You might also like
- A Cure For Cancer Hidden in Plain Sight July 2019 DR David WilliamsDocument8 pagesA Cure For Cancer Hidden in Plain Sight July 2019 DR David WilliamsThomas Van Beek100% (2)
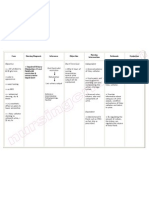
- Nursing Care Plan Impaired Urinary EliminationDocument1 pageNursing Care Plan Impaired Urinary Eliminationderic86% (14)
- Spirometry findings in a 65-year old male with respiratory distressDocument5 pagesSpirometry findings in a 65-year old male with respiratory distressAaron ConstantinoNo ratings yet
- Congestive Heart Failure OutlineDocument4 pagesCongestive Heart Failure OutlineDominique PorterNo ratings yet
- Wear and Tear TheoryDocument2 pagesWear and Tear TheoryAko ManghudNo ratings yet
- Floracopeia Essential Oil EbookDocument61 pagesFloracopeia Essential Oil EbookOana Algasovschi100% (1)
- Benign Ovarian ConditionsDocument31 pagesBenign Ovarian ConditionsNur Hanani KhanNo ratings yet
- Gouty Arthritis: Presented By: Petit Ivy Mae B. NacarioDocument21 pagesGouty Arthritis: Presented By: Petit Ivy Mae B. NacarioMarivic DianoNo ratings yet
- DrowningDocument7 pagesDrowningmedhatsabriNo ratings yet
- NCM106 Module II Cardiac Failure Nursing CareDocument3 pagesNCM106 Module II Cardiac Failure Nursing CareGrant Wynn ArnucoNo ratings yet
- Addison's Disease: Adrenal Insufficiency and Adrenal CrisisDocument15 pagesAddison's Disease: Adrenal Insufficiency and Adrenal CrisisMaryONo ratings yet
- CHN Review March 1 2011 CompleteDocument61 pagesCHN Review March 1 2011 CompletekrezeojNo ratings yet
- Diarrhea and DehydrationDocument12 pagesDiarrhea and DehydrationnikprovNo ratings yet
- PneumoniaDocument8 pagesPneumoniaNader Smadi100% (2)
- A. Cardiac Failure: Biologic CrisisDocument11 pagesA. Cardiac Failure: Biologic CrisisJillian CaumbanNo ratings yet
- Pathophysiology of Copd: Prepared By: Joseph Mari Jess R. EnanoDocument20 pagesPathophysiology of Copd: Prepared By: Joseph Mari Jess R. Enanojoyrena ochondraNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia Gravisdmnd_cdNo ratings yet
- MyocarditisDocument29 pagesMyocarditispanvilai0% (1)
- Medical Surgical: SNS (Anti-Cholinergic/adrenergic)Document12 pagesMedical Surgical: SNS (Anti-Cholinergic/adrenergic)Pedro SorianoNo ratings yet
- Sirs, Shock, Sepsis, ModsDocument8 pagesSirs, Shock, Sepsis, ModsthubtendrolmaNo ratings yet
- 12 NCP Spinal Cord InjuryDocument21 pages12 NCP Spinal Cord InjuryICa MarlinaNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- Hematologic DisordersDocument40 pagesHematologic DisordersMary Grace LeronNo ratings yet
- Amoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Document25 pagesAmoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Abdullah AzeemNo ratings yet
- Pathophysiology of Chronic Renal Failure PDFDocument4 pagesPathophysiology of Chronic Renal Failure PDFDewa Made Rendy SanjayaNo ratings yet
- Hemorrhagic Cerebro Vascular DiseaseDocument37 pagesHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Pathophysiology of ArrhythmiasDocument15 pagesPathophysiology of ArrhythmiasJonathan MontecilloNo ratings yet
- Hypovolemic ShockDocument13 pagesHypovolemic ShockJed ProwellNo ratings yet
- Diabetes Insipidus: Nursing Care PlansDocument6 pagesDiabetes Insipidus: Nursing Care PlansSewyel GarburiNo ratings yet
- ABRUPTIO PLACENTAE PathophysiologyDocument3 pagesABRUPTIO PLACENTAE PathophysiologyBarda GulanNo ratings yet
