You might also like
- Cardiac Electrophysiology Board Review and Self-AssessmentDocument335 pagesCardiac Electrophysiology Board Review and Self-AssessmentAndonis AngelovNo ratings yet
- Acls Study GuideDocument24 pagesAcls Study GuideMohammad Gita100% (17)
- Manual of Pediatric Cardiac Intensive CareDocument326 pagesManual of Pediatric Cardiac Intensive CareLeydi Baltazar T100% (4)
- Atlas of Critical Care EchocardiographyDocument189 pagesAtlas of Critical Care EchocardiographyLara Abu LailaNo ratings yet
- Internal Medicine Case Write Up 1Document16 pagesInternal Medicine Case Write Up 1Shafiah Aqilah Mohd Jamal67% (3)
- Present-Tratamentul in DislipidemieDocument52 pagesPresent-Tratamentul in DislipidemieAdina BrahaNo ratings yet
- MCQS Pathology, Rawalpindi Medical CollegeDocument8 pagesMCQS Pathology, Rawalpindi Medical CollegeZahid QamarNo ratings yet
- Epigenetics (Nilofer Saba Azad, M.D.)Document40 pagesEpigenetics (Nilofer Saba Azad, M.D.)National Press Foundation100% (1)
- Hemodynamic MonitoringDocument23 pagesHemodynamic MonitoringIrvan SetiawanNo ratings yet
- Paradise TrialDocument26 pagesParadise TrialMiguel Martinez DuranNo ratings yet
- Statins in CVD Management: Is Just Lipid Lowering Enough?Document37 pagesStatins in CVD Management: Is Just Lipid Lowering Enough?