You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Aviva Natural Medicine CabinetDocument2 pagesAviva Natural Medicine Cabinetjayjonbeach100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
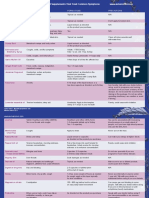
- Psychiatric Nursing Questionares With Rationale 1Document23 pagesPsychiatric Nursing Questionares With Rationale 1Tsuyoshi Bang100% (2)
- FieldManual A Field Manual For Collection of Specimens To Enhance Diagnosis of Animal Diseases PDFDocument150 pagesFieldManual A Field Manual For Collection of Specimens To Enhance Diagnosis of Animal Diseases PDFrazadrpkNo ratings yet
- CastDocument7 pagesCastRegina Nina YoshidaNo ratings yet
- Bound Tree Active Shooter Response EbookDocument17 pagesBound Tree Active Shooter Response EbookVein100% (1)
- Concept of Disease CausationDocument44 pagesConcept of Disease CausationShivani Dhillon100% (2)
- Radiation Protection Bushong Study GuideDocument6 pagesRadiation Protection Bushong Study GuideAsha6842100% (1)
- Neurologic ProblemsDocument11 pagesNeurologic ProblemsFilipino Nurses Central67% (3)
- The Four Phases of The Menstrual CycleDocument6 pagesThe Four Phases of The Menstrual CyclepenfoNo ratings yet
- Welcome Letter For FamiliesDocument3 pagesWelcome Letter For FamiliesChild and Family InstituteNo ratings yet
- The Death of An EmperorDocument20 pagesThe Death of An EmperorabbasNo ratings yet
- Nampath MonositDocument8 pagesNampath MonositEllya Latifah IlyasNo ratings yet
- Normal Leukocyte CountDocument1 pageNormal Leukocyte CountEllya Latifah IlyasNo ratings yet
- Daftar Pustaka: Medicine, 4 (18), Pp. 338-344. DOIDocument1 pageDaftar Pustaka: Medicine, 4 (18), Pp. 338-344. DOIEllya Latifah IlyasNo ratings yet
- Fase HemopoiesisDocument35 pagesFase HemopoiesisEllya Latifah IlyasNo ratings yet
- Curley 2018 Platelet Transfusion Threshols in NeonatesDocument11 pagesCurley 2018 Platelet Transfusion Threshols in NeonatesEllya Latifah IlyasNo ratings yet
- Applied Statistics Survival AnalysisDocument23 pagesApplied Statistics Survival AnalysisOneng IfayaniNo ratings yet
- Ukdi AgustusDocument31 pagesUkdi AgustusnahdiaNo ratings yet
- Morbidity, Mortality and Management of Wheat Pill Poisoning: Background: MethodsDocument5 pagesMorbidity, Mortality and Management of Wheat Pill Poisoning: Background: MethodsAamir ShahzadNo ratings yet
- School Health & Preventive Care Programs in India Jarma WellnessDocument3 pagesSchool Health & Preventive Care Programs in India Jarma WellnessJarma WellnessNo ratings yet
- Appendix 4M - Paediatric Emergency MedicineDocument21 pagesAppendix 4M - Paediatric Emergency MedicineEssam HassanNo ratings yet
- Coronavirus: There Is A Current Outbreak of Coronavirus (COVID-19) DiseaseDocument5 pagesCoronavirus: There Is A Current Outbreak of Coronavirus (COVID-19) DiseaseLuna BellatrixNo ratings yet
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Document155 pagesColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- Example 001Document17 pagesExample 001Bhavana GangurdeNo ratings yet
- Helping Patient With WoundDocument3 pagesHelping Patient With WoundSevina Eka ChannelNo ratings yet
- Klasifikasi Tumor Jaringan Lunak PDFDocument10 pagesKlasifikasi Tumor Jaringan Lunak PDFzakibonnie100% (1)
- Concept Map Cabg PTDocument8 pagesConcept Map Cabg PTapi-607926939No ratings yet
- Abstract IctromiDocument2 pagesAbstract Ictromiyayasan harapan ummatNo ratings yet
- Respiration Course ObjectivesDocument8 pagesRespiration Course Objectivesjoshy220996No ratings yet
- Thesis 2019Document8 pagesThesis 2019Kim YunaNo ratings yet
- Chaves 2020Document10 pagesChaves 2020Matheus CastroNo ratings yet
- General Surgery Examination and Board Review 1St Edition Robert B Lim Full ChapterDocument51 pagesGeneral Surgery Examination and Board Review 1St Edition Robert B Lim Full Chapterrichard.mowatt659100% (20)
- Medical Times v20 1000031612 PDFDocument494 pagesMedical Times v20 1000031612 PDFLouise StagnoNo ratings yet
- Uts Bahasa Inggris Ii Semester IiDocument4 pagesUts Bahasa Inggris Ii Semester Iibintang pamungkasNo ratings yet
- Brachytherapy Applicator and Accessory GuideDocument127 pagesBrachytherapy Applicator and Accessory GuideIsaura CarvajalNo ratings yet