You might also like
- Clinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingDocument7 pagesClinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingNazia BhatNo ratings yet
- Serrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyDocument4 pagesSerrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyclaudyNo ratings yet
- Presentation Clinical Spectrum and Chromosomal Abnormalities of Children With Turner 1251Document6 pagesPresentation Clinical Spectrum and Chromosomal Abnormalities of Children With Turner 1251Mai SomaaNo ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Evaluation and Management of Cholelithiasis in Children: A Hospital Based StudyDocument6 pagesEvaluation and Management of Cholelithiasis in Children: A Hospital Based StudyangelaanapakuNo ratings yet
- WJMH 32 110Document6 pagesWJMH 32 110Yacine Tarik AizelNo ratings yet
- Manuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesDocument4 pagesManuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesHerman FiraNo ratings yet
- Clinical Spectrum of Disorders of Sexual Differentiation: Original ArticleDocument5 pagesClinical Spectrum of Disorders of Sexual Differentiation: Original ArticleInne CarolineNo ratings yet
- Scenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsDocument5 pagesScenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- 407 PDFDocument4 pages407 PDFSrideviRaviNo ratings yet
- Research Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryDocument5 pagesResearch Article: Spectrum of Intracerebral Hemorrhage in Children: A Report From PICU of A Resource Limited CountryAyu Septiari ArtatiNo ratings yet
- Ghidini Et Al-2018-Prenatal DiagnosisDocument18 pagesGhidini Et Al-2018-Prenatal Diagnosismeaad kahtanNo ratings yet
- Findings Regarding Non-Sexual Penile Fracture in A Referral Emergency HospitalDocument7 pagesFindings Regarding Non-Sexual Penile Fracture in A Referral Emergency HospitalRENENo ratings yet
- Leiomyoma Types, Incidence and Clinical Presentation - A Study at A Tertiary Care HospitalDocument6 pagesLeiomyoma Types, Incidence and Clinical Presentation - A Study at A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- A Retrospective Research Study On The Positive Impacts of Morbidity and Mortality (M&M) Forums On The Overall Medical Profession and Patient CareDocument6 pagesA Retrospective Research Study On The Positive Impacts of Morbidity and Mortality (M&M) Forums On The Overall Medical Profession and Patient CareiajpsNo ratings yet
- Clinical Outcomes in A Specialist Male Genital Skin Clinic: Prospective Follow-Up of 600 PatientsDocument5 pagesClinical Outcomes in A Specialist Male Genital Skin Clinic: Prospective Follow-Up of 600 PatientsMeta SakinaNo ratings yet
- Semen AnalysisDocument4 pagesSemen AnalysisHamid IqbalNo ratings yet
- Resurgence of Diphtheria: Clinical Profile and Outcome - A Retrospective Observational StudyDocument4 pagesResurgence of Diphtheria: Clinical Profile and Outcome - A Retrospective Observational StudyLestari LifaNo ratings yet
- Tubal Abnormalities in Thai Infertile FemalesDocument5 pagesTubal Abnormalities in Thai Infertile FemalesMor OB-GYNNo ratings yet
- IUFD Incidence Causes and Complications A RetrospeDocument6 pagesIUFD Incidence Causes and Complications A Retrospeadri20121989No ratings yet
- Systematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenDocument4 pagesSystematic Review On Recognising Patterns in Incidence of Polycystic Ovarian Syndrome in Young WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Issm Prisma ChecklistDocument9 pagesIssm Prisma ChecklistInnani Wildania HusnaNo ratings yet
- Association Between Location of Thyroid Nodule and Risk of MalignancyDocument4 pagesAssociation Between Location of Thyroid Nodule and Risk of MalignancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Maternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanDocument12 pagesMaternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanIJAR JOURNALNo ratings yet
- Ogi2019 9465375Document6 pagesOgi2019 9465375Novi HermanNo ratings yet
- Pregnant Women's Attitudes Toward UltrasoundDocument6 pagesPregnant Women's Attitudes Toward Ultrasoundelda zulkarnainNo ratings yet
- Scientific Journal of Neurology & NeurosurgeryDocument5 pagesScientific Journal of Neurology & NeurosurgerySciresNo ratings yet
- PrimaryCareProviderAwarenessofIR-A Single-Center AnalysisDocument8 pagesPrimaryCareProviderAwarenessofIR-A Single-Center AnalysisQueen Arlene BeeNo ratings yet
- Jurnal BEDocument6 pagesJurnal BEM Ali AdrianNo ratings yet
- Sexual Habits and Clinico-Etiological Profile of Sexually Transmitted Diseases in NepalDocument7 pagesSexual Habits and Clinico-Etiological Profile of Sexually Transmitted Diseases in NepalMuhammad TariqNo ratings yet
- Functional Assesment of Patients With AIDS DiseaseDocument6 pagesFunctional Assesment of Patients With AIDS DiseaseLilian RamineNo ratings yet
- Eritroderma EpidemiologyDocument6 pagesEritroderma EpidemiologyAhmad Ligar SuhermanNo ratings yet
- Pituitary Incidentalomas Best Practices and Looking AheadDocument9 pagesPituitary Incidentalomas Best Practices and Looking AheadJulieta LopezNo ratings yet
- Spectrum of Symptoms in Women Diagnosed With Endometriosis During Adolescence Vs AdulthoodDocument11 pagesSpectrum of Symptoms in Women Diagnosed With Endometriosis During Adolescence Vs AdulthoodnicloverNo ratings yet
- The Diagnostic Criteria For Chronic EndometritisDocument7 pagesThe Diagnostic Criteria For Chronic EndometritisyuriescaidaNo ratings yet
- David A Goldfarb Renal Transplantation 2021Document2 pagesDavid A Goldfarb Renal Transplantation 2021alan.rangel.puenteNo ratings yet
- Hairdressing Processes As Well As Head of Hair Morphology A New ClinicoMicroscopic Comparison Examinemzgqc PDFDocument1 pageHairdressing Processes As Well As Head of Hair Morphology A New ClinicoMicroscopic Comparison Examinemzgqc PDFborderkayak0No ratings yet
- Journal of Pediatric Surgery: Emanuele Trovalusci, Marco Rossato, Piergiorgio Gamba, Paola MidrioDocument7 pagesJournal of Pediatric Surgery: Emanuele Trovalusci, Marco Rossato, Piergiorgio Gamba, Paola MidrioAde Triansyah EmsilNo ratings yet
- Gajms 42 34-38Document6 pagesGajms 42 34-38Raden Ayu Miftah CahyaniNo ratings yet
- Gynecology & Reproductive HealthDocument6 pagesGynecology & Reproductive HealthtiaranindyNo ratings yet
- Clinico-Histopathological Study of Endometrium With and Without Hormone Therapy in Patients Withabnormal Uterine BleedingDocument6 pagesClinico-Histopathological Study of Endometrium With and Without Hormone Therapy in Patients Withabnormal Uterine BleedingIJAR JOURNALNo ratings yet
- Treatment Outcome and Mortality: Their Predictors Among HIV/TB Co-Infected Patients From IranDocument5 pagesTreatment Outcome and Mortality: Their Predictors Among HIV/TB Co-Infected Patients From Iranali aliNo ratings yet
- Teenage Sexual Health in A Uk Community Genitourinary (Gu) Medicine Clinic-Can We Improve Further?Document7 pagesTeenage Sexual Health in A Uk Community Genitourinary (Gu) Medicine Clinic-Can We Improve Further?mominamalikNo ratings yet
- 1.managemen ExploreDocument5 pages1.managemen ExploreRiski YustitiaNo ratings yet
- Study of Congenital Heart Disease in Neonates: Clinical Profile, Diagnosis, Immediate Outcome and Short-Term Follow-UpDocument6 pagesStudy of Congenital Heart Disease in Neonates: Clinical Profile, Diagnosis, Immediate Outcome and Short-Term Follow-UpDhiaul IzzahNo ratings yet
- A Study of Inguinal Hernia in ChildrenDocument5 pagesA Study of Inguinal Hernia in ChildrenrhmathidayatNo ratings yet
- Management of Cryptorchidism: A Survey of Clinical Practice in ItalyDocument8 pagesManagement of Cryptorchidism: A Survey of Clinical Practice in ItalyHamdan Yuwafi NaimNo ratings yet
- Sadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte MaryamDocument7 pagesSadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte Maryamgamal attamNo ratings yet
- Spectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South IndiaDocument4 pagesSpectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South Indianikhil00007No ratings yet
- Vitiligo ObatDocument6 pagesVitiligo ObatLidwina DewiNo ratings yet
- Tayeb I 2017Document8 pagesTayeb I 2017Essay NationNo ratings yet
- Work ExposureDocument5 pagesWork ExposureJaved IqbalNo ratings yet
- ArticleDocument16 pagesArticleobbyNo ratings yet
- 74566-Article Text-168163-1-10-20120307Document4 pages74566-Article Text-168163-1-10-20120307Lawrence MungaNo ratings yet
- Spermatic Dna Fragmentation Index of Infertile Men: Interest in The Choice of Pma Technique Preliminary StudyDocument7 pagesSpermatic Dna Fragmentation Index of Infertile Men: Interest in The Choice of Pma Technique Preliminary StudyIJAR JOURNALNo ratings yet
- Risk Factors for Hepatitis B in Northern PakistanDocument3 pagesRisk Factors for Hepatitis B in Northern PakistanDr Alamzeb JadoonNo ratings yet
- Amenore PrimerDocument4 pagesAmenore PrimerHamka KoersloNo ratings yet
- Endometriosis in Menopause A Single Institution ExperienceDocument5 pagesEndometriosis in Menopause A Single Institution ExperienceMartin Romero Torres100% (1)
- Venkatraman KDocument3 pagesVenkatraman KRana Zara AthayaNo ratings yet
- Fullpapers Bik376117be181fullDocument6 pagesFullpapers Bik376117be181fullIGusti Ngurah AgungNo ratings yet
- Fullpapers Bik376117be181fullDocument6 pagesFullpapers Bik376117be181fullIGusti Ngurah AgungNo ratings yet
- Vitamin C Content Declines With Increased Paprika Heating TimeDocument7 pagesVitamin C Content Declines With Increased Paprika Heating Timeyerich septaNo ratings yet
- 41166-Article Text-144398-1-10-20190506 PDFDocument5 pages41166-Article Text-144398-1-10-20190506 PDFyerich septaNo ratings yet
- Pump It Up XX Unlock RequirementsDocument4 pagesPump It Up XX Unlock Requirementsyerich septa60% (5)
- 731 1547 1 SMDocument4 pages731 1547 1 SMiccakn.No ratings yet
- Tuberculosis Verrucosa Cutis: Case Report of A Diagnostic ChallengeDocument4 pagesTuberculosis Verrucosa Cutis: Case Report of A Diagnostic Challengeyerich septaNo ratings yet
- AmerDocument97 pagesAmeryerich septaNo ratings yet
- ArtikelDocument14 pagesArtikelyerich septaNo ratings yet
- Bno IvpDocument9 pagesBno Ivpyerich septaNo ratings yet
- 1 s2.0 S1015958417304232 MainDocument9 pages1 s2.0 S1015958417304232 Mainyerich septaNo ratings yet
- Undescended Testis: Ravibindu RanawakaDocument2 pagesUndescended Testis: Ravibindu RanawakaBrianne LeeNo ratings yet
- Buah Mengkudu (Morinda Citrifolia L.) Sebagai Pengadsorbsi Minyak Jealantah Noni (Morinda Citrifolia L.) Fruit As Adsorbent For Cooking OilDocument9 pagesBuah Mengkudu (Morinda Citrifolia L.) Sebagai Pengadsorbsi Minyak Jealantah Noni (Morinda Citrifolia L.) Fruit As Adsorbent For Cooking Oilyerich septaNo ratings yet
- AmerDocument97 pagesAmeryerich septaNo ratings yet
- AmerDocument97 pagesAmeryerich septaNo ratings yet
- Urological Science: Jiun-Hung Geng, Chun-Nung HuangDocument4 pagesUrological Science: Jiun-Hung Geng, Chun-Nung Huangyerich septaNo ratings yet
- Revisiting Donor Risk Over Two Decades of Single-Center Experience: More Attention On The Impact of OverweightDocument8 pagesRevisiting Donor Risk Over Two Decades of Single-Center Experience: More Attention On The Impact of Overweightyerich septaNo ratings yet
- Undescended Testis in Adult Epidemiology and TheraDocument8 pagesUndescended Testis in Adult Epidemiology and Therayerich septaNo ratings yet
- Role of Primary Chemotherapy in Management of LargDocument4 pagesRole of Primary Chemotherapy in Management of Largyerich septaNo ratings yet
- Laparoscopic Transabdominal Preperitoneal Approach For Giant Inguinal HerniasDocument6 pagesLaparoscopic Transabdominal Preperitoneal Approach For Giant Inguinal Herniasyerich septaNo ratings yet
- DKT Herbal Drug Impact on LDLT OutcomesDocument5 pagesDKT Herbal Drug Impact on LDLT Outcomesyerich septaNo ratings yet
- 1 s2.0 S1015958417305833 MainDocument7 pages1 s2.0 S1015958417305833 Mainyerich septaNo ratings yet
- Diagnosisdan Penatalaksanaan Undescended TestisDocument8 pagesDiagnosisdan Penatalaksanaan Undescended Testisyerich septaNo ratings yet
- 1 s2.0 S1015958417304402 MainDocument6 pages1 s2.0 S1015958417304402 Mainyerich septaNo ratings yet
- Bells PalsyDocument15 pagesBells PalsyChandra ManapaNo ratings yet
- Cover + No KatalogDocument2 pagesCover + No KatalogMifti SyawaliNo ratings yet
- Laryngopharyngeal Reflux A Syndrome That Mimics AsthmaDocument3 pagesLaryngopharyngeal Reflux A Syndrome That Mimics Asthmayerich septaNo ratings yet
- 1 s2.0 S101595841730622X MainDocument7 pages1 s2.0 S101595841730622X Mainyerich septaNo ratings yet
- DR. NINEVETCH CRUZ, Petitioner, vs. COURT OF APPEALS and LYDIA UMALI, Respondents.Document1 pageDR. NINEVETCH CRUZ, Petitioner, vs. COURT OF APPEALS and LYDIA UMALI, Respondents.Charles Roger RayaNo ratings yet
- (PDF) Influence of TORCH Infections in First Trimester Miscarriage in The Malabar Region of KeralaDocument16 pages(PDF) Influence of TORCH Infections in First Trimester Miscarriage in The Malabar Region of KeralaleartaNo ratings yet
- Dr. Siva Narayan Reddy Vennapusa - Best NeonatoloDocument1 pageDr. Siva Narayan Reddy Vennapusa - Best Neonatolokranthikumar510No ratings yet
- Resume Katelyn DustmanDocument2 pagesResume Katelyn Dustmanapi-546593615No ratings yet
- Vulnerable Patient Sop FinalDocument28 pagesVulnerable Patient Sop FinalManglemba Moirangthem100% (1)
- Nellcor Oximax Technology ProductDocument8 pagesNellcor Oximax Technology ProductSwami MeeraNo ratings yet
- Ross Rosen ResumeDocument4 pagesRoss Rosen ResumeKanak SoniNo ratings yet
- Health 10 MODULE2Document6 pagesHealth 10 MODULE2armand bayoranNo ratings yet
- Physician's Notes and OrdersDocument2 pagesPhysician's Notes and OrdersEunick VillagraciaNo ratings yet
- Hh2sgonzupzxf4gu1w1wym1fDocument1 pageHh2sgonzupzxf4gu1w1wym1fHarsh AryaNo ratings yet
- Avian Medicine and Surgery, 2nd Edition, Self-Assessment Color Review PDFDocument384 pagesAvian Medicine and Surgery, 2nd Edition, Self-Assessment Color Review PDFSilvana MartinezNo ratings yet
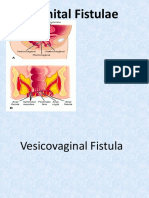
- Fistula GenitaliaDocument35 pagesFistula GenitaliaFifi FruitasariNo ratings yet
- 7 Scott NgaiDocument21 pages7 Scott Ngaiapi-220705744No ratings yet
- Critical Care in Obstetrics Guideline: NHSCT/12/515Document10 pagesCritical Care in Obstetrics Guideline: NHSCT/12/515ana mariaNo ratings yet
- ACS Doctors Naples Feb2017Document21 pagesACS Doctors Naples Feb2017IvonneNo ratings yet
- Certified Nurse Anesthetist (CRNA)Document4 pagesCertified Nurse Anesthetist (CRNA)api-78920101No ratings yet
- Remifentanil Use in Anaesthesia and Critical Care: Basic Science Tutorial 342Document9 pagesRemifentanil Use in Anaesthesia and Critical Care: Basic Science Tutorial 342khalidNo ratings yet
- Asymptomatic Endometrial Thickness PDFDocument10 pagesAsymptomatic Endometrial Thickness PDFkukadiyaNo ratings yet
- Effect of Different Types of Textiles On Sexual Activity of RatsDocument6 pagesEffect of Different Types of Textiles On Sexual Activity of RatsDavid MoyeNo ratings yet
- The Light of My EyeDocument3 pagesThe Light of My EyePaul Marfil100% (1)
- Practical ProceduresDocument315 pagesPractical ProceduresAnil SoodNo ratings yet
- Clinical Guidelines on Intrapartum and Postpartum CareDocument52 pagesClinical Guidelines on Intrapartum and Postpartum CareAngela SaldajenoNo ratings yet
- Garbhini Paricharya: (Regimen For The Pregnant Woman)Document3 pagesGarbhini Paricharya: (Regimen For The Pregnant Woman)JDSJJDNo ratings yet
- Induction Ceremony Emcee ScriptDocument5 pagesInduction Ceremony Emcee Scriptyg love91% (11)
- 10-16-01 Cleft Lip and Palate Part 1Document52 pages10-16-01 Cleft Lip and Palate Part 1Zoilo NuñezNo ratings yet
- (10920684 - Neurosurgical Focus) Novel Technique For Trialing Peripheral Nerve Stimulation - Ultrasonography-Guided StimuCath TrialDocument7 pages(10920684 - Neurosurgical Focus) Novel Technique For Trialing Peripheral Nerve Stimulation - Ultrasonography-Guided StimuCath TrialSebastiano SerraNo ratings yet
- ExEm Foam KitDocument1 pageExEm Foam KitferdinandexNo ratings yet
- Travel Report IVTDocument3 pagesTravel Report IVTNiña Ceniza CalatravaNo ratings yet
- The Optical Quality of The CorneaDocument32 pagesThe Optical Quality of The CorneaacalossiNo ratings yet
- Menstrual DisorderDocument36 pagesMenstrual DisorderPrayogi KramyNo ratings yet