You might also like
- Endocrinology and DiabetesDocument766 pagesEndocrinology and DiabetesDr. Salvador Muñoz BarriosNo ratings yet
- By Douglas Mulhall: © May-July 2005Document6 pagesBy Douglas Mulhall: © May-July 2005JOSH USHERNo ratings yet
- Tulio E. Bertorini - Neuromuscular DisordersDocument466 pagesTulio E. Bertorini - Neuromuscular DisordersLeila Gonzalez100% (1)
- Drogas RenalDocument69 pagesDrogas RenalJamerson Carvalho100% (1)
- Renukaprasad Ys - Medicine - Thesis NewDocument110 pagesRenukaprasad Ys - Medicine - Thesis NewLokesh ChopraNo ratings yet
- Nammiaca 000032Document5,323 pagesNammiaca 000032gangadhark196No ratings yet
- FPAL Product Code GuideDocument53 pagesFPAL Product Code GuideSRARNo ratings yet
- Check - Unit - 554 - October - Renal - Problems V2 PDFDocument26 pagesCheck - Unit - 554 - October - Renal - Problems V2 PDFdragon660% (1)
- Woltering's New BookDocument265 pagesWoltering's New Bookapi-3775442No ratings yet
- BCBR - Review + Cycle 3Document103 pagesBCBR - Review + Cycle 3Dr. Richa Choudhary89% (9)
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDocument209 pagesACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34No ratings yet
- PrediabetesDocument8 pagesPrediabetesVimal NishadNo ratings yet
- Guide To Greyhawk PDFDocument108 pagesGuide To Greyhawk PDFAnonymous PtMxUHm9RoNo ratings yet
- Varaah KavachDocument7 pagesVaraah KavachBalagei Nagarajan100% (1)
- Taper Lock BushesDocument4 pagesTaper Lock BushesGopi NathNo ratings yet
- National Kidney Foundation Position PaperDocument4 pagesNational Kidney Foundation Position PaperGenesis HendraNo ratings yet
- Swallowing Dysfunction After Critical IllnessDocument9 pagesSwallowing Dysfunction After Critical IllnessGisele DiasNo ratings yet
- 1 s2.0 S105122762300105X MainDocument11 pages1 s2.0 S105122762300105X MainJulia KhaerunisaNo ratings yet
- Introduction To Critical Care Nephrology and Acute Kidney InjuryDocument2 pagesIntroduction To Critical Care Nephrology and Acute Kidney Injuryjesus garcia solanoNo ratings yet
- PIIS008525381546747XDocument15 pagesPIIS008525381546747XBintiNo ratings yet
- Steroid-AssociatedSideEffectsinPatients WithPrimaryProteinuricKidneyDiseaseDocument9 pagesSteroid-AssociatedSideEffectsinPatients WithPrimaryProteinuricKidneyDiseaseIndah SolehaNo ratings yet
- Thesis On Chronic Kidney DiseaseDocument5 pagesThesis On Chronic Kidney Diseasebrendahigginsarlington100% (2)
- Consensus Based Recommendations For The ManagementDocument14 pagesConsensus Based Recommendations For The Managementranjani093No ratings yet
- 23 732938 Brochure FINALDocument8 pages23 732938 Brochure FINALfouad tabetNo ratings yet
- Ca - Acute Renal FailureDocument51 pagesCa - Acute Renal FailureCharisse CaydanNo ratings yet
- Adult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesDocument9 pagesAdult Minimal-Change Disease: Clinical Characteristics, Treatment, and OutcomesMutiara RizkyNo ratings yet
- Differential Diagnosis in Surgical Pathology - Pulmonary Pathology (PDFDrive)Document740 pagesDifferential Diagnosis in Surgical Pathology - Pulmonary Pathology (PDFDrive)Tan Zhen YiNo ratings yet
- Short-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyDocument12 pagesShort-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyTJPRC PublicationsNo ratings yet
- Summary 2014Document16 pagesSummary 2014Adrian ZapataNo ratings yet
- Pediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyDocument5 pagesPediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyagusNo ratings yet
- Pneumonia in Acute Stroke Patients Fed by Nasogastric Tube: PaperDocument5 pagesPneumonia in Acute Stroke Patients Fed by Nasogastric Tube: PaperLira PurnamawatiNo ratings yet
- Nut in Clin Prac - 2021 - Powers - Development of A Competency Model For Placement and Verification of Nasogastric andDocument17 pagesNut in Clin Prac - 2021 - Powers - Development of A Competency Model For Placement and Verification of Nasogastric andanonNo ratings yet
- 1 s2.0 S0002934314006871 Main PDFDocument9 pages1 s2.0 S0002934314006871 Main PDFcarlos orjuelaNo ratings yet
- Comparative Effectiveness of Diuretic Regimens: EditorialDocument2 pagesComparative Effectiveness of Diuretic Regimens: EditorialFabio Luis Padilla AvilaNo ratings yet
- The Recommendations of A Consensus Panel For The Screening, Diagnosis, and Treatment of Neurogenic Orthostatic Hypotension and Associated Supine Hypertension (Journal of Neurology, 2017)Document16 pagesThe Recommendations of A Consensus Panel For The Screening, Diagnosis, and Treatment of Neurogenic Orthostatic Hypotension and Associated Supine Hypertension (Journal of Neurology, 2017)mysticmdNo ratings yet
- 16 PDFDocument8 pages16 PDFAkhileshNo ratings yet
- Pielonefritis Enfisematos NatureDocument8 pagesPielonefritis Enfisematos NatureJose Guadalupe Martinez AlonsoNo ratings yet
- Ijnrd 8 125Document13 pagesIjnrd 8 125Muhammad Halil GibranNo ratings yet
- FA - Metabolomic and Biochemical Characterization of A New Model of The Transition of Acute Kidney Injury To Chronic Kidney Disease Induced by Folic AcidDocument26 pagesFA - Metabolomic and Biochemical Characterization of A New Model of The Transition of Acute Kidney Injury To Chronic Kidney Disease Induced by Folic AcidCher IshNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- Sample Qualipheno DialysisDocument202 pagesSample Qualipheno Dialysisnoronisa talusobNo ratings yet
- Kalantar Zadeh Etal 2021 Preserving Kidney Function in PeopleDocument61 pagesKalantar Zadeh Etal 2021 Preserving Kidney Function in Peoplenpuspa243No ratings yet
- Research Paper On Polycystic Kidney DiseaseDocument4 pagesResearch Paper On Polycystic Kidney Diseaseafeeotove100% (1)
- Enhanced Recovery After Surgery For Cesarean.24Document3 pagesEnhanced Recovery After Surgery For Cesarean.24grace liwantoNo ratings yet
- Kidney Disease Research PaperDocument6 pagesKidney Disease Research Papergz8aqe8wNo ratings yet
- 1 s2.0 S1051227616301789 MainDocument7 pages1 s2.0 S1051227616301789 MainResearch OfficeNo ratings yet
- Update On Psychotropic Medication Use in Renal DiseaseDocument15 pagesUpdate On Psychotropic Medication Use in Renal DiseaseMartinaNo ratings yet
- Efficacy of Dietary Interventions in End-Stage Renal Disease Patients A Systematic ReviewDocument13 pagesEfficacy of Dietary Interventions in End-Stage Renal Disease Patients A Systematic ReviewKhusnu Waskithoningtyas NugrohoNo ratings yet
- Wa0007Document17 pagesWa0007Eko WidodoNo ratings yet
- Handbook of GlomerulonephritisDocument456 pagesHandbook of Glomerulonephritiscorazones.232.mgNo ratings yet
- Septic ShockDocument12 pagesSeptic ShockPatrick CommettantNo ratings yet
- Nerjm SesionDocument12 pagesNerjm SesionjorgeNo ratings yet
- The Silent Gap Between Epilepsy Surgery Evaluations and Clinical Practice GuidelinesDocument2 pagesThe Silent Gap Between Epilepsy Surgery Evaluations and Clinical Practice GuidelinesAmelia PratiwiNo ratings yet
