood Maxillofacial Articledrchabra dentalNo ratings yet
- Casas-Murillo2021 Article 3D-printedAnatomicalModelsOfThDocument8 pagesCasas-Murillo2021 Article 3D-printedAnatomicalModelsOfThVicente Bruno GuimaraesNo ratings yet
- 11.behavioral Study of Conchal Cartilage Autograft - An Animal Model ResearchDocument3 pages11.behavioral Study of Conchal Cartilage Autograft - An Animal Model ResearchDR K C MALLIKNo ratings yet
- The New "Cubism" Graft Technique in Tympanoplasty - A Randomized Controlled TrialDocument9 pagesThe New "Cubism" Graft Technique in Tympanoplasty - A Randomized Controlled Trialian danarkoNo ratings yet
- Endodontic ArmamentariumDocument29 pagesEndodontic ArmamentariumAbdulSamiNo ratings yet
- Zhou - Virtual Shape ModelDocument10 pagesZhou - Virtual Shape ModelRicardo GrilloNo ratings yet
- Study of Ear Biometrics Based Identification System Using Machine LearningDocument9 pagesStudy of Ear Biometrics Based Identification System Using Machine LearningIJRASETPublicationsNo ratings yet
- The Sheep As An Animal Model in Orthopaedic ResearchDocument4 pagesThe Sheep As An Animal Model in Orthopaedic ResearchAlina TeodorescuNo ratings yet
- Sutura X Art.Document11 pagesSutura X Art.jessica5rcNo ratings yet
- Abstract Clin Oral Invest Resumes ConsEuro 2013bDocument84 pagesAbstract Clin Oral Invest Resumes ConsEuro 2013bRoxana OneaNo ratings yet
- Jced 13 E935Document6 pagesJced 13 E935Marwa Wagih ElboraeyNo ratings yet
- Lymphatic DrainageDocument49 pagesLymphatic DrainageMehek BatraNo ratings yet
- Medical Education - Simulation and Virtual RealityDocument2 pagesMedical Education - Simulation and Virtual Realityapi-688059491No ratings yet
- Socket Shield Technique For Implant Placement To Stabilize The Facial Gingival and Osseous Architecture: A Systematic ReviewDocument13 pagesSocket Shield Technique For Implant Placement To Stabilize The Facial Gingival and Osseous Architecture: A Systematic ReviewАртур Медрано ДиасNo ratings yet
- Journal of The World Federation of Orthodontists: Original ResearchDocument7 pagesJournal of The World Federation of Orthodontists: Original ResearchAndrésAcostaNo ratings yet
- Reusing Dental Implants?: An Experimental Study For Detecting The Success Rates of Re-OsseointegrationDocument7 pagesReusing Dental Implants?: An Experimental Study For Detecting The Success Rates of Re-OsseointegrationSatya AsatyaNo ratings yet
- qi_Soldatos_37133Document18 pagesqi_Soldatos_37133Juliana Gomes BarretoNo ratings yet
- Guidance On Good Cell Culture PracticeDocument28 pagesGuidance On Good Cell Culture PracticeNyna KawlesNo ratings yet
- Implant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoDocument6 pagesImplant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoMelina Nataly Robles AcuñaNo ratings yet
- Chemvibes Chemvibes Chemvibes ChemvibesDocument32 pagesChemvibes Chemvibes Chemvibes ChemvibeschmcstudsNo ratings yet
- Immediate or Early Placement of Implants Following Tooth Extraction: Review of Biologic Basis, Clinical Procedures, and OutcomesDocument15 pagesImmediate or Early Placement of Implants Following Tooth Extraction: Review of Biologic Basis, Clinical Procedures, and OutcomesFelipe CastroNo ratings yet
- J Tissue Eng Regen Med - 2022 - Louvrier - Development of A Biomimetic Bioreactor For Regenerative Endodontics ResearchDocument10 pagesJ Tissue Eng Regen Med - 2022 - Louvrier - Development of A Biomimetic Bioreactor For Regenerative Endodontics ResearchPedro AfonsoNo ratings yet
- Philips Gyroscan T10-NT CT-MR Cochlea LengthDocument7 pagesPhilips Gyroscan T10-NT CT-MR Cochlea LengthSinisa HristovNo ratings yet
- Running Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Document16 pagesRunning Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Roja AllampallyNo ratings yet
- Esearch RticleDocument5 pagesEsearch RticleMin Htet KoNo ratings yet
- Journal of Oral Biology and Craniofacial ResearchDocument4 pagesJournal of Oral Biology and Craniofacial ResearchRafika OljNo ratings yet
- InstrumentationDocument12 pagesInstrumentationMaiush JbNo ratings yet
- Dental Occlusion Ties A Rapid Safe and Non-InvasivDocument6 pagesDental Occlusion Ties A Rapid Safe and Non-InvasivFernando CasanovaNo ratings yet
- Bajka Et Al-2004-Clinical AnatomyDocument10 pagesBajka Et Al-2004-Clinical Anatomywhiterose.storiesNo ratings yet
- Oral Tissue EngineeringDocument3 pagesOral Tissue EngineeringIJAR JOURNALNo ratings yet
- Digital Planning For Immediate Implants in Anterior EstheticDocument9 pagesDigital Planning For Immediate Implants in Anterior EstheticGustavo IsmaelNo ratings yet
- Development of A Mouse Model For Pulp-Dentin ComplDocument8 pagesDevelopment of A Mouse Model For Pulp-Dentin ComplLindaNo ratings yet
- Clin Oral Invest Btcp Type 1 Col ConesDocument10 pagesClin Oral Invest Btcp Type 1 Col ConesPathivada LumbiniNo ratings yet
