You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Reference Manual: Alcolyzer Plus BeerDocument129 pagesReference Manual: Alcolyzer Plus BeerPhuong Nguyen100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Central Nervous System Tuberculosis: John M. LeonardDocument10 pagesCentral Nervous System Tuberculosis: John M. LeonardMarcela Catalina Fandiño VargasNo ratings yet
- Display PDFDocument8 pagesDisplay PDFSri BalajiNo ratings yet
- Speciality FibresDocument38 pagesSpeciality Fibresnitishkohli100% (6)
- Module 2 SolutionDocument2 pagesModule 2 SolutionLJ Valdez100% (1)
- Swim School Brochure For WebDocument2 pagesSwim School Brochure For WebSudhakar GanjikuntaNo ratings yet
- LM2907 and LM2917 Frequency To Voltage Converter: 1 Features 3 DescriptionDocument42 pagesLM2907 and LM2917 Frequency To Voltage Converter: 1 Features 3 Descriptioncontrol tejidoNo ratings yet
- Section 5 Mechanical Standards Tema Class R C B: StyleDocument195 pagesSection 5 Mechanical Standards Tema Class R C B: StyleASI.KHMEDNo ratings yet
- Foreign Bodies of Air Passages and Food PassageDocument20 pagesForeign Bodies of Air Passages and Food PassageRamli HassanNo ratings yet
- Phaseo ABL7 - ABL8 - ABL7RP4803Document8 pagesPhaseo ABL7 - ABL8 - ABL7RP4803hicham boutoucheNo ratings yet
- Wall Final CalcsDocument9 pagesWall Final CalcsCele Adu-wusuNo ratings yet
- Bajaj Led Lum Price List DT 06 Dec 2016Document62 pagesBajaj Led Lum Price List DT 06 Dec 2016Ujjwal ModiNo ratings yet
- Heat Moisture Pressure Shape Mold Crease The Geometric Forms Smooth Perfect Form During or Final Finishing ProcessDocument29 pagesHeat Moisture Pressure Shape Mold Crease The Geometric Forms Smooth Perfect Form During or Final Finishing Processaqsa imranNo ratings yet
- Semana 5 InglesDocument31 pagesSemana 5 Inglescarlos cajaNo ratings yet
- Announcement 01 Oct PDFDocument2 pagesAnnouncement 01 Oct PDFgaurav chauhanNo ratings yet
- Nightingales Environmental Theory 2Document21 pagesNightingales Environmental Theory 2samanthanicolemercadoNo ratings yet
- Pocket-Guide-To-Fire-Detection-And-Fire-Alarm-Systems-For-Buildings BS 5839-1 - 2017Document24 pagesPocket-Guide-To-Fire-Detection-And-Fire-Alarm-Systems-For-Buildings BS 5839-1 - 2017Robert VillavicencioNo ratings yet
- Uvtron DriverDocument2 pagesUvtron DriverwizdevNo ratings yet
- Cover SDRRMDocument20 pagesCover SDRRMTon LunaNo ratings yet
- PROFITABILITY ANALYSIS at ASIAN PAINTSDocument62 pagesPROFITABILITY ANALYSIS at ASIAN PAINTSRajesh BathulaNo ratings yet
- Breastfeeding TechniqueDocument2 pagesBreastfeeding TechniqueKaye Niale BaleteNo ratings yet
- Presentation Microbial Connections Antibiotic ResistanceDocument21 pagesPresentation Microbial Connections Antibiotic Resistancesushantk862No ratings yet
- Synopsis On Child PsychologyDocument3 pagesSynopsis On Child PsychologyVaishnavi Kulkarni100% (1)
- Teaching Faculty For Allied Health Sciences - 2021Document9 pagesTeaching Faculty For Allied Health Sciences - 2021jamoonNo ratings yet
- The New BMW I3 LCI BMW I3s SpecificationsDocument8 pagesThe New BMW I3 LCI BMW I3s SpecificationsPetre DumitrescuNo ratings yet
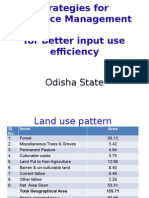
- OdishaDocument36 pagesOdishanirvana.7No ratings yet
- Overflow With Hope - Joel OsteenDocument7 pagesOverflow With Hope - Joel OsteenJHON RAY OTAÑESNo ratings yet
- DZ Value DonutDocument7 pagesDZ Value DonutAmira RosliNo ratings yet
- Dabat Water Supply Design ReportDocument70 pagesDabat Water Supply Design ReportNaaf67% (3)