You might also like
- Coronary Artery DiseaseDocument82 pagesCoronary Artery Diseasecortassa265No ratings yet
- 4conference mv2 HKR PDFDocument87 pages4conference mv2 HKR PDFekafithraNo ratings yet
- Fractional Flow ReserveDocument44 pagesFractional Flow Reserveusfcards100% (2)
- 09.30 Professor John Townend, Chest Pain and Troponins On The Acute TakeDocument39 pages09.30 Professor John Townend, Chest Pain and Troponins On The Acute Takeamir ahmadNo ratings yet
- Parameter Echo Ase Eka FixDocument59 pagesParameter Echo Ase Eka Fixdian asrianaNo ratings yet
- Ischemic Mitral Regurgitation Repair or Replace ?: Patrick F. WOUTERS Ghent, BelgiumDocument26 pagesIschemic Mitral Regurgitation Repair or Replace ?: Patrick F. WOUTERS Ghent, BelgiumDana BursacovschiNo ratings yet
- Qualitative and Quantitative Comparison of Tgrappa and Tsense Real Time Cine Techniques During Deep BreathingDocument316 pagesQualitative and Quantitative Comparison of Tgrappa and Tsense Real Time Cine Techniques During Deep BreathingRadhaRajasekaranNo ratings yet
- 1 s2.0 S0735109716353086 MainDocument3 pages1 s2.0 S0735109716353086 MainPaul CalbureanNo ratings yet
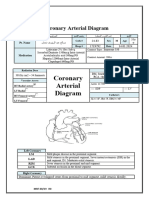
- Coronary Arterial DiagramDocument3 pagesCoronary Arterial Diagramshamaamo19No ratings yet
- Coumadin Clinics and POCT 092310Document51 pagesCoumadin Clinics and POCT 092310tungNo ratings yet
- 1 s2.0 S0002914901021981 MainDocument7 pages1 s2.0 S0002914901021981 MainLuisa OsorioNo ratings yet
- HC3600 Precision AC Power Working Standards: Terminology and Operation InterfaceDocument40 pagesHC3600 Precision AC Power Working Standards: Terminology and Operation InterfaceRamdan suprianaNo ratings yet
- Iacta 2011 Janak Mehta Award Winning PresentationDocument56 pagesIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNo ratings yet
- 307 RogersDocument23 pages307 Rogersdakic85No ratings yet
- Confounding Stratification22Document26 pagesConfounding Stratification22AriefWicaksonoNo ratings yet
- 03 - Echocardiography and Imaging 49: ResultsDocument2 pages03 - Echocardiography and Imaging 49: ResultsJussara FerreiraNo ratings yet
- Carpentier Mitral Valve Regurgitation ClasifDocument45 pagesCarpentier Mitral Valve Regurgitation ClasifKudor Szabadi Zoltán100% (1)
- Moartea Subita CardiacaDocument63 pagesMoartea Subita CardiacaAlexa whyNo ratings yet
- Leipsic-MDCT For TAVRDocument58 pagesLeipsic-MDCT For TAVRLuz Dinora Sandoval CastilloNo ratings yet
- Adhip Shukla-16Ume003 Akshat Sharma-16Uec014 Devesh Sharma-16Uec035 Raushan Kumar Jha-16Uec081 Shravan Tawri-16Ume046Document38 pagesAdhip Shukla-16Ume003 Akshat Sharma-16Uec014 Devesh Sharma-16Uec035 Raushan Kumar Jha-16Uec081 Shravan Tawri-16Ume046Adhip ShuklaNo ratings yet
- Physiology NandaDocument41 pagesPhysiology NandaHaverson LethulurNo ratings yet
- Angiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialDocument26 pagesAngiotensin Receptor Neprilysin Inhibition (ARNI) Following Acute Myocardial Infarction: Primary Results of The PARADISE-MI TrialsumaNo ratings yet
- 1 s2.0 S0735109707035796 MainDocument6 pages1 s2.0 S0735109707035796 MainIván CornejoNo ratings yet
- High Prosthetic Gradient: Is This Prosthesis Dysfunction or Prosthesis-Patient Mismatch?Document46 pagesHigh Prosthetic Gradient: Is This Prosthesis Dysfunction or Prosthesis-Patient Mismatch?raghesh VNo ratings yet
