You might also like
- Anal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read OnlineDocument4 pagesAnal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read Onlinezamin4pak50% (2)
- Basic Life Support CPR and First AidDocument112 pagesBasic Life Support CPR and First AidArthur LimNo ratings yet
- Self HypnosisDocument56 pagesSelf HypnosisMarinNo ratings yet
- The Chest of Hope, Inc.Document2 pagesThe Chest of Hope, Inc.bg giangNo ratings yet
- Sop of SopDocument3 pagesSop of SopGajanan NaikNo ratings yet
- Caregiving Elderly Care TRDocument170 pagesCaregiving Elderly Care TRRodolfo Corpuz67% (3)
- P ECH 23 3102 220649-ReceiptDocument1 pageP ECH 23 3102 220649-ReceiptLe RoiNo ratings yet
- Addison's DiseaseDocument17 pagesAddison's DiseaseMah Jezthy100% (1)
- Ot DischargeDocument2 pagesOt DischargePatrick Mamai SimiyuNo ratings yet
- Requisition For Medical Imaging and Interventional ProceduresDocument2 pagesRequisition For Medical Imaging and Interventional ProceduresokamiotokoNo ratings yet
- WCB Invoice BlankDocument1 pageWCB Invoice BlankJord Van DansenNo ratings yet
- PSYCHNDocument1 pagePSYCHNDawn CasuncadNo ratings yet
- 267 PDF enDocument1 page267 PDF ensanjeetNo ratings yet
- Worker & Plan Details: C921 Home Health Care Services Incident ReportDocument1 pageWorker & Plan Details: C921 Home Health Care Services Incident ReportDawn CasuncadNo ratings yet
- C642 Home Health Care Services Assessment Report: Worker DetailsDocument2 pagesC642 Home Health Care Services Assessment Report: Worker DetailsDawn CasuncadNo ratings yet
- Microbiology Test Request FormDocument4 pagesMicrobiology Test Request FormMegen PLCNo ratings yet
- Form 1Document1 pageForm 1Abdur RasyidNo ratings yet
- C1416 Psychology Services Family Member/Joint Treatment Extension RequestDocument2 pagesC1416 Psychology Services Family Member/Joint Treatment Extension RequestDawn CasuncadNo ratings yet
- C537ADocument1 pageC537ADawn CasuncadNo ratings yet
- Worker & Plan Details: (Claim#) (Surname) (Firstname)Document1 pageWorker & Plan Details: (Claim#) (Surname) (Firstname)Dawn CasuncadNo ratings yet
- CS011Document11 pagesCS011Dean LefebvreNo ratings yet
- C987 Prosthetic and Orthotic Services Prosthetist Request: Microprocessor or Myoelectric Device Worker DetailsDocument2 pagesC987 Prosthetic and Orthotic Services Prosthetist Request: Microprocessor or Myoelectric Device Worker DetailsDawn CasuncadNo ratings yet
- PBCC Seminar Registration FormDocument1 pagePBCC Seminar Registration FormCedrickNo ratings yet
- Neurology Request FormDocument4 pagesNeurology Request FormMegen PLCNo ratings yet
- C988 Prosthetic and Orthotic Services Physician Assessment: Microprocessor or Myoelectric Device Worker DetailsDocument2 pagesC988 Prosthetic and Orthotic Services Physician Assessment: Microprocessor or Myoelectric Device Worker DetailsDawn CasuncadNo ratings yet
- C972 Hearing Loss Services Hearing Loss Authorization: Worker DetailsDocument1 pageC972 Hearing Loss Services Hearing Loss Authorization: Worker DetailsDawn CasuncadNo ratings yet
- C776 Home Health Care Services: Non-Authorized Provider Invoice Cover SheetDocument1 pageC776 Home Health Care Services: Non-Authorized Provider Invoice Cover SheetDawn CasuncadNo ratings yet
- B 0506 BHS1700000003 08Document76 pagesB 0506 BHS1700000003 08vijayNo ratings yet
- New Supplier Set Up and Details Update FormDocument3 pagesNew Supplier Set Up and Details Update FormPenélope FatimaNo ratings yet
- #382383 Update Current Credit Application - L3Document3 pages#382383 Update Current Credit Application - L3radman1420No ratings yet