- Syndrome of Inappropriate Antidiuretic Hormone Secretion - Practice Essentials, Background, PathophysiologyDocument5 pagesSyndrome of Inappropriate Antidiuretic Hormone Secretion - Practice Essentials, Background, PathophysiologyWoro Hapsari WahyuningrumNo ratings yet
- OsteomalaciaDocument23 pagesOsteomalaciaKim Gonzales88% (8)
- Biologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManDocument162 pagesBiologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManLex CatNo ratings yet
- Pathophysiology - Acute Respiratory Distress Syndrome (ARDS)Document1 pagePathophysiology - Acute Respiratory Distress Syndrome (ARDS)Jewel YapNo ratings yet
- Gouty ArthritisDocument8 pagesGouty ArthritisNik2No ratings yet
- Multiple Organ Dysfunction Syndrome (MODS)Document1 pageMultiple Organ Dysfunction Syndrome (MODS)mikErlh50% (2)
- Coronary Heart Disease With AsthmaDocument31 pagesCoronary Heart Disease With AsthmaEf LablaNo ratings yet
- Assessment of Digestive and Gastrointestinal FunctionDocument19 pagesAssessment of Digestive and Gastrointestinal Functioncburnett1No ratings yet
- Compilation of CHN NotesDocument22 pagesCompilation of CHN Notestempter_10100% (1)
- DRUG STUDY: NCM 106 PHARMACOLOGYDocument6 pagesDRUG STUDY: NCM 106 PHARMACOLOGYKevin RosalesNo ratings yet
- Crestor (Rosuvastatin Calcium) : Abbreviations Abbrev Definitions Dictionary ICD9 Codes Equipment Hospitals Drugs More.Document2 pagesCrestor (Rosuvastatin Calcium) : Abbreviations Abbrev Definitions Dictionary ICD9 Codes Equipment Hospitals Drugs More.Aidi RahmanNo ratings yet
- Pulmonary Contusion - WikipediaDocument15 pagesPulmonary Contusion - WikipediaRony OktarizalNo ratings yet
- Brain AbscessDocument5 pagesBrain AbscessEugene Briagas Roque100% (1)
- Types of ShocksDocument33 pagesTypes of Shocksmark OrpillaNo ratings yet
- Chapter 13: Clients With Fluid ImbalancesDocument6 pagesChapter 13: Clients With Fluid ImbalancesTrixie AlvarezNo ratings yet
- Care of Older Adults Concepts and TheoriesDocument13 pagesCare of Older Adults Concepts and TheoriesDaryl Adrian RecaidoNo ratings yet
- Disorders of The EyeDocument16 pagesDisorders of The Eyelisette_sakuraNo ratings yet
- MB451X PSDocument2 pagesMB451X PSMalik AzizNo ratings yet
- Peptic UlcerDocument5 pagesPeptic UlcermerobabuNo ratings yet
- Hyperglycemic Crisis in Acute Care: Purwoko Sugeng HDocument49 pagesHyperglycemic Crisis in Acute Care: Purwoko Sugeng HBee DanielNo ratings yet
- Medical Surgical Nursing Kawasaki DiseaseDocument2 pagesMedical Surgical Nursing Kawasaki DiseaseChieChay DubNo ratings yet
- Nurse Licensure Exam CBQs on Renal and Cardiovascular SystemsDocument2 pagesNurse Licensure Exam CBQs on Renal and Cardiovascular SystemsJhannNo ratings yet
- Psychiatric Nursing (Notes) : Alcohol AbuseDocument88 pagesPsychiatric Nursing (Notes) : Alcohol AbuseJulie Ann ParaNo ratings yet
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Document2 pagesKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaNo ratings yet
- Respiratory FailureDocument15 pagesRespiratory FailureJulien TorresNo ratings yet
- Grand Coaching: Medical Surgical NursingDocument22 pagesGrand Coaching: Medical Surgical NursingEsarpy (Nana)No ratings yet
- Cardiogenic Shock NclexDocument81 pagesCardiogenic Shock NclexKrishna SapkotaNo ratings yet
