You might also like
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointFrom EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointNo ratings yet
- Total Shoulder ReplacementDocument11 pagesTotal Shoulder ReplacementNeicu VladNo ratings yet
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.From EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.No ratings yet
- Knee Arthroscopy Meniscectomy Recovery GuideDocument9 pagesKnee Arthroscopy Meniscectomy Recovery Guidebayan salahNo ratings yet
- Resistance Band Workouts for Bad Posture and Back PainFrom EverandResistance Band Workouts for Bad Posture and Back PainRating: 3.5 out of 5 stars3.5/5 (4)
- National Hospital (Shoulder-Arthroplasty Rehab-Protocol)Document14 pagesNational Hospital (Shoulder-Arthroplasty Rehab-Protocol)muhammad umarNo ratings yet
- Total Hip Arthroplasty (THA) Rehabilitation ProtocolDocument11 pagesTotal Hip Arthroplasty (THA) Rehabilitation ProtocoldvenumohanNo ratings yet
- Total Hip Arthroplasty (THA) Rehabilitation ProtocolDocument11 pagesTotal Hip Arthroplasty (THA) Rehabilitation ProtocolSherly L WaromiNo ratings yet
- Ortho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalDocument17 pagesOrtho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalKattamedhi Krishnachaitanya KumarreddyNo ratings yet
- Frozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSDocument6 pagesFrozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSpempekplgNo ratings yet
- Bristow Latarjet ProcedureDocument7 pagesBristow Latarjet ProcedurebigwhaledorkNo ratings yet
- Clavicle Fracture Protocol Non SurgicalDocument17 pagesClavicle Fracture Protocol Non SurgicalAlbert MarcuNo ratings yet
- A Patient's Guide To Adhesive CapsulitisDocument6 pagesA Patient's Guide To Adhesive Capsulitisamal sehat100% (1)
- Frozen ShoulderDocument6 pagesFrozen ShoulderanumolNo ratings yet
- Reverse Total Shoulder Arthroplasty Rehab ProtocolDocument12 pagesReverse Total Shoulder Arthroplasty Rehab Protocol張水蛙No ratings yet
- Rotator Cuff Impingement/Tendinopathy Rehab GuideDocument8 pagesRotator Cuff Impingement/Tendinopathy Rehab GuidemadaleenNo ratings yet
- TKR PDFDocument6 pagesTKR PDFKaribeños San JavierNo ratings yet
- Treatment: Home TreatmentsDocument3 pagesTreatment: Home TreatmentsDhimas Reyhan Putra SayudhaNo ratings yet
- Achilles Tendon Rupture 0Document15 pagesAchilles Tendon Rupture 0Usman JabbarNo ratings yet
- Total Shoulder Arthroplasty Tsa 2Document15 pagesTotal Shoulder Arthroplasty Tsa 2api-550365743No ratings yet
- ACL Non-Operative ManagmentDocument10 pagesACL Non-Operative ManagmentHammad -ullahNo ratings yet
- Information For Patients Following Knee Arthroscopy: Therapies DirectorateDocument6 pagesInformation For Patients Following Knee Arthroscopy: Therapies Directoratepecson1No ratings yet
- Arthroscopic Bankart Repair1Document14 pagesArthroscopic Bankart Repair1Rinkle KateNo ratings yet
- Post SPINAL - FUSION GuidelinesDocument7 pagesPost SPINAL - FUSION GuidelineskapilphysioNo ratings yet
- TKA Rehab Guide for Fast RecoveryDocument11 pagesTKA Rehab Guide for Fast RecoveryCamille DelageNo ratings yet
- Physiotherapy Goals and Techniques for Burn PatientsDocument15 pagesPhysiotherapy Goals and Techniques for Burn PatientsPraneetha NouduriNo ratings yet
- Signs and TestsDocument4 pagesSigns and TestsKathryn RedNo ratings yet
- Acl Physio ProtocolDocument6 pagesAcl Physio ProtocolAna MorenoNo ratings yet
- ACL Reconstruction ProtocolDocument23 pagesACL Reconstruction ProtocolRoberto Tommasini100% (2)
- Lumbar Spinal Fusion Exercises - Jan20Document4 pagesLumbar Spinal Fusion Exercises - Jan20TrisnadewiNo ratings yet
- Arthroscopic Labrum Repair of The Shoulder (SLAP) : AnatomyDocument16 pagesArthroscopic Labrum Repair of The Shoulder (SLAP) : AnatomyDruga Danut100% (1)
- Rotator Cuff Repair EbookDocument31 pagesRotator Cuff Repair EbookJohnPaulBascoNo ratings yet
- SLAP Lesion Repair Operation: A Guide For PatientsDocument12 pagesSLAP Lesion Repair Operation: A Guide For PatientsCiro AlbuquerqueNo ratings yet
- Cast CareDocument4 pagesCast CareRogelyn PatriarcaNo ratings yet
- Lumbar Laminectomy Relief for SciaticaDocument3 pagesLumbar Laminectomy Relief for SciaticaIndah ChristyNo ratings yet
- After Surgery Rehabilitation Program MPFL ReconstructionDocument12 pagesAfter Surgery Rehabilitation Program MPFL ReconstructionNedelcu NicolaeNo ratings yet
- Anterior Labral (Bankart) RepairsDocument13 pagesAnterior Labral (Bankart) RepairsChris CarmenNo ratings yet
- Post-Operative Exercise Program: Knee Joint Replacement SurgeryDocument16 pagesPost-Operative Exercise Program: Knee Joint Replacement SurgeryRamses DagoyNo ratings yet
- Shoulder Post-Operative Rehabilitation ProtocolsDocument6 pagesShoulder Post-Operative Rehabilitation ProtocolsShrutiNo ratings yet
- Total Elbow Arthroplasty and RehabilitationDocument5 pagesTotal Elbow Arthroplasty and RehabilitationMarina ENo ratings yet
- Adhesive Capsulitis or Frozen SholderDocument24 pagesAdhesive Capsulitis or Frozen Sholdersanalcrazy100% (1)
- Knee Arthroscopy ProgramDocument26 pagesKnee Arthroscopy ProgramDavid StoevskiNo ratings yet
- Post-operative and Pre-Prosthetic Management for AmputeesDocument38 pagesPost-operative and Pre-Prosthetic Management for AmputeesTanzeelah RajawNo ratings yet
- Rehab Bankart RepairDocument20 pagesRehab Bankart RepairtaingsNo ratings yet
- Shoulder Protocol Bankart Information: How The Shoulder WorksDocument4 pagesShoulder Protocol Bankart Information: How The Shoulder WorksKartick PaiNo ratings yet
- Acl Rehab ProtocolDocument18 pagesAcl Rehab Protocolapi-256259376No ratings yet
- ACL ReconstructionDocument24 pagesACL Reconstructionsamabdelaal2000No ratings yet
- Clavicle Fracture Protocol After Surgical RepairDocument20 pagesClavicle Fracture Protocol After Surgical RepairNicoGeorgescuNo ratings yet
- Anterior Cervical Diskectomy and Fusion (ACDF) : What Is Done During The Surgery? What Are The Risks of The Surgery?Document3 pagesAnterior Cervical Diskectomy and Fusion (ACDF) : What Is Done During The Surgery? What Are The Risks of The Surgery?Adi KNo ratings yet
- Role of Physiotherapy in Management of Burns-HshDocument25 pagesRole of Physiotherapy in Management of Burns-HshChristopher Chibueze Igbo100% (1)
- Physiotherapy InformationDocument16 pagesPhysiotherapy InformationAlejandro SanchezNo ratings yet
- ACL Reconstruction Rehabilitation Protocol GuideDocument18 pagesACL Reconstruction Rehabilitation Protocol GuiderajadigitalNo ratings yet
- Slap Tears-Orthoinfo - AaosDocument6 pagesSlap Tears-Orthoinfo - Aaosapi-228773845No ratings yet
- Post-Op Knee Arthroscopy InstructionsDocument4 pagesPost-Op Knee Arthroscopy InstructionsTusan SidhartaNo ratings yet
- NHS UK Rotator Cuff RepairDocument5 pagesNHS UK Rotator Cuff RepairmertNo ratings yet
- Rotator Cuff RepairDocument5 pagesRotator Cuff RepairAdhitya TaslimNo ratings yet
- Freeletics Workout PlanDocument5 pagesFreeletics Workout PlanMiguel OrdoñezNo ratings yet
- Safety TipsDocument16 pagesSafety TipsAnonymous do9rmemPDNo ratings yet
- Lumbar Disc HerniationDocument8 pagesLumbar Disc Herniationandra_scooterNo ratings yet
- Arthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDDocument8 pagesArthroscopic Shoulder Anterior Stabilisation Rehabilitation Protocol by TENDAYI MUTSOPOTSI MSc. ORTHO-MEDPhysiotherapy Care SpecialistsNo ratings yet
- FNCP OutputDocument6 pagesFNCP OutputRenz AnggoyNo ratings yet
- Paramedian Forehead Flap Nasal Reconstruction Surgical TechniqueDocument10 pagesParamedian Forehead Flap Nasal Reconstruction Surgical Techniquetegegnegenet2No ratings yet
- ChepalotomaDocument14 pagesChepalotomarosaNo ratings yet
- Detecting Hemoperitoneum: Limitations of Repeat FAST ExamsDocument123 pagesDetecting Hemoperitoneum: Limitations of Repeat FAST ExamsSinisa Ristic50% (2)
- Kimia Farma Per 30 September ZRMM076Document271 pagesKimia Farma Per 30 September ZRMM076SriyatiNo ratings yet
- Gerson Therapy Handbook-5th-Revision PDFDocument118 pagesGerson Therapy Handbook-5th-Revision PDFCelia Steiman100% (1)
- BupropionDocument23 pagesBupropiontheintrovNo ratings yet
- Increased Intracranial Pressure NCLEX ReviewDocument8 pagesIncreased Intracranial Pressure NCLEX ReviewAnia JuanNo ratings yet
- Amniotic MembraneDocument8 pagesAmniotic Membraneapi-481789048No ratings yet
- Aubf MergeDocument164 pagesAubf MergeVia Gail CanlasNo ratings yet
- Anatomy of The Hepatobiliary System MaranDocument18 pagesAnatomy of The Hepatobiliary System Maransgod34No ratings yet
- 2 Pathophysiology EpidemiologyDocument36 pages2 Pathophysiology EpidemiologyYosefina CindyNo ratings yet
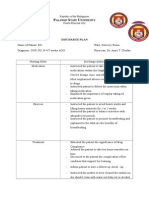
- Discharge Plan: Alawan Tate NiversityDocument2 pagesDischarge Plan: Alawan Tate NiversityLenieGracePascoNo ratings yet
- Rose Geranium in Sesame Oil NasalDocument3 pagesRose Geranium in Sesame Oil NasalHolly JonesNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- Ahlskog Et Al. Mayo Clin Proc 2011Document9 pagesAhlskog Et Al. Mayo Clin Proc 2011Thais AmandaNo ratings yet
- Angioedema 4Document18 pagesAngioedema 4Venosha GunasekaranNo ratings yet
- Clinical RotationDocument2 pagesClinical RotationDarwin QuirimitNo ratings yet
- Recurrent/Persistent Pneumonia Among Children in Upper EgyptDocument14 pagesRecurrent/Persistent Pneumonia Among Children in Upper EgyptLaila Ninda ShofiaNo ratings yet
- Psychiatric Case Write Up on Brief Psychotic DisorderDocument10 pagesPsychiatric Case Write Up on Brief Psychotic DisorderBen Man JunNo ratings yet
- Cerebrovascular AccidentDocument62 pagesCerebrovascular AccidentJaydee DalayNo ratings yet
- The Voice of PLC 1101Document6 pagesThe Voice of PLC 1101The Plymouth Laryngectomy ClubNo ratings yet
- Infectious Bronchitis and Its Effect On Egg Production and Egg QualityDocument2 pagesInfectious Bronchitis and Its Effect On Egg Production and Egg QualityPrima Puji RaharjoNo ratings yet
- Ent Bcqs 2Document22 pagesEnt Bcqs 2Ghazi Uddin Ahmed100% (1)
- Pathophysiology A Clinical Approach 2nd Edition Braun Anderson Test BankDocument36 pagesPathophysiology A Clinical Approach 2nd Edition Braun Anderson Test Bankbeswikemysteryy6rpNo ratings yet
- JCDP 22 310Document6 pagesJCDP 22 310Anand MohattaNo ratings yet
- Inflammatory Bowel Disease and Carcinogenesis: Hiroko Nagao Kitamoto Sho Kitamoto Nobuhiko KamadaDocument16 pagesInflammatory Bowel Disease and Carcinogenesis: Hiroko Nagao Kitamoto Sho Kitamoto Nobuhiko KamadaDiego Fernando Ortiz TenorioNo ratings yet
- Informed Consent For Lasik SurgeryDocument2 pagesInformed Consent For Lasik SurgeryMoerieda RinquestNo ratings yet
- H. PyloriDocument5 pagesH. PyloriWaleed El SaidNo ratings yet
- Surat Dental 181Document15 pagesSurat Dental 181deva nesanNo ratings yet