- WFP, UN Compound at Shelter-21 - Primary ISPDocument14 pagesWFP, UN Compound at Shelter-21 - Primary ISPtestNo ratings yet
- InternationalStudentHealthFee Ish Ish X37003194374 Invoice 2024 01 05Document2 pagesInternationalStudentHealthFee Ish Ish X37003194374 Invoice 2024 01 05manmeetbirring2344No ratings yet
- 1A76D682Document1 page1A76D682Priya PNo ratings yet
- Summary of Current Charges (RS) : Talk To Us SMSDocument7 pagesSummary of Current Charges (RS) : Talk To Us SMSanujshah13No ratings yet
- Canvass 2019 1 LOT Proposed Monthly Periodic Maintenance Service For (1) Unit Elevator, Kone Brand Etc 0243Document1 pageCanvass 2019 1 LOT Proposed Monthly Periodic Maintenance Service For (1) Unit Elevator, Kone Brand Etc 0243Procurement WVMCNo ratings yet
- Amazon Labor Union LMs For 2023Document28 pagesAmazon Labor Union LMs For 2023LaborUnionNews.comNo ratings yet
- Mat2 FormDocument2 pagesMat2 FormTirso Leo Adelante100% (1)
- Supplier Rules: (See Attached Vendor Set Up/ Changes Form)Document3 pagesSupplier Rules: (See Attached Vendor Set Up/ Changes Form)Penélope FatimaNo ratings yet
- Exam Application Form - December 12, 2023Document2 pagesExam Application Form - December 12, 2023lixingyuhhhhhNo ratings yet
- How To Fill in This Dental Claim FormDocument2 pagesHow To Fill in This Dental Claim FormEli RodriguezNo ratings yet
- C1304 Home Health Care Services Monthly Summary: Worker DetailsDocument1 pageC1304 Home Health Care Services Monthly Summary: Worker DetailsDawn CasuncadNo ratings yet
- Customer Information Update: Details of PolicyownerDocument2 pagesCustomer Information Update: Details of PolicyownerHuck NomadNo ratings yet
- E-Receipt For State Bank Collect Payment: Chief Warden DateDocument1 pageE-Receipt For State Bank Collect Payment: Chief Warden Datebhagyashree dNo ratings yet
- 310323I049906813 (1) Payslip PDFDocument1 page310323I049906813 (1) Payslip PDF21octatradingNo ratings yet
- C1170 Occupational Therapy Services Splinting Initial AssessmentDocument2 pagesC1170 Occupational Therapy Services Splinting Initial AssessmentDawn CasuncadNo ratings yet
- Reimbursement Request CUAETDocument1 pageReimbursement Request CUAETqwertNo ratings yet
- RPT Bulk Customer InfoDocument1 pageRPT Bulk Customer InfoHarry JackNo ratings yet
- 058 MEPCO CallDocument1 page058 MEPCO CallCh ShahzadNo ratings yet
- Eastern Maine Me WorkbookDocument16 pagesEastern Maine Me WorkbookNEWS CENTER MaineNo ratings yet
- MAT2Document2 pagesMAT2Kyle Irvin Gole CruzNo ratings yet
- 0724A FeeSchedPhys 2018Document4 pages0724A FeeSchedPhys 2018lknjlkjkNo ratings yet
- Free Medical InvoiceDocument2 pagesFree Medical InvoicetestingidfakeNo ratings yet
- Inter Company Invoicing ProcessDocument1 pageInter Company Invoicing Processaj9055537No ratings yet
- TopTech InvoiceDocument2 pagesTopTech InvoiceSanthosh SanrockNo ratings yet
- El Rey Motel 954533465 454 E Foothill BLVD Rialto, CA 92376 (909) 875-0134 Marvin Lal (909) 875-0134Document20 pagesEl Rey Motel 954533465 454 E Foothill BLVD Rialto, CA 92376 (909) 875-0134 Marvin Lal (909) 875-0134Patel ArvindNo ratings yet
- Sof SKJ2Document2 pagesSof SKJ2YAAKOP BIN HAJI CHELONNo ratings yet
- ModernaDocument508 pagesModernasmtknivesNo ratings yet
- Gastroenterology and Hepatology Test RequestDocument4 pagesGastroenterology and Hepatology Test Requestbassam alharaziNo ratings yet
- New Hanover Community Endowment Applications April 2024Document40 pagesNew Hanover Community Endowment Applications April 2024Ben SchachtmanNo ratings yet
- A 4 Jee Main 1 1Document1 pageA 4 Jee Main 1 1sumit sajwanNo ratings yet