- Buap PDFDocument7 pagesBuap PDFWawawaNo ratings yet
- Construction of An Implant-Retained Auricular Prosthesis With The Aid of Contemporary Digital Technologies: A Clinical ReportDocument5 pagesConstruction of An Implant-Retained Auricular Prosthesis With The Aid of Contemporary Digital Technologies: A Clinical ReportnoranNo ratings yet
- Chapter 2 Background To This ProposalDocument10 pagesChapter 2 Background To This ProposalMMatute FDNo ratings yet
- CAE-Services Llc Numerical Analysis of Supersonic Missile Flow with Transverse Jet InjectionDocument2 pagesCAE-Services Llc Numerical Analysis of Supersonic Missile Flow with Transverse Jet InjectionMMatute FDNo ratings yet
- Draft EIS for proposed Gorgon gas developmentDocument22 pagesDraft EIS for proposed Gorgon gas developmentMMatute FDNo ratings yet
- ANSYS CFX Tutorials 19.2Document910 pagesANSYS CFX Tutorials 19.2MMatute FDNo ratings yet
- 02 BoilDocument18 pages02 BoilWeb LogueandoNo ratings yet
- IC4 L2 OQ Question BankDocument4 pagesIC4 L2 OQ Question BankMMatute FD100% (1)
- Freddy Moncayo Homework Group 3Document2 pagesFreddy Moncayo Homework Group 3MMatute FDNo ratings yet
- How to Don and Doff Sterile Gloves SafelyDocument32 pagesHow to Don and Doff Sterile Gloves SafelyCoreen Mangaoang83% (6)
- Skills Checklist-Critical CareDocument3 pagesSkills Checklist-Critical CareRom Anog100% (4)
- Fitt Principle WorksheetsDocument5 pagesFitt Principle WorksheetsMae Ann Daganos0% (1)
- DFGHDocument6 pagesDFGHManuelEduardoSanchezSotoNo ratings yet
- Cutaneous Manifestations of Juvenile Onset Lupus Erythematosus: A Clinical StudyDocument5 pagesCutaneous Manifestations of Juvenile Onset Lupus Erythematosus: A Clinical StudyMaya SusantiNo ratings yet
- TC Electronic M-100 User ManualDocument21 pagesTC Electronic M-100 User Manualzewdaroo9599No ratings yet
- Blue Plains Plant Brochure PDFDocument7 pagesBlue Plains Plant Brochure PDFAfzal AhmadNo ratings yet
- Critical Care Update PDFDocument25 pagesCritical Care Update PDFHugo PozoNo ratings yet
- Soccer Class-Action Complaint - Aug. 27, 2014Document138 pagesSoccer Class-Action Complaint - Aug. 27, 2014Evan Buxbaum, CircaNo ratings yet
- RASA BooksDocument57 pagesRASA BooksArathy Krishna100% (1)
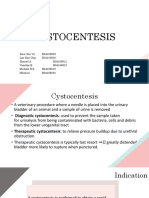
- Cystocentesis K4Document24 pagesCystocentesis K4Sze KhayNo ratings yet
- Spa CuisineDocument11 pagesSpa CuisineNamanraj Singh JollyNo ratings yet
- Module Four Wellness PlanDocument12 pagesModule Four Wellness Plankayle mylerNo ratings yet
- Revision 2Document7 pagesRevision 2Maina JonnNo ratings yet
- Effect of Prone Positioning on Respiratory Rate and Oxygen Saturation in Infants with RDSDocument3 pagesEffect of Prone Positioning on Respiratory Rate and Oxygen Saturation in Infants with RDSAgustina VivoNo ratings yet
- Medication Booklet and TicketDocument3 pagesMedication Booklet and TicketCayanne ChuaNo ratings yet
- Coe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Document23 pagesCoe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Alejandro MolinaNo ratings yet
- Baby Friendly Hospital Initiative (Bfhi)Document9 pagesBaby Friendly Hospital Initiative (Bfhi)Ankita BramheNo ratings yet
- Flow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlDocument4 pagesFlow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlAndreea DiaconuNo ratings yet
- Postpartum Health AssessmentDocument11 pagesPostpartum Health Assessmentapi-546355462No ratings yet
- Aefi - Mop 2014 FinalDocument106 pagesAefi - Mop 2014 FinalJethro Floyd QuintoNo ratings yet
- ISO Datasheet UE-71D10 Preliminary BMSTDocument1 pageISO Datasheet UE-71D10 Preliminary BMSTNamtien UsNo ratings yet
- Hip ExaminationDocument7 pagesHip ExaminationWaqas Haleem100% (1)
- R-07 Behaviour Policy (1536) PDFDocument1 pageR-07 Behaviour Policy (1536) PDFAmerNo ratings yet
- And Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!Document2 pagesAnd Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!kagnejukkeNo ratings yet
- Week 12-13-Group Activity-Conceptualizing A Possible GMODocument5 pagesWeek 12-13-Group Activity-Conceptualizing A Possible GMOAlexandra MandrezaNo ratings yet
- Cancer Screening Call ScriptDocument2 pagesCancer Screening Call Scriptjhez tel100% (1)
- Modes of Ventilation Chart - 1Document5 pagesModes of Ventilation Chart - 1Khamra SalahuddinNo ratings yet
- Referred PainDocument9 pagesReferred PainElsa Tamara SaragihNo ratings yet
- WIC Authorized Food List: Shopping GuideDocument17 pagesWIC Authorized Food List: Shopping GuideGanda PrajaNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Horse Training 101: Key Techniques for Every Horse OwnerFrom EverandHorse Training 101: Key Techniques for Every Horse OwnerRating: 4.5 out of 5 stars4.5/5 (27)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)