- Urinary Diversion After Radical Cystectomy Ileal Conduit or Transuretero-Cutaneostomy?Document1 pageUrinary Diversion After Radical Cystectomy Ileal Conduit or Transuretero-Cutaneostomy?Indra JayaNo ratings yet
- MonitoringDocument128 pagesMonitoringShahzada irfanNo ratings yet
- Noninvasive Cardiac Output Monitoring (NICOM) : A Clinical ValidationDocument4 pagesNoninvasive Cardiac Output Monitoring (NICOM) : A Clinical Validationdrcds99No ratings yet
- Short NoteDocument8 pagesShort Notema9858056No ratings yet
- "How We Do" CMR in Acute Myocardial Infarction: Derek J Hausenloy, Anna S Herrey, James C MoonDocument17 pages"How We Do" CMR in Acute Myocardial Infarction: Derek J Hausenloy, Anna S Herrey, James C Moon祁晓浪No ratings yet
- Triger ChirurgicalDocument7 pagesTriger ChirurgicalPanfilAlinaNo ratings yet
- 400pmET Transcatheter Tricuspid Valve Treatment TCT 2019Document22 pages400pmET Transcatheter Tricuspid Valve Treatment TCT 2019KushanNo ratings yet
- Manoj SirDocument27 pagesManoj SirANKURNo ratings yet
- Ma Chap3Document10 pagesMa Chap3sheokandmanjeetNo ratings yet
- How Does Intravascular ImagingDerived FFR Work and When Should It Be UsedDocument25 pagesHow Does Intravascular ImagingDerived FFR Work and When Should It Be Usedrainmed USNo ratings yet
- Liquefaction SPTDocument5 pagesLiquefaction SPTJohnNo ratings yet
- CT PT CVT 16012014 PDFDocument69 pagesCT PT CVT 16012014 PDFPramod Bhoir100% (1)
- Definition of Acute Coronary Syndrome: Creatine Kinase (CK) Versus Troponin T (TNT) Plotted On A Log ScaleDocument15 pagesDefinition of Acute Coronary Syndrome: Creatine Kinase (CK) Versus Troponin T (TNT) Plotted On A Log ScaleFebryNo ratings yet
- Trauma Management Information Pra HospitalDocument39 pagesTrauma Management Information Pra HospitalcaroliaNo ratings yet
- Pla2.5k 60 1000Document2 pagesPla2.5k 60 1000Suman RachaNo ratings yet
- Sca 2019Document69 pagesSca 2019PLIFNo ratings yet
- Lab Report NewDocument6 pagesLab Report NewPriya DubeyNo ratings yet
- Mitral StenosisDocument31 pagesMitral StenosisArtemisNo ratings yet
- Intraoperative Monitoring: Dr. M. FadhillahDocument52 pagesIntraoperative Monitoring: Dr. M. Fadhillahfadil85No ratings yet
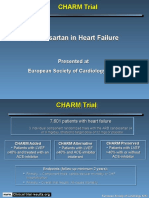
- Candesartan in Heart Failure Candesartan in Heart FailureDocument8 pagesCandesartan in Heart Failure Candesartan in Heart FailureHassan RazaNo ratings yet
- Candesartan in Heart Failure Candesartan in Heart FailureDocument8 pagesCandesartan in Heart Failure Candesartan in Heart FailureNawel BenNo ratings yet
- 1 TonometryDocument39 pages1 TonometrySri Rama Chandra ManchikantyNo ratings yet
- JournalDocument1 pageJournalAdli Wafi JabbarNo ratings yet
- Tugas ADK-resultsDocument26 pagesTugas ADK-resultsal fathNo ratings yet
- Huntron Htr-1005b Maintenance SCHDocument38 pagesHuntron Htr-1005b Maintenance SCHRodolfoBucaloNo ratings yet
- Numbers To Remember COREDocument15 pagesNumbers To Remember COREConcierge Health InternationalNo ratings yet
- Paradise TrialDocument26 pagesParadise TrialMiguel Martinez DuranNo ratings yet
- 0915 - Thomas - Zeller - 31 - 01 - 2018 - Room - 1 - Main - Arena - 1 - v2 UpDocument17 pages0915 - Thomas - Zeller - 31 - 01 - 2018 - Room - 1 - Main - Arena - 1 - v2 UpBHAVANA VNNo ratings yet
- Voorna OutputDocument7 pagesVoorna OutputGeertNo ratings yet
- Qa Tolerances FinalDocument38 pagesQa Tolerances Finalapi-356919224No ratings yet
- Cardiac Resynchronization Therapy, Robotic LV Epicardial Lead Placement: Indications and TechniqueDocument34 pagesCardiac Resynchronization Therapy, Robotic LV Epicardial Lead Placement: Indications and TechniquedcicareNo ratings yet
- Sunbeam CorporationDocument2 pagesSunbeam CorporationArch Faith Lejarso-SerisolaNo ratings yet
- Biomedical Engineering Biomedizinische TechnikDocument10 pagesBiomedical Engineering Biomedizinische TechnikJayanthi ThiruvengadamNo ratings yet
- DR Muhadi - Workshop Basic Echo PW CW PIN 2019Document39 pagesDR Muhadi - Workshop Basic Echo PW CW PIN 2019Zakka JayadisastraNo ratings yet
- Clinical Nuclear Cardiology: Practical Applications and Future DirectionsFrom EverandClinical Nuclear Cardiology: Practical Applications and Future DirectionsNo ratings yet
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- Hipertensión Pulmonar (2022)Document114 pagesHipertensión Pulmonar (2022)Mauricio CabreraNo ratings yet
- European J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalDocument19 pagesEuropean J of Heart Fail - 2022 - Guazzi - Exercise Testing in Heart Failure With Preserved Ejection Fraction An AppraisalVimal NishadNo ratings yet
- ARRYHTHMIADocument122 pagesARRYHTHMIAVimal NishadNo ratings yet
- Vimal PAD - SlidesDocument53 pagesVimal PAD - SlidesVimal NishadNo ratings yet
- BCBR - Review + Cycle 3Document103 pagesBCBR - Review + Cycle 3Dr. Richa Choudhary89% (9)
- Heart Sounds S2Document31 pagesHeart Sounds S2Vimal NishadNo ratings yet
- pm0150 LooksteinRobert Debulki MondayDocument27 pagespm0150 LooksteinRobert Debulki MondayVimal NishadNo ratings yet
- Seminar TopicsDocument4 pagesSeminar TopicsVimal NishadNo ratings yet
- Merchant 2019Document7 pagesMerchant 2019Vimal NishadNo ratings yet
- Transcatheter Therapies For Valvular Heart DiseaseDocument10 pagesTranscatheter Therapies For Valvular Heart DiseaseVimal NishadNo ratings yet
- Medicine Emergency ChartsDocument1 pageMedicine Emergency ChartsVimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Mcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseDocument25 pagesMcqs in Cardiology Based On Braunwald by Dr. Adithya Udupa K Aortic Valve DiseaseVimal NishadNo ratings yet
- Assessment of Glycemic Status, Insulin Resistance and HypogonadismDocument5 pagesAssessment of Glycemic Status, Insulin Resistance and HypogonadismVimal NishadNo ratings yet
- Towards Developing A Scoring System For Febrile ThrombocytopeniaDocument5 pagesTowards Developing A Scoring System For Febrile ThrombocytopeniaVimal NishadNo ratings yet
- Mesna PM ENG v4.0 011218Document23 pagesMesna PM ENG v4.0 011218Vimal NishadNo ratings yet
- 12 OA Evaluation of Febrile Thrombocytopenia CasesDocument5 pages12 OA Evaluation of Febrile Thrombocytopenia CasesVimal NishadNo ratings yet
- Questions On The Kidney and Urinary Tract-2Document7 pagesQuestions On The Kidney and Urinary Tract-2Vimal NishadNo ratings yet
- Evaluation of EndotheliumDocument3 pagesEvaluation of EndotheliumVimal NishadNo ratings yet
- TBM 1Document2 pagesTBM 1Vimal NishadNo ratings yet
- CardiologyDocument29 pagesCardiologyVimal NishadNo ratings yet
- Fluid and ElectrolyteDocument6 pagesFluid and ElectrolyteVimal NishadNo ratings yet
- PDFDocument1 pagePDFVimal NishadNo ratings yet
- Mod Rhuematic Fever Final PDFDocument90 pagesMod Rhuematic Fever Final PDFVimal NishadNo ratings yet
- 483 PDFDocument6 pages483 PDFVimal NishadNo ratings yet
- PrediabetesDocument8 pagesPrediabetesVimal NishadNo ratings yet
- Neet As OrderDocument1 pageNeet As OrderVimal NishadNo ratings yet
- Neurophysiology Quiz Oct 03Document3 pagesNeurophysiology Quiz Oct 03Vimal NishadNo ratings yet
- S 5359 LBLDocument58 pagesS 5359 LBLNidershan SuguneshwaranNo ratings yet
- Vascular Dementia: By: Omar Nuhic 4th Year Student Subject: PsychiatryDocument10 pagesVascular Dementia: By: Omar Nuhic 4th Year Student Subject: PsychiatryOmar NuhicNo ratings yet
- Predictor Scale of Delayed Cerebral Ischemic in Aneurysmal Subarachnoid Hemorrhage Case Series: What A Radiologist Should KnowDocument5 pagesPredictor Scale of Delayed Cerebral Ischemic in Aneurysmal Subarachnoid Hemorrhage Case Series: What A Radiologist Should KnowPopy TheresiaNo ratings yet
- Molecules, Transport and HealthDocument29 pagesMolecules, Transport and Healthkamrunnisa100% (1)
- Science 9 W1-W4Document21 pagesScience 9 W1-W4Jennifer Lacadue Masoa - LumantasNo ratings yet
- Ebook Vascular Medicine A Companion To Braunwalds Heart Disease PDF Full Chapter PDFDocument67 pagesEbook Vascular Medicine A Companion To Braunwalds Heart Disease PDF Full Chapter PDFelsie.mcintyre883100% (27)
- Hypoxic Ischemic EncephalopathyDocument20 pagesHypoxic Ischemic Encephalopathyejikieru03No ratings yet
- Group Discussion Second Year Cardiovascular SystemDocument2 pagesGroup Discussion Second Year Cardiovascular Systemola nagarNo ratings yet
- Introduction To The CvsDocument43 pagesIntroduction To The CvsParmesh PandeyNo ratings yet
- CV SUPRIYATNO - UpdateDocument3 pagesCV SUPRIYATNO - UpdateSayung IchaNo ratings yet
- Pulsus ParadoxusDocument2 pagesPulsus ParadoxusHassan.shehriNo ratings yet
- In Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinusDocument7 pagesIn Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinushelloaNo ratings yet
- Overview of Nurses' Role in Management of Patient With Atrial FibrillationDocument5 pagesOverview of Nurses' Role in Management of Patient With Atrial FibrillationAhmed AlkhaqaniNo ratings yet
- Mics 1Document7 pagesMics 1Ramya ENo ratings yet
- Transport SystemDocument2 pagesTransport Systemgnana87No ratings yet
- Effect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseDocument4 pagesEffect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseFitratun NajizahNo ratings yet
- SEX DifferencesDocument12 pagesSEX DifferencesSubhashini KNo ratings yet
- MEGACODEDocument6 pagesMEGACODESafety JNo ratings yet
- 10 Steps To Learn ECG InterpretationDocument5 pages10 Steps To Learn ECG InterpretationMohammadNo ratings yet
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Vascular Surgery MedCosmos Surgery - MCQDocument34 pagesVascular Surgery MedCosmos Surgery - MCQMike GNo ratings yet
- Pex 06 01Document5 pagesPex 06 01Elvis Nor FitrianaNo ratings yet
- Mitral StenosisDocument48 pagesMitral StenosiskornbergwiNo ratings yet
- Ninja - Antiarrhythmic Drugs PDFDocument7 pagesNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- Pulse OximeterDocument17 pagesPulse OximeterΑнмєɒ FσυαɒNo ratings yet
- Bedside MonitorDocument6 pagesBedside Monitoranggi fianitaNo ratings yet
- ECG Interpretation BookDocument57 pagesECG Interpretation BookLouis Plan100% (2)
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- DeVega TV RepairDocument8 pagesDeVega TV Repairndang01No ratings yet
- BCLS Practice MCQ StudentsDocument14 pagesBCLS Practice MCQ StudentsRaniNo ratings yet
- Jurnal Reading American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualityDocument17 pagesJurnal Reading American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualitydinageubrinaNo ratings yet