- Healthcare Provider Relation LetterDocument3 pagesHealthcare Provider Relation LetterKewal TareNo ratings yet
- TN Enrollment Document For 87726 Created 6-12-2023 37731414Document2 pagesTN Enrollment Document For 87726 Created 6-12-2023 37731414kalinalveyNo ratings yet
- EST1030970Document2 pagesEST1030970cristian camilo ONo ratings yet
- Kyc Details Change Form For IndividualDocument1 pageKyc Details Change Form For IndividualUttam MehtaNo ratings yet
- For ANSI Use Only:: Service Date: - Noted ByDocument1 pageFor ANSI Use Only:: Service Date: - Noted BySusan Doblada SilvaNo ratings yet
- Below Knee AmputationDocument6 pagesBelow Knee AmputationAmacayoNo ratings yet
- Metodologia de Admitere 2018 - Limba EnglezaDocument27 pagesMetodologia de Admitere 2018 - Limba EnglezaoscarapaNo ratings yet
- CH-2034 Nalco Waters PermaCare Application Improved Productivity of A Reverse Osmosis SystemDocument2 pagesCH-2034 Nalco Waters PermaCare Application Improved Productivity of A Reverse Osmosis SystemLeonardo SimorangkirNo ratings yet
- AnaPhy Skin Cancer Case Study-BASCODocument6 pagesAnaPhy Skin Cancer Case Study-BASCOChristine Jane BascoNo ratings yet
- CID Cheese Mozzarella LiteDocument8 pagesCID Cheese Mozzarella LiteBayu SyurahmadNo ratings yet
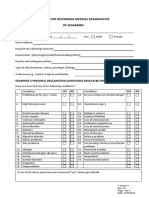
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- Copd VS AsthmaDocument2 pagesCopd VS AsthmaHarkirat AtwalNo ratings yet
- Hostel Rules and RegulationsDocument11 pagesHostel Rules and RegulationsAkshet PatelNo ratings yet
- The Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesDocument8 pagesThe Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesLwsynergylab OfficialNo ratings yet
- Intraoperative CholangiogramDocument3 pagesIntraoperative CholangiogramPauline Jimenea100% (2)
- Effectiveness and Neural Mechanisms of Home-BasedDocument5 pagesEffectiveness and Neural Mechanisms of Home-BasedMuhammad ImronNo ratings yet
- Synerquest 2014 Annual Calendar of DOLE-prescribed CoursesDocument3 pagesSynerquest 2014 Annual Calendar of DOLE-prescribed CoursesrobinrubinaNo ratings yet
- History of Perioperative Nursing 2023Document10 pagesHistory of Perioperative Nursing 2023Boniface MogakaNo ratings yet
- Staphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andDocument8 pagesStaphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andRisna IrvianiNo ratings yet
- The U.S. Virgin Islands Renewable and Alternative Energy Act of 2009Document28 pagesThe U.S. Virgin Islands Renewable and Alternative Energy Act of 2009Detlef LoyNo ratings yet
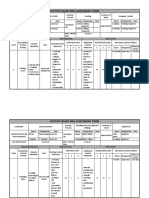
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Department of Pharmaceutical ChemistryDocument13 pagesDepartment of Pharmaceutical ChemistrySuvarna KiniNo ratings yet
- Republic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionDocument8 pagesRepublic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionChristy Ledesma-NavarroNo ratings yet
- Perbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia TenggaraDocument6 pagesPerbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia Tenggarasofia uyNo ratings yet
- ST Bridget's DebriefDocument8 pagesST Bridget's DebriefSri NarendiranNo ratings yet
- Understanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityDocument8 pagesUnderstanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityMutluri AbrahamNo ratings yet
- Ringkasan Promosi CCHC GT, CP & SR Nov 2023Document73 pagesRingkasan Promosi CCHC GT, CP & SR Nov 2023Adnin MonandaNo ratings yet
- TBL PaedsDocument10 pagesTBL PaedsHo Yong WaiNo ratings yet
- DecomposingDocument2 pagesDecomposingapi-254428474100% (1)