- Global Kidney Disease 1: SeriesDocument12 pagesGlobal Kidney Disease 1: Seriesalex lNo ratings yet
- Nephrology Module: 2007/8 Curriculum: Year 4 & 5 Undergraduate MedicineDocument7 pagesNephrology Module: 2007/8 Curriculum: Year 4 & 5 Undergraduate MedicineemmaNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- PROCESSDocument11 pagesPROCESSandrea vargasNo ratings yet
- Serum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyDocument7 pagesSerum Electrolyte Levels and Outcomes in Patients Hospitalized With Hepatic EncephalopathyhimayatullahNo ratings yet
- 200100409priti BhamaDocument70 pages200100409priti BhamaDr. PrinceNo ratings yet
- Vestibular CPG JNPT 2016 FinalDocument33 pagesVestibular CPG JNPT 2016 FinalMairaNo ratings yet
- The Value of Repeat Biopsy in SLEDocument8 pagesThe Value of Repeat Biopsy in SLESergio CerpaNo ratings yet
- Research Papers On Chronic Kidney DiseaseDocument9 pagesResearch Papers On Chronic Kidney Diseaseaflbtlzaw100% (1)
- Cerebral Vascular Accident Confounded by Parkinsons Disease - A CDocument28 pagesCerebral Vascular Accident Confounded by Parkinsons Disease - A CSavannah GreyNo ratings yet
- Laringo y BroncoespasmoDocument4 pagesLaringo y BroncoespasmoLUIS FERNANDO GOMEZ CANONo ratings yet
- Guia Vestibular 2016Document32 pagesGuia Vestibular 2016Paul Lavados ZavallaNo ratings yet
- Seminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDocument17 pagesSeminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicJack JackNo ratings yet
- Pulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseFrom EverandPulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseOscar Henry MayerNo ratings yet
- Hipertensión Pulmonar (2022)Document114 pagesHipertensión Pulmonar (2022)Mauricio CabreraNo ratings yet
- European J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalDocument19 pagesEuropean J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalVimal NishadNo ratings yet
- ARRYHTHMIADocument122 pagesARRYHTHMIAVimal NishadNo ratings yet
- Vimal PAD - SlidesDocument53 pagesVimal PAD - SlidesVimal NishadNo ratings yet
- Heart Sounds S2Document31 pagesHeart Sounds S2Vimal NishadNo ratings yet
- pm0150 LooksteinRobert Debulki MondayDocument27 pagespm0150 LooksteinRobert Debulki MondayVimal NishadNo ratings yet
- Seminar TopicsDocument4 pagesSeminar TopicsVimal NishadNo ratings yet
- Index of Microcirculatory Resistance:: The BasicsDocument54 pagesIndex of Microcirculatory Resistance:: The BasicsVimal NishadNo ratings yet
- Merchant 2019Document7 pagesMerchant 2019Vimal NishadNo ratings yet
- Mcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseDocument25 pagesMcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseVimal NishadNo ratings yet
- Medicine Emergency ChartsDocument1 pageMedicine Emergency ChartsVimal NishadNo ratings yet
- Transcatheter Therapies For Valvular Heart DiseaseDocument10 pagesTranscatheter Therapies For Valvular Heart DiseaseVimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Fluid and ElectrolyteDocument6 pagesFluid and ElectrolyteVimal NishadNo ratings yet
- Evaluation of EndotheliumDocument3 pagesEvaluation of EndotheliumVimal NishadNo ratings yet
- TBM 1Document2 pagesTBM 1Vimal NishadNo ratings yet
- Towards Developing A Scoring System For Febrile ThrombocytopeniaDocument5 pagesTowards Developing A Scoring System For Febrile ThrombocytopeniaVimal NishadNo ratings yet
- CardiologyDocument29 pagesCardiologyVimal NishadNo ratings yet
- 12 OA Evaluation of Febrile Thrombocytopenia CasesDocument5 pages12 OA Evaluation of Febrile Thrombocytopenia CasesVimal NishadNo ratings yet
- Questions On The Kidney and Urinary Tract-2Document7 pagesQuestions On The Kidney and Urinary Tract-2Vimal NishadNo ratings yet
- Mesna PM ENG v4.0 011218Document23 pagesMesna PM ENG v4.0 011218Vimal NishadNo ratings yet
- Mod Rhuematic Fever Final PDFDocument90 pagesMod Rhuematic Fever Final PDFVimal NishadNo ratings yet
- 483 PDFDocument6 pages483 PDFVimal NishadNo ratings yet
- Neet As OrderDocument1 pageNeet As OrderVimal NishadNo ratings yet
- Neurophysiology Quiz Oct 03Document3 pagesNeurophysiology Quiz Oct 03Vimal NishadNo ratings yet
- PDFDocument1 pagePDFVimal NishadNo ratings yet
- S 5359 LBLDocument58 pagesS 5359 LBLNidershan SuguneshwaranNo ratings yet
- Ge Druck PTX 7535Document2 pagesGe Druck PTX 7535ICSSNo ratings yet
- VlsiDocument79 pagesVlsimdhuq1No ratings yet
- Genie Z45/22Document58 pagesGenie Z45/22jonny david martinez perezNo ratings yet
- Chinese ArchitectureDocument31 pagesChinese Architecturenusantara knowledge100% (2)
- Mercedes (DTC) 976990001963 20220615144147Document3 pagesMercedes (DTC) 976990001963 20220615144147YB MOTOR Nissan - Datsun SpecialistNo ratings yet
- Amies A 114 - 3Document17 pagesAmies A 114 - 3Syed Umar Farooq100% (1)
- KZPOWER Perkins Stamford Genset Range CatalogueDocument2 pagesKZPOWER Perkins Stamford Genset Range CatalogueWiratama TambunanNo ratings yet
- Lcnews227 - Nexera SeriesDocument47 pagesLcnews227 - Nexera SeriesMuhammad RohmanNo ratings yet
- The Sea DevilDocument6 pagesThe Sea DevilRevthi SankerNo ratings yet
- AC350 Specs UsDocument18 pagesAC350 Specs Uskloic1980100% (1)
- Module 12. Big Issues Lesson 12a. Reading. Pages 140-141: No Words TranslationDocument4 pagesModule 12. Big Issues Lesson 12a. Reading. Pages 140-141: No Words TranslationLeonardo Perez AlegriaNo ratings yet
- Study of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderDocument3 pagesStudy of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderAnonymous AkoNo ratings yet
- Digital Trail Camera: Instruction ManualDocument20 pagesDigital Trail Camera: Instruction Manualdavid churaNo ratings yet
- Chemistry NotesDocument11 pagesChemistry Notesraifaisal9267% (12)
- Epilepsy Lecture NoteDocument15 pagesEpilepsy Lecture Notetamuno7100% (2)
- ScilabDocument4 pagesScilabAngeloLorenzoSalvadorTamayoNo ratings yet
- NARS Fall 2011 Press File PDFDocument19 pagesNARS Fall 2011 Press File PDFheather_dillowNo ratings yet
- NCERT Solutions For Class 12 Maths Chapter 10 Vector AlgebraDocument51 pagesNCERT Solutions For Class 12 Maths Chapter 10 Vector AlgebraKavin .J.S (KingK)No ratings yet
- Popular CultureDocument6 pagesPopular CultureAmritaNo ratings yet
- Phonetics ReportDocument53 pagesPhonetics ReportR-jhay Mepusa AceNo ratings yet
- InTech-Batteries Charging Systems For Electric and Plug in Hybrid Electric VehiclesDocument20 pagesInTech-Batteries Charging Systems For Electric and Plug in Hybrid Electric VehiclesM VetriselviNo ratings yet
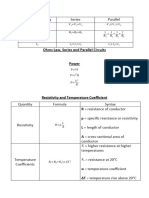
- EET - Formulas - Christmas TermDocument3 pagesEET - Formulas - Christmas TermJMDNo ratings yet
- PDFDocument8 pagesPDFDocNo ratings yet
- Modern Views Catalogue/Sotheby's BenefitDocument36 pagesModern Views Catalogue/Sotheby's BenefitStudio AdjayeNo ratings yet