- Nursing care of Clients in Emergency Situations - 1Document48 pagesNursing care of Clients in Emergency Situations - 1Danica FrancoNo ratings yet
- Alteration in OxygenationDocument8 pagesAlteration in Oxygenationraquel maniegoNo ratings yet
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Respiratory System: Lower Airway Disorders and PneumoniaDocument247 pagesThe Respiratory System: Lower Airway Disorders and PneumoniaKatrina PonceNo ratings yet
- Acute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanDocument54 pagesAcute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanMuhammad Rizki Junaidi SaputraNo ratings yet
- Rundown Kegiatan Pearls Makassar 2021: HARI 1, 23 OKTOBER 2021 WaktuDocument12 pagesRundown Kegiatan Pearls Makassar 2021: HARI 1, 23 OKTOBER 2021 WaktuangelicaNo ratings yet
- Case Study Pneumonia)Document20 pagesCase Study Pneumonia)Jai - Ho83% (6)
- MaternityDocument91 pagesMaternityAnonymous D8KswoNo ratings yet
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument2 pagesDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- Robert Murphy DissertationDocument6 pagesRobert Murphy DissertationPaperWritingCompanyCanada100% (1)
- Nephrostomy Tubes ToolkitDocument18 pagesNephrostomy Tubes Toolkitmegawati.rscmNo ratings yet
- Autoimmune DiseaseDocument3 pagesAutoimmune DiseasePearl AudeNo ratings yet
- Vertebral Augmentation: Panayotis E. Zouboulis, MD, PHDDocument20 pagesVertebral Augmentation: Panayotis E. Zouboulis, MD, PHDneareastspineNo ratings yet
- Gorilla Beringei Ssp. BeringeiDocument25 pagesGorilla Beringei Ssp. BeringeiLaibaNo ratings yet
- Antiinflammatory and Antimicrobial Activity of Hexane Extract of Seed of Psoralea Corylifolia LinnDocument9 pagesAntiinflammatory and Antimicrobial Activity of Hexane Extract of Seed of Psoralea Corylifolia Linnvani srcmNo ratings yet
- Nursing Student Resume GuideDocument16 pagesNursing Student Resume GuideBrainan Aquino100% (2)
- Bab 1 Normal KGBDocument14 pagesBab 1 Normal KGBukhtianitaNo ratings yet
- Microbiome Investigation Notebook, Pages 39-45Document7 pagesMicrobiome Investigation Notebook, Pages 39-45Rick WuNo ratings yet
- One Word Substitutions PDFDocument7 pagesOne Word Substitutions PDFSunil Darisipudi DNo ratings yet
- PATHOPHYSIOLOGYDocument4 pagesPATHOPHYSIOLOGYThea Lacaba AbosamaNo ratings yet
- Foam SclerotherapyDocument30 pagesFoam SclerotherapyRMR100% (1)
- 1.1 Fundamentals of The Nervous SystemDocument18 pages1.1 Fundamentals of The Nervous Systemno nameNo ratings yet
- Evaluation of The Hip: History, Physical Examination, and ImagingDocument11 pagesEvaluation of The Hip: History, Physical Examination, and ImagingmilelytaNo ratings yet
- EmotionsDocument58 pagesEmotionsthivyaashini SellaNo ratings yet
- Rasmussen's EncephalitisDocument25 pagesRasmussen's EncephalitisShellyanaCindyNo ratings yet
- 01 Introduction To Anatomy and PhysiologyDocument38 pages01 Introduction To Anatomy and PhysiologyRahmania PamungkasNo ratings yet
- Sangu ParpamDocument9 pagesSangu ParpamBraveheartt0% (1)
- Research Chapter 1 3Document21 pagesResearch Chapter 1 3anon_53520000100% (1)
- Guía de Práctica Clínica Europea ITUDocument7 pagesGuía de Práctica Clínica Europea ITUVICTORIA GONZALEZ VEGANo ratings yet
- Brachial Plexus Most ImportantDocument2 pagesBrachial Plexus Most ImportantFlowerNo ratings yet
- Controlling Drug Delivery SystemsDocument24 pagesControlling Drug Delivery SystemsYuppie RajNo ratings yet