You might also like
- How To Split PostingDocument14 pagesHow To Split Postingrajis75100% (1)
- Pdftax Invoice.665985633 PDFDocument14 pagesPdftax Invoice.665985633 PDFTrevNo ratings yet
- Blank Taxi Receipt TemplateDocument4 pagesBlank Taxi Receipt TemplatedigrajNo ratings yet
- Detailed Instructions: Please SelectDocument7 pagesDetailed Instructions: Please Selectflrpatel81No ratings yet
- Simple ReceiptDocument5 pagesSimple Receiptnuri90No ratings yet
- Mushak: 6.3: Tax Invoice Details of Registered PersonDocument2 pagesMushak: 6.3: Tax Invoice Details of Registered PersonAnonymous ZGcs7MwsLNo ratings yet
- SampleDocument11 pagesSampleYanyan RivalNo ratings yet
- C776 Home Health Care Services: Non-Authorized Provider Invoice Cover SheetDocument1 pageC776 Home Health Care Services: Non-Authorized Provider Invoice Cover SheetDawn CasuncadNo ratings yet
- Summary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Document4 pagesSummary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377far03No ratings yet
- Expense Report IIF FileDocument8 pagesExpense Report IIF FileLiz AnNo ratings yet
- Service-Invoice 2Document6 pagesService-Invoice 2Realliance PHNo ratings yet
- Blank InvoiceDocument3 pagesBlank Invoicemelky dominggusNo ratings yet
- Rental Billing StatementDocument7 pagesRental Billing StatementTRACY100% (1)
- Service InvoiceDocument7 pagesService InvoiceRealliance PHNo ratings yet
- 1 Word InvoiceDocument2 pages1 Word InvoicePawPaul MccoyNo ratings yet
- Reliance Communications bill details for Rs. 464.52 due on April 1stDocument6 pagesReliance Communications bill details for Rs. 464.52 due on April 1stManamohan KamatNo ratings yet
- Bill Enquiries: 3033 7777 or 377: Summary of Current Charges Amount (RS)Document4 pagesBill Enquiries: 3033 7777 or 377: Summary of Current Charges Amount (RS)anon-224663No ratings yet
- Simple InvoiceDocument4 pagesSimple InvoiceEdo YahyaNo ratings yet
- Statement: Company NameDocument6 pagesStatement: Company NameBleep NewsNo ratings yet
- Statement: Company NameDocument6 pagesStatement: Company NameRomeo DupaNo ratings yet
- Wa0025.Document3 pagesWa0025.aldarizmafNo ratings yet
- 1 Word-Invoice ProformaDocument2 pages1 Word-Invoice ProformaNaYS- GNo ratings yet
- Fatura Vivo Total_ Fibra + Celular500_10GBDocument1 pageFatura Vivo Total_ Fibra + Celular500_10GBlaerteassis51No ratings yet
- Bina Jaya Enterprise: Resit RasmiDocument5 pagesBina Jaya Enterprise: Resit Rasmiramli zakariaNo ratings yet
- Challan No./ Itns 280: Details of Payments For Use in Receiving BankDocument3 pagesChallan No./ Itns 280: Details of Payments For Use in Receiving BankSatish BatchaNo ratings yet
- Summary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Document6 pagesSummary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377chandra_nadikudiNo ratings yet
- Document Checklist: Joint Venture / Sole-Proprietor / Unincorporated BodyDocument20 pagesDocument Checklist: Joint Venture / Sole-Proprietor / Unincorporated BodyEDWARD LEENo ratings yet
- Account StatementDocument9 pagesAccount StatementAzwarNo ratings yet
- LT BILL 37056257097 Dec23Document2 pagesLT BILL 37056257097 Dec23rik chattopadhyayNo ratings yet
- Accounting For Vat: The BahamasDocument24 pagesAccounting For Vat: The Bahamasrazi12129094No ratings yet
- Expense Report TemplateDocument6 pagesExpense Report TemplateLiz AnNo ratings yet
- FD ExistingDocument2 pagesFD Existingmisra.srbh11No ratings yet
- Simple ReceiptDocument4 pagesSimple ReceiptLouis KohNo ratings yet
- ChallanFormDocument1 pageChallanFormmanpreet singhNo ratings yet
- Certificate of Creditable Tax Withheld at Source: (MM/DD/YYYY) (MM/DD/YYYY)Document3 pagesCertificate of Creditable Tax Withheld at Source: (MM/DD/YYYY) (MM/DD/YYYY)RodelLaborNo ratings yet
- Fowlis, Jesse - T183Document2 pagesFowlis, Jesse - T183End UserNo ratings yet
- DREMC-Application-for-Service-2022-fillable 2Document2 pagesDREMC-Application-for-Service-2022-fillable 2vtcwrxdf26No ratings yet
- ChallanFormDocument1 pageChallanFormmanpreet singhNo ratings yet
- Abc Elementary School: Purchase OrderDocument16 pagesAbc Elementary School: Purchase OrderRexell MaybuenaNo ratings yet
- Summary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Document6 pagesSummary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377meedinesh123No ratings yet
- Account StatementDocument11 pagesAccount Statementsouth adventureNo ratings yet
- ChallanFormDocument1 pageChallanFormmanpreet singhNo ratings yet
- Challan No. ITNS 280Document2 pagesChallan No. ITNS 280RAHUL AGARWALNo ratings yet
- R.A. Bill No.Document304 pagesR.A. Bill No.Yash DeoreNo ratings yet
- HVAC Incentive AppDocument2 pagesHVAC Incentive AppsandyolkowskiNo ratings yet
- Account Temporary ReceiptDocument5 pagesAccount Temporary ReceiptPD888No ratings yet
- D D MM Y Y Yy: (Separate Forms Need To Be Filled For Each Tax Type)Document3 pagesD D MM Y Y Yy: (Separate Forms Need To Be Filled For Each Tax Type)nikhil kumarNo ratings yet
- Income Tax - Computation - 2021Document26 pagesIncome Tax - Computation - 2021umasankarNo ratings yet
- CS011Document11 pagesCS011Dean LefebvreNo ratings yet
- Summary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Document6 pagesSummary of Current Charges Amount (RS.) : Bill Enquiries: 3033 7777 or 377Deepak ThakurNo ratings yet
- C1304 Home Health Care Services Monthly Summary: Worker DetailsDocument1 pageC1304 Home Health Care Services Monthly Summary: Worker DetailsDawn CasuncadNo ratings yet
- Request For Quotation: Not RequiredDocument3 pagesRequest For Quotation: Not RequiredChirag DaveNo ratings yet
- Challan No./ ITNS 282: Tax Applicable (Tick One)Document2 pagesChallan No./ ITNS 282: Tax Applicable (Tick One)satishkumar.mandora.smNo ratings yet
- How To Reconcile and Pay Your Aflac InvoiceDocument21 pagesHow To Reconcile and Pay Your Aflac InvoiceLaurie RandleNo ratings yet
- Mosegeri Engineering and Construction Co. Limited November Vat ReturnDocument1 pageMosegeri Engineering and Construction Co. Limited November Vat Returnmburumoses240No ratings yet
- MPPL It 2019 - 1Document3 pagesMPPL It 2019 - 1Fareed KhanNo ratings yet
- Your Reliance Bill: Summary of Current Charges Amount (RS)Document3 pagesYour Reliance Bill: Summary of Current Charges Amount (RS)shimmmNo ratings yet
- GST Icai 15072023Document98 pagesGST Icai 15072023Selvakumar MuthurajNo ratings yet
- Bill of Supply For Electricity: Due Date: 24-03-2018Document2 pagesBill of Supply For Electricity: Due Date: 24-03-2018gurdeeNo ratings yet
- Georgia State Board of Workers' Compensation: EmployeeDocument1 pageGeorgia State Board of Workers' Compensation: EmployeejeffdandelNo ratings yet
- Economic & Budget Forecast Workbook: Economic workbook with worksheetFrom EverandEconomic & Budget Forecast Workbook: Economic workbook with worksheetNo ratings yet
- Goods and Services Tax (GST) Filing Made Easy: Free Software Literacy SeriesFrom EverandGoods and Services Tax (GST) Filing Made Easy: Free Software Literacy SeriesNo ratings yet
- Worker Details: C1265 Hearing Loss Services Hearing Aid Replacement InformationDocument2 pagesWorker Details: C1265 Hearing Loss Services Hearing Aid Replacement InformationDawn CasuncadNo ratings yet
- HC965Document1 pageHC965Dawn CasuncadNo ratings yet
- (Claim#) (Surname) (Firstname) : C1392 Psychology Services Mental Health First ReportDocument4 pages(Claim#) (Surname) (Firstname) : C1392 Psychology Services Mental Health First ReportDawn CasuncadNo ratings yet
- (Claim#) (Surname) (Firstname) : C852 Psychology Services Counselling Progress ReportDocument4 pages(Claim#) (Surname) (Firstname) : C852 Psychology Services Counselling Progress ReportDawn CasuncadNo ratings yet
- (Claim#) (Surname) (Firstname) : C1392 Psychology Services Mental Health First ReportDocument4 pages(Claim#) (Surname) (Firstname) : C1392 Psychology Services Mental Health First ReportDawn CasuncadNo ratings yet
- Occupational Therapy Services: Worker DetailsDocument3 pagesOccupational Therapy Services: Worker DetailsDawn CasuncadNo ratings yet
- C1388 Psychology Services MSW Counselling Services Invoice: Worker DetailsDocument2 pagesC1388 Psychology Services MSW Counselling Services Invoice: Worker DetailsDawn CasuncadNo ratings yet
- PSYCHNDocument1 pagePSYCHNDawn CasuncadNo ratings yet
- HC428Document1 pageHC428Dawn CasuncadNo ratings yet
- HC397Document5 pagesHC397Dawn CasuncadNo ratings yet
- C642 Home Health Care Services Assessment Report: Worker DetailsDocument2 pagesC642 Home Health Care Services Assessment Report: Worker DetailsDawn CasuncadNo ratings yet
- Become AcupDocument1 pageBecome AcupDawn CasuncadNo ratings yet
- C728 Home Health Care Services Homemaking PlanDocument3 pagesC728 Home Health Care Services Homemaking PlanDawn CasuncadNo ratings yet
- Occupational Therapy Services: (Claim#) (Surname) (Firstname)Document10 pagesOccupational Therapy Services: (Claim#) (Surname) (Firstname)Dawn CasuncadNo ratings yet
- Worker & Plan Details: C729 Home Health Care Services Personal Care PlanDocument5 pagesWorker & Plan Details: C729 Home Health Care Services Personal Care PlanDawn CasuncadNo ratings yet
- Worker & Plan Details: C921 Home Health Care Services Incident ReportDocument1 pageWorker & Plan Details: C921 Home Health Care Services Incident ReportDawn CasuncadNo ratings yet
- Psych Treat ConsentDocument1 pagePsych Treat ConsentDawn CasuncadNo ratings yet
- HC774Document4 pagesHC774Dawn CasuncadNo ratings yet
- C1162 Occupational Therapy Services Ergonomic Assessment: Worker DetailsDocument3 pagesC1162 Occupational Therapy Services Ergonomic Assessment: Worker DetailsDawn CasuncadNo ratings yet
- C1169 Occupational Therapy Services Hand Therapy Discharge ReportDocument2 pagesC1169 Occupational Therapy Services Hand Therapy Discharge ReportDawn CasuncadNo ratings yet
- HC777Document3 pagesHC777Dawn CasuncadNo ratings yet
- HC404Document4 pagesHC404Dawn CasuncadNo ratings yet
- C1167 Occupational Therapy Services Hand Therapy Initial AssessmentDocument2 pagesC1167 Occupational Therapy Services Hand Therapy Initial AssessmentDawn CasuncadNo ratings yet
- C1260 Occupational Therapy Services General Assessment: (Claim#) (Surname) (Firstname)Document3 pagesC1260 Occupational Therapy Services General Assessment: (Claim#) (Surname) (Firstname)Dawn CasuncadNo ratings yet
- Occupational Therapy Services: Worker DetailsDocument5 pagesOccupational Therapy Services: Worker DetailsDawn CasuncadNo ratings yet
- Occupational Therapy Services: Worker DetailsDocument3 pagesOccupational Therapy Services: Worker DetailsDawn CasuncadNo ratings yet
- HC781Document3 pagesHC781Dawn CasuncadNo ratings yet
- HC172Document6 pagesHC172Dawn CasuncadNo ratings yet
- HC825Document6 pagesHC825Dawn CasuncadNo ratings yet
- Oracle Procurement Cloud 2016 Implementation Essentials Q & ADocument17 pagesOracle Procurement Cloud 2016 Implementation Essentials Q & AC NuNo ratings yet
- MCQ of GSTDocument23 pagesMCQ of GSTOnline tally guide100% (2)
- Smart Pay Appllication FormDocument2 pagesSmart Pay Appllication FormTony M.TomyNo ratings yet
- Jan 15Document9 pagesJan 15Alankar GuptaNo ratings yet
- Saravanan Ramaraj ResumeDocument2 pagesSaravanan Ramaraj Resumeanon_469443760No ratings yet
- Spain_SubmitListsForFilesCreatedInExternalSystems_SAPERP_2020JuneDocument16 pagesSpain_SubmitListsForFilesCreatedInExternalSystems_SAPERP_2020JuneDíazNo ratings yet
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Document1 pageTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)R.S.No ratings yet
- SuiteAcademy - Accounting Module 3Document17 pagesSuiteAcademy - Accounting Module 3Chan Yi LinNo ratings yet
- Technical Perspective On Accounts Receivable Receipts PDFDocument15 pagesTechnical Perspective On Accounts Receivable Receipts PDFvenuvydhyalaNo ratings yet
- Marketing Information Systems and The Sales Order ProcessDocument32 pagesMarketing Information Systems and The Sales Order ProcessTejas KeswaniNo ratings yet
- Topic 6 - Bank ReconciliationRev (Students)Document32 pagesTopic 6 - Bank ReconciliationRev (Students)Novian Dwi RamadanaNo ratings yet
- Oracle Apex ERP GUIDE DocumentDocument148 pagesOracle Apex ERP GUIDE DocumentMuhammad WaqasNo ratings yet
- Archit BBP FI V1.0 30092010Document189 pagesArchit BBP FI V1.0 30092010Subhash ReddyNo ratings yet
- PA TablesDocument85 pagesPA Tablescvnagesh0% (1)
- Enhancement For US Tax Calulation FunctionsDocument3 pagesEnhancement For US Tax Calulation Functionsraj gNo ratings yet
- FE Manual SBPDocument24 pagesFE Manual SBPSaad MasoodNo ratings yet
- FY08 Car Lease Document V2Document3 pagesFY08 Car Lease Document V2Swanidhi SinghNo ratings yet
- The Special GL Indicator Sap HanaDocument8 pagesThe Special GL Indicator Sap HanaFormateur Sap SageNo ratings yet
- GSTDocument6 pagesGSTKarthick Raj100% (1)
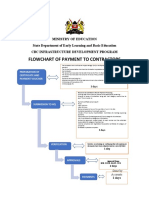
- Process of Payment To ContractorsDocument1 pageProcess of Payment To ContractorsBasil MalakiNo ratings yet
- Finance InductionDocument14 pagesFinance Inductionyayang indahNo ratings yet
- Hotel BillDocument1 pageHotel BillClear ID Supplier100% (1)
- Tender Document For Purchase Of: Safety Items Tender Number: 6000012593/SAFETYITEMS/463/, Dated: 03.06.2019Document37 pagesTender Document For Purchase Of: Safety Items Tender Number: 6000012593/SAFETYITEMS/463/, Dated: 03.06.2019Ganda PrajaNo ratings yet
- Concept of ERS in SAP MMDocument9 pagesConcept of ERS in SAP MMAristeu CunhaNo ratings yet
- Setup OMDocument170 pagesSetup OMBabush LPNo ratings yet
- INCOME TAX AND GST. JURAZ-Module 4Document8 pagesINCOME TAX AND GST. JURAZ-Module 4TERZO IncNo ratings yet
- Oracle: Oracle Inventory Cloud 2020 Implementation EssentialsDocument36 pagesOracle: Oracle Inventory Cloud 2020 Implementation EssentialsManish NayakNo ratings yet