You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Magic Frequencies: Excerpted From The Mixing Engineer's HandbookDocument5 pagesMagic Frequencies: Excerpted From The Mixing Engineer's HandbookmehmetkurtulusNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ancient Skies of Northern Europe: Stars, Constellations, and The Moon in Nordic MythologyDocument12 pagesAncient Skies of Northern Europe: Stars, Constellations, and The Moon in Nordic MythologyoldenglishblogNo ratings yet
- Livro Vertex MACIOCIADocument62 pagesLivro Vertex MACIOCIAxandinhag100% (5)
- 974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Document64 pages974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Leo BurnsNo ratings yet
- Newton Papers Letter Nat Phil Cohen EdDocument512 pagesNewton Papers Letter Nat Phil Cohen EdFernando ProtoNo ratings yet
- Polynesian MigrationsDocument2 pagesPolynesian Migrationskinneyjeffrey100% (1)
- The Word Became Flesh An Exploratory Essay On Jesu 003Document62 pagesThe Word Became Flesh An Exploratory Essay On Jesu 003Alexios VrionisNo ratings yet
- Quiz 2 Principles of DesignDocument4 pagesQuiz 2 Principles of DesignJovito Reyes0% (1)
- BCA 5005 Minor Project Synopsis Format & GuidelinesDocument7 pagesBCA 5005 Minor Project Synopsis Format & GuidelinesAnu VermaNo ratings yet
- JVC KD-G331Document179 pagesJVC KD-G331Saša DumanovićNo ratings yet
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Dr. M. Syed Jamil Asghar: Paper Published: 80Document6 pagesDr. M. Syed Jamil Asghar: Paper Published: 80Awaiz NoorNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- Poisson, Poisson-Gamma and Zero-Inflated Regression ModelsDocument43 pagesPoisson, Poisson-Gamma and Zero-Inflated Regression ModelszohrehNo ratings yet
- Sa 387Document6 pagesSa 387ismaelarchilacastilloNo ratings yet
- Consola Phonic CELEUS800 en EspañolDocument32 pagesConsola Phonic CELEUS800 en EspañolRoberto BurgosNo ratings yet
- Riparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesDocument12 pagesRiparian Flora of Kaliwa River Watershed in The Sierra Madre Mountain Range, PhilippinesMichael Angelo ValdezNo ratings yet
- Algebra I m5 Topic B Lesson 6 TeacherDocument13 pagesAlgebra I m5 Topic B Lesson 6 TeacherjxhroyNo ratings yet
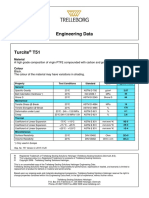
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- 1cobalt Is An Element in Period 4 of The Periodic TableDocument3 pages1cobalt Is An Element in Period 4 of The Periodic TableZigla MooreNo ratings yet
- Matter 1A Forms Properties and ChangesDocument47 pagesMatter 1A Forms Properties and ChangesSamKris Guerrero Malasaga100% (2)
- Real Time DC Water Tank Level Control Using Arduino Mega 2560Document6 pagesReal Time DC Water Tank Level Control Using Arduino Mega 2560Sam ArNo ratings yet
- Valores de Laboratorio Harriet LaneDocument14 pagesValores de Laboratorio Harriet LaneRonald MoralesNo ratings yet
- 10069-9-V01-Ef00-00039 Fire Alarm SystemDocument49 pages10069-9-V01-Ef00-00039 Fire Alarm Systemahffg nnffNo ratings yet
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- Car Frontal ImpactDocument25 pagesCar Frontal Impactapi-3762972100% (1)
- ActuatorsDocument24 pagesActuatorsharishcsharmaNo ratings yet
- cs229.... Machine Language. Andrew NGDocument17 pagescs229.... Machine Language. Andrew NGkrishnaNo ratings yet
- Seajet 118 Ultra-Build Epoxy PrimerDocument2 pagesSeajet 118 Ultra-Build Epoxy PrimerRai Hasnain Ahmad DahaNo ratings yet
- Unit 2 SignalsDocument3 pagesUnit 2 SignalsDigitallogicdlNo ratings yet