You might also like
- Healthy Shoulder Handbook: Second Edition: 100 Exercises for Treating Common Injuries and Ending Chronic PainFrom EverandHealthy Shoulder Handbook: Second Edition: 100 Exercises for Treating Common Injuries and Ending Chronic PainNo ratings yet
- Frozen Shoulder: Information For YouDocument8 pagesFrozen Shoulder: Information For YouCentaur Archer100% (1)
- Frozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSDocument6 pagesFrozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSpempekplgNo ratings yet
- Cure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainFrom EverandCure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainNo ratings yet
- Leave Muscle and Back PainDocument12 pagesLeave Muscle and Back PainBackpainGone050% (2)
- Clavicle Fracture Protocol Non SurgicalDocument17 pagesClavicle Fracture Protocol Non SurgicalAlbert MarcuNo ratings yet
- Typical Shoulder TroublesDocument7 pagesTypical Shoulder TroublesLev KalikaNo ratings yet
- Jurnal Tennis ElbowDocument5 pagesJurnal Tennis ElbowMuhamad Fahrizal RilahiNo ratings yet
- Inversiontherapy PDFDocument29 pagesInversiontherapy PDFVizu VizuNo ratings yet
- Mock 2Document40 pagesMock 2Syali Sasidharan100% (2)
- Lumbar Disk HerniationDocument6 pagesLumbar Disk HerniationShivaji DeshmukhNo ratings yet
- Knee Knee Collateral LigamentsDocument8 pagesKnee Knee Collateral LigamentsekaNo ratings yet
- Tennis elbow treatment optionsDocument10 pagesTennis elbow treatment optionsMarliani AfriastutiNo ratings yet
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDocument7 pagesRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNo ratings yet
- Shoulder Arthroscopy Patient Education Packet RayappaDocument5 pagesShoulder Arthroscopy Patient Education Packet Rayappaapi-549337910No ratings yet
- Musculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324Document8 pagesMusculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324JJKNo ratings yet
- Tendonitis of The Long Head of The Biceps-Orthoinfo - AaosDocument5 pagesTendonitis of The Long Head of The Biceps-Orthoinfo - Aaosapi-228773845100% (1)
- Adhesive Capsulitis or Frozen SholderDocument24 pagesAdhesive Capsulitis or Frozen Sholdersanalcrazy100% (1)
- Slap Tears-Orthoinfo - AaosDocument6 pagesSlap Tears-Orthoinfo - Aaosapi-228773845No ratings yet
- Shoulder Injuries in Baseball PlayersDocument7 pagesShoulder Injuries in Baseball PlayersMahayu Firsty RamadhaniNo ratings yet
- Frozen Shoulder (Revision)Document6 pagesFrozen Shoulder (Revision)Atet KurniadiNo ratings yet
- Aaos 2013Document152 pagesAaos 2013Yusufa ArdyNo ratings yet
- Soal UAS Bahasa Inggris Kelas 4 SD Semester 1Document8 pagesSoal UAS Bahasa Inggris Kelas 4 SD Semester 1amal sehat100% (1)
- FootDocument59 pagesFootAnmar Hamid Abd AlmageedNo ratings yet
- Rotator Cuff Repair EbookDocument31 pagesRotator Cuff Repair EbookJohnPaulBascoNo ratings yet
- Shoulder Injury Brachial Plexus InjuryDocument9 pagesShoulder Injury Brachial Plexus InjuryAtet KurniadiNo ratings yet
- Lateral Epicondylitis (Tennis Elbow)Document8 pagesLateral Epicondylitis (Tennis Elbow)Rusu AdrianNo ratings yet
- Campbell's Operative Orthopaedics 11th Edition Canale & Beaty SEO-Optimized TitleDocument5 pagesCampbell's Operative Orthopaedics 11th Edition Canale & Beaty SEO-Optimized TitleShazada Khan50% (4)
- Soal UAS Bahasa Inggris Kelas 3 SD Semester 1Document9 pagesSoal UAS Bahasa Inggris Kelas 3 SD Semester 1amal sehat100% (1)
- What You Should Know About Shoulder InstabilityDocument4 pagesWhat You Should Know About Shoulder InstabilityWoo Guan Lee100% (1)
- Frozen ShoulderDocument6 pagesFrozen ShoulderanumolNo ratings yet
- Frozen Shoulder (Adhesive Capsulitis)Document7 pagesFrozen Shoulder (Adhesive Capsulitis)Rully Riyan DikaNo ratings yet
- Why Is My Shoulder Painful?Document2 pagesWhy Is My Shoulder Painful?Michael CodsiNo ratings yet
- Frozen Shoulder GuideDocument8 pagesFrozen Shoulder GuidefriskaNo ratings yet
- Total Shoulder ReplacementDocument11 pagesTotal Shoulder ReplacementNeicu VladNo ratings yet
- Shoulder Pain and Common Shoulder ProblemsDocument14 pagesShoulder Pain and Common Shoulder ProblemsRatnaPrasadNalamNo ratings yet
- Rotator Cuff Tears - Symptoms, Causes, Diagnosis and TreatmentDocument19 pagesRotator Cuff Tears - Symptoms, Causes, Diagnosis and TreatmentsafiraNo ratings yet
- Long Thoracic Nerve PalsyDocument2 pagesLong Thoracic Nerve PalsyJose Luis Tabueña OrtegaNo ratings yet
- Best Physical Therapy Methods For Treating Shoulder Pain & InjuriesDocument1 pageBest Physical Therapy Methods For Treating Shoulder Pain & Injuriesaidoojeffery260No ratings yet
- Lumbar DiscectomyDocument4 pagesLumbar Discectomyapi-549337910No ratings yet
- Fikri Zulfikar Najat - Ilmu Keolahragaan - Report TextDocument4 pagesFikri Zulfikar Najat - Ilmu Keolahragaan - Report TextFikri Zulfikar NajatNo ratings yet
- Shoulderpain 1Document3 pagesShoulderpain 1Fadlan KhuzaifaNo ratings yet
- Impingement of The Shoulder: DescriptionDocument4 pagesImpingement of The Shoulder: DescriptionRicardo Santi Jr.No ratings yet
- Rehabilitation Exercises For Frozen ShoulderDocument5 pagesRehabilitation Exercises For Frozen ShoulderRajorshi MishraNo ratings yet
- Subacromial Decompression Protocol: Anatomy and BiomechanicsDocument8 pagesSubacromial Decompression Protocol: Anatomy and BiomechanicsIoana PiticarNo ratings yet
- Acromioclavicular Joint Injuries and Physical Therapy ManagementDocument12 pagesAcromioclavicular Joint Injuries and Physical Therapy ManagementSereinNo ratings yet
- Frozen ShoulderDocument4 pagesFrozen ShoulderFirza OktavianiNo ratings yet
- Shoulder Replacement Book: Your Guide to RecoveryDocument8 pagesShoulder Replacement Book: Your Guide to RecoveryRammah EmadNo ratings yet
- Intersection SyndromeDocument5 pagesIntersection SyndromepitkerenNo ratings yet
- Subacromial Bursitis PatientsDocument7 pagesSubacromial Bursitis PatientsSiti WulandariNo ratings yet
- Frozen ShoulderDocument16 pagesFrozen ShoulderRatnaPrasadNalamNo ratings yet
- Rotator Cuff Tear Exercises - Resurgens OrthopaedicsDocument1 pageRotator Cuff Tear Exercises - Resurgens OrthopaedicsaztillaerkNo ratings yet
- Englsih Multimodal EssayDocument6 pagesEnglsih Multimodal Essayapi-667816610No ratings yet
- MSK Shoulder Workbook Final DraftDocument36 pagesMSK Shoulder Workbook Final DraftTrailers MCNo ratings yet
- Bristow Latarjet ProcedureDocument7 pagesBristow Latarjet ProcedurebigwhaledorkNo ratings yet
- SnappinghipsyndromeDocument3 pagesSnappinghipsyndromeapi-275934094No ratings yet
- Techniques 05Document15 pagesTechniques 05saleem razaNo ratings yet
- Total Hip Arthroplasty (THA) Rehabilitation ProtocolDocument11 pagesTotal Hip Arthroplasty (THA) Rehabilitation ProtocoldvenumohanNo ratings yet
- Total Hip Arthroplasty (THA) Rehabilitation ProtocolDocument11 pagesTotal Hip Arthroplasty (THA) Rehabilitation ProtocolSherly L WaromiNo ratings yet
- Frozen ShoulderDocument110 pagesFrozen ShoulderAchmad ZulfikarNo ratings yet
- Muscle-related neck pain reliefDocument8 pagesMuscle-related neck pain reliefvipra ayurvedaNo ratings yet
- North American Spine Society Public Education SeriesDocument12 pagesNorth American Spine Society Public Education SeriesVanitha Ratha KrishnanNo ratings yet
- Cubital Tunnel Syndrome GuideDocument7 pagesCubital Tunnel Syndrome GuideoracleappshrmsNo ratings yet
- Shoulder Protocol Bankart Information: How The Shoulder WorksDocument4 pagesShoulder Protocol Bankart Information: How The Shoulder WorksKartick PaiNo ratings yet
- The Frozen ShoulderDocument27 pagesThe Frozen Shoulderleenadevi90No ratings yet
- Tennis Elbow (Lateral Epicondylitis) - OrthoInfo - AAOSDocument8 pagesTennis Elbow (Lateral Epicondylitis) - OrthoInfo - AAOSnoony 98No ratings yet
- 1Document1 page1amal sehatNo ratings yet
- Jadwal Opr 2012Document30 pagesJadwal Opr 2012amal sehatNo ratings yet
- Cara Instal ProgramDocument1 pageCara Instal Programamal sehatNo ratings yet
- Jadwal Poliklinik RS Islam Amal Sehat SragenDocument2 pagesJadwal Poliklinik RS Islam Amal Sehat Sragenamal sehatNo ratings yet
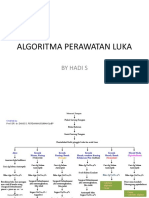
- Algoritma Perawatan Luka by Hadi SetiarjoDocument2 pagesAlgoritma Perawatan Luka by Hadi Setiarjoamal sehatNo ratings yet
- Asuhan Keperawatan Ulcus Diabetic by Aries Asmorohadi, S.kep, NS, M.kep, SP KMB (Etn)Document32 pagesAsuhan Keperawatan Ulcus Diabetic by Aries Asmorohadi, S.kep, NS, M.kep, SP KMB (Etn)amal sehatNo ratings yet
- BFFDocument1 pageBFFamal sehatNo ratings yet
- Acl InjuryDocument8 pagesAcl InjuryFransiscaChelseaNatalieNo ratings yet
- BOS Basic Arthroscopy Course ProgrammeDocument4 pagesBOS Basic Arthroscopy Course ProgrammePankaj VatsaNo ratings yet
- A Review On Frozen Shoulder: Singapore Medical Journal September 2010Document5 pagesA Review On Frozen Shoulder: Singapore Medical Journal September 2010Anonymous ckZmIgoNo ratings yet
- Petitioners vs. vs. Respondent.: Third DivisionDocument7 pagesPetitioners vs. vs. Respondent.: Third DivisionAmicah Frances AntonioNo ratings yet
- Jurnal Reading DR Tomy SpOTDocument10 pagesJurnal Reading DR Tomy SpOTAlfina MeidinaNo ratings yet
- Poly-Traumatic Multi-Ligament Knee Injuries: Is The Knee The Limiting Factor?Document7 pagesPoly-Traumatic Multi-Ligament Knee Injuries: Is The Knee The Limiting Factor?Luigi Paolo Zapata DelgadoNo ratings yet
- Allograft Vs Autograft 2022Document11 pagesAllograft Vs Autograft 2022Ahmed MortadaNo ratings yet
- Return To Sport After Surgical Management of Posterior Shoulder InstabilityDocument13 pagesReturn To Sport After Surgical Management of Posterior Shoulder InstabilityAziz CupinNo ratings yet
- Care PlanDocument11 pagesCare PlanCathy GewontNo ratings yet
- CANINE-Canine Elbow Joint Arthroscopy-Introduction and Descriptin of TechniqueDocument8 pagesCANINE-Canine Elbow Joint Arthroscopy-Introduction and Descriptin of Techniquetaner_soysurenNo ratings yet
- Dimitroulis 2013Document5 pagesDimitroulis 2013priscilavitalfialhoNo ratings yet
- Mohammad ZahidDocument15 pagesMohammad ZahidNazeer AhmadNo ratings yet
- 8 Ankle SprainDocument11 pages8 Ankle Sprainapi-241264935No ratings yet
- 2013 Product GuideDocument149 pages2013 Product GuideTatae UesuNo ratings yet
- TransAmerica Accident AdvanceDocument9 pagesTransAmerica Accident AdvancepreparebenefitsNo ratings yet
- D2 Arthroscopy JournalDocument2 pagesD2 Arthroscopy JournalMartín ZamoraNo ratings yet
- The Anterior Cruciate Ligament: Reconstruction and Basic ScienceDocument6 pagesThe Anterior Cruciate Ligament: Reconstruction and Basic ScienceMourad BennaniNo ratings yet
- Shoulder DislocationDocument7 pagesShoulder Dislocationamal.fathullahNo ratings yet
- Dhawan 2016Document12 pagesDhawan 2016febyan yohanesNo ratings yet
- Comparison of Clinic-And Home-Based Rehabilitation Programs After Total Knee ArthroplastyDocument10 pagesComparison of Clinic-And Home-Based Rehabilitation Programs After Total Knee ArthroplastyKaribeños San JavierNo ratings yet
- DR Clement JosephDocument3 pagesDR Clement JosephShivansh PandeyNo ratings yet
- Arthroscopic Bankart RepairDocument14 pagesArthroscopic Bankart RepairDavid Paul RajNo ratings yet
- What Is A Torn MeniscusDocument6 pagesWhat Is A Torn MeniscusDinesh GodhaniNo ratings yet
- Knee Injury and Osteoarthritis Outcome Score Koos: A User's Guide ToDocument9 pagesKnee Injury and Osteoarthritis Outcome Score Koos: A User's Guide ToQina Nugroho, pts.No ratings yet
- Temporomandibular Joint Surgery for Internal DerangementDocument14 pagesTemporomandibular Joint Surgery for Internal DerangementMatheus MoraisNo ratings yet