You might also like
- Project Management Bo Tonnquist ENGDocument168 pagesProject Management Bo Tonnquist ENGIgor Brodin63% (8)
- TASK 2 - BSBMGT517 Manage Operational Plan TASK 2 - BSBMGT517 Manage Operational PlanDocument14 pagesTASK 2 - BSBMGT517 Manage Operational Plan TASK 2 - BSBMGT517 Manage Operational PlanVioleta Hoyos Lopez68% (19)
- Quotation For Geotechnical Investigation & Topography, Sardar Mohammad Dawood Khan Hospital, Dec 2018Document1 pageQuotation For Geotechnical Investigation & Topography, Sardar Mohammad Dawood Khan Hospital, Dec 2018fereydoun nasratzadaNo ratings yet
- 0417 - 118T3293 Cooling Sealing AirDocument6 pages0417 - 118T3293 Cooling Sealing AirfaisalnadimNo ratings yet
- Engineering Economy - EEDocument68 pagesEngineering Economy - EEMaricarLogronioSalazar100% (1)
- Joy Film - Guided Viewing Questions & AnalysisDocument6 pagesJoy Film - Guided Viewing Questions & AnalysisMichael MarquisNo ratings yet
- Asian Fabricx Company ProfileDocument5 pagesAsian Fabricx Company ProfileSenthuran MBANo ratings yet
- Indian Institute of Foreign Trade Programme: EPGDIB (Online) 2021-2022 Mid Term Examination Human Resource ManagementDocument2 pagesIndian Institute of Foreign Trade Programme: EPGDIB (Online) 2021-2022 Mid Term Examination Human Resource ManagementsahilnhnNo ratings yet
- Consumer Behaviour in Chocolate IndustryDocument4 pagesConsumer Behaviour in Chocolate IndustryJay DabhiNo ratings yet
- Reporting Formats For TSP 16-17-Vol1-30Jun16Document1 pageReporting Formats For TSP 16-17-Vol1-30Jun16MuraliKrishna NaiduNo ratings yet
- Grupo de Potência HidráulicaDocument24 pagesGrupo de Potência HidráulicaelizeuNo ratings yet
- Gantt Team Project Chart TemplateDocument1 pageGantt Team Project Chart TemplateVitor FirmoNo ratings yet
- TB Ro: Dr. Aryo WibowoDocument7 pagesTB Ro: Dr. Aryo WibowoAryoWibowoNo ratings yet
- Semiconductor Sector Update: Kick Starting The NKEA-15/10/2010Document2 pagesSemiconductor Sector Update: Kick Starting The NKEA-15/10/2010Rhb InvestNo ratings yet
- SJ117219Document1 pageSJ117219sheecheong01No ratings yet
- 1635930426.0410814 - Citybank 2021 Q3Document1 page1635930426.0410814 - Citybank 2021 Q3Omar FarukNo ratings yet
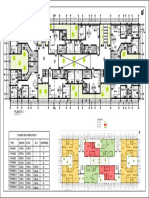
- B D A C' H E F G I: Primera PlantaDocument1 pageB D A C' H E F G I: Primera PlantaHaile Huaman GuzmanNo ratings yet
- Anandam Manufacturing Company.1Document2 pagesAnandam Manufacturing Company.1AkshitNo ratings yet
- Rencana AC Atap: Skala 1: 200Document1 pageRencana AC Atap: Skala 1: 200BellindaClaudyaNo ratings yet
- DTS Sheet 2 ComponentDocument1 pageDTS Sheet 2 ComponenthimanshuNo ratings yet
- R 1 - 420x594 3ex Negru PDFDocument1 pageR 1 - 420x594 3ex Negru PDFconstantin ciobanuNo ratings yet
- 03 URS GENERATED FORMAT FAR No. 4 March 2021Document2 pages03 URS GENERATED FORMAT FAR No. 4 March 2021Mark AlbaNo ratings yet
- F-AIRFIELD FIRE FIGHTING ENGINEERING-C20 - Reviewed-RRDocument6 pagesF-AIRFIELD FIRE FIGHTING ENGINEERING-C20 - Reviewed-RRsokeara phoungNo ratings yet
- Timesheet Mês de Setembro - 2022Document1 pageTimesheet Mês de Setembro - 2022Idiamine Da Alzira SKNo ratings yet
- Part 2 A1 (Workshop Crane) PDFDocument1 pagePart 2 A1 (Workshop Crane) PDFAritra GoswamiNo ratings yet
- Investment Analysis Example ReportDocument28 pagesInvestment Analysis Example ReportOwenNo ratings yet
- SJ 121220Document1 pageSJ 121220fit asmarufNo ratings yet
- Form - T: Combined Muster Roll Cum Register of WagesDocument2 pagesForm - T: Combined Muster Roll Cum Register of WageskapilvarshaNo ratings yet
- TECH-7 Work Schedule SampleDocument1 pageTECH-7 Work Schedule SamplemarkNo ratings yet
- VIP Building Ground Floor-Lighting Layout - MEP-EL-GF-01Document1 pageVIP Building Ground Floor-Lighting Layout - MEP-EL-GF-01AmulyaRajbharNo ratings yet
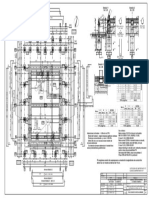
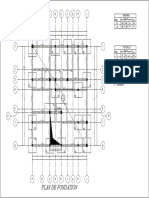
- Plan de FondationDocument1 pagePlan de FondationBoris Djomo HappiNo ratings yet
- Arbore CompletDocument1 pageArbore CompletAlex KiduNo ratings yet
- How To Read A Value Line ReportDocument15 pagesHow To Read A Value Line ReportJamie GiannaNo ratings yet
- 029 025 A A3 Scaff Wall Position CheckDocument1 page029 025 A A3 Scaff Wall Position Checksales.honestcoNo ratings yet
- PHASE II - Construction Supervision and Contract Management PHASE I - Design and Preparation of Tender Documents Defect Liability Period (12 Months)Document4 pagesPHASE II - Construction Supervision and Contract Management PHASE I - Design and Preparation of Tender Documents Defect Liability Period (12 Months)Anonymous Xb3zHioNo ratings yet
- Wurth WR-BHD 61202023021 IDC JTag Connecteur 2x10pinDocument6 pagesWurth WR-BHD 61202023021 IDC JTag Connecteur 2x10pinSupportNo ratings yet
- MPIND00190710000012060 NewDocument3 pagesMPIND00190710000012060 NewStore PurchaseNo ratings yet
- This Is New PDFDocument1 pageThis Is New PDFAnonymous BZQOJwWIh6No ratings yet
- 13.8Kv U/V Load Shedding Panel-2 +uvls.2: D HA555 P 3-1313003.03 EA-383186 4400004656Document1 page13.8Kv U/V Load Shedding Panel-2 +uvls.2: D HA555 P 3-1313003.03 EA-383186 4400004656Anonymous BZQOJwWIh6No ratings yet
- DD-N-00426-3-01-DDCMS-C-15-STRU-312-2-P-01 - First Floor - Slab Layout & Details (Sh-2) - RA-312-2Document1 pageDD-N-00426-3-01-DDCMS-C-15-STRU-312-2-P-01 - First Floor - Slab Layout & Details (Sh-2) - RA-312-2SivaAgathamudiNo ratings yet
- Treble: Ampeg Ba110 Schematic Loud TechnologiesDocument1 pageTreble: Ampeg Ba110 Schematic Loud Technologiesjesus fuentesNo ratings yet
- P Okitm07 329 03 Eqd 2003 1Document1 pageP Okitm07 329 03 Eqd 2003 1ismiasyofNo ratings yet
- WBDGP13820000000000419 NewDocument6 pagesWBDGP13820000000000419 NewAnup RouthNo ratings yet
- Zssat Far 4Document1 pageZssat Far 4Nicole SilorioNo ratings yet
- Brain Dead MPPTDocument1 pageBrain Dead MPPTWrhik Bhattacharyya100% (1)
- MOEB2015SEP Results PDFDocument119 pagesMOEB2015SEP Results PDFppgpcsNo ratings yet
- SS 3Document1 pageSS 3Nathalie EvineNo ratings yet
- Investrust Space Plan A001Document1 pageInvestrust Space Plan A001Mr. SwiftNo ratings yet
- Z15Arq N2Document1 pageZ15Arq N2LCNo ratings yet
- Jasch Industries Dec 2021 ResultsDocument10 pagesJasch Industries Dec 2021 ResultsPuneet367No ratings yet
- R12 T07B24 Ifmi XX XX SDW El 00063Document1 pageR12 T07B24 Ifmi XX XX SDW El 00063Abrar DigitalNo ratings yet
- A-814-Flooring Layout First Floor - MosqueDocument1 pageA-814-Flooring Layout First Floor - MosqueEmmanuel InfanteNo ratings yet
- Echame A Mi La Culpa-Albert HammondDocument2 pagesEchame A Mi La Culpa-Albert HammondRafael SanchezNo ratings yet
- HSE Dashboard For Multiple SitessDocument11 pagesHSE Dashboard For Multiple SitessAfroz Alam0% (1)
- P20c40ug01prw Mmso Civtundwg 14003 1Document1 pageP20c40ug01prw Mmso Civtundwg 14003 1subhash kumarNo ratings yet
- G026a-Pv-15001 String Wiring Layout Block 1-15001Document1 pageG026a-Pv-15001 String Wiring Layout Block 1-15001Daniel BanawaNo ratings yet
- Sssar2010low 120222214841 Phpapp02 PDFDocument31 pagesSssar2010low 120222214841 Phpapp02 PDFKhaela MercaderNo ratings yet
- TNMAS00508200000016682 NewDocument2 pagesTNMAS00508200000016682 NewHakkeem saitNo ratings yet
- Jose Abad Santos Es - Aip Cy 2022Document4 pagesJose Abad Santos Es - Aip Cy 2022Jay Ar Lanon EgangNo ratings yet
- Absensi JUNI 2022Document1 pageAbsensi JUNI 2022Luqman KaitoNo ratings yet
- Planta 1: LeyendaDocument1 pagePlanta 1: LeyendaAnderson johan Espinoza malcaNo ratings yet
- Option C: 1+2 Way Road: Lake Street Shared TrailDocument1 pageOption C: 1+2 Way Road: Lake Street Shared TrailNeenNo ratings yet
- LSGG VacDocument2 pagesLSGG Vacsamykarim2009No ratings yet
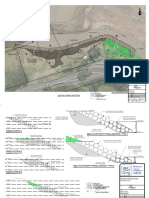
- Sandy Bay Erosion Protection Eng Consent Dwgs RevD 2018-12-12Document4 pagesSandy Bay Erosion Protection Eng Consent Dwgs RevD 2018-12-12Stuff NewsroomNo ratings yet
- S-23-01 Saraswati Singh TKDocument3 pagesS-23-01 Saraswati Singh TKTanweer KhanNo ratings yet
- 8021 1 1 1.30ka4Document2 pages8021 1 1 1.30ka4julianvanraalteNo ratings yet
- CBTRY20022480000010034 NewDocument2 pagesCBTRY20022480000010034 Newkarthikeyan PNo ratings yet
- UNDP/Gender Equality Project LOA Staff: National LevelDocument2 pagesUNDP/Gender Equality Project LOA Staff: National Levelfereydoun nasratzadaNo ratings yet
- 1update LOA Staff ListDocument2 pages1update LOA Staff Listfereydoun nasratzadaNo ratings yet
- 1revised LoA Tracking Table June 3 2012Document3 pages1revised LoA Tracking Table June 3 2012fereydoun nasratzadaNo ratings yet
- Gender Equality Project - Regional StaffDocument8 pagesGender Equality Project - Regional Stafffereydoun nasratzadaNo ratings yet
- List of Personnel Recruited by Government and Paid by UNDP - July 2012Document1 pageList of Personnel Recruited by Government and Paid by UNDP - July 2012fereydoun nasratzadaNo ratings yet
- Jack Monroe On Twitter - Woke Up This Morning To The RadioDocument9 pagesJack Monroe On Twitter - Woke Up This Morning To The RadioToni PrugNo ratings yet
- Venture Capital & Ventre Capitalist: Made By: Gagan Vats Priyanka Tuteja Achal Jain Akshat DhallDocument24 pagesVenture Capital & Ventre Capitalist: Made By: Gagan Vats Priyanka Tuteja Achal Jain Akshat DhalltarunshridharNo ratings yet
- Olaf Abel Ethylene ApcDocument32 pagesOlaf Abel Ethylene Apcasamad54No ratings yet
- The-One-Day-Audit-5-Real-Life-ExamplesDocument4 pagesThe-One-Day-Audit-5-Real-Life-ExamplesDawson EllisonNo ratings yet
- Stock Market Portfolio ProjectDocument3 pagesStock Market Portfolio ProjectTaquee MahmoodNo ratings yet
- LoanDocument1 pageLoansuriya bhaiNo ratings yet
- Insurance Surveyors and Loss AssessorsDocument16 pagesInsurance Surveyors and Loss AssessorssarathlalNo ratings yet
- DeKalb County Commissioners Chief of Staff Morris Williams P-Card ActivityDocument37 pagesDeKalb County Commissioners Chief of Staff Morris Williams P-Card ActivityViola DavisNo ratings yet
- CDR Mechanical Engineer 1 No SummaryDocument24 pagesCDR Mechanical Engineer 1 No SummaryZizo Awad100% (1)
- 1 CISSP 1er Dummy Examen Respuestas y Explicaciones - QADocument58 pages1 CISSP 1er Dummy Examen Respuestas y Explicaciones - QAIvan MartinezNo ratings yet
- Joselito Resumae UpdatedDocument8 pagesJoselito Resumae Updatedjoselito ruantoNo ratings yet
- Sem-1 Syllabus Distribution 2021Document2 pagesSem-1 Syllabus Distribution 2021Kishan JhaNo ratings yet
- Foundations of Business LawDocument3 pagesFoundations of Business LawAmandeep Singh100% (1)
- Bam 040 Demand and Supply PT.2Document14 pagesBam 040 Demand and Supply PT.2Vkyla BataoelNo ratings yet
- Accounting Cycle Service BusinessDocument120 pagesAccounting Cycle Service BusinessElla Mae AcostaNo ratings yet
- D15 Hybrid P1 QPDocument6 pagesD15 Hybrid P1 QPShaameswary AnnadoraiNo ratings yet
- C TSCM62 65 Sample QuestionsDocument7 pagesC TSCM62 65 Sample QuestionsAnand Iyer100% (2)
- Ellis CAMPBELL, JR., Director of Internal Revenue For The Second Collection District of Texas, v. William A. SAILER and Wife, Patricia O'Leary SailerDocument4 pagesEllis CAMPBELL, JR., Director of Internal Revenue For The Second Collection District of Texas, v. William A. SAILER and Wife, Patricia O'Leary SailerScribd Government DocsNo ratings yet
- Group Asignment Questions LawDocument3 pagesGroup Asignment Questions LawKcaj WongNo ratings yet
- Cash Management: Strategies To Manage CashDocument6 pagesCash Management: Strategies To Manage CashRamalingam ChandrasekharanNo ratings yet
- Accounting AssmntDocument11 pagesAccounting AssmntasadNo ratings yet
- Final COP-Section 1Document86 pagesFinal COP-Section 1Arbaz KhanNo ratings yet
- Investment Decision RulesDocument14 pagesInvestment Decision RulesprashantgoruleNo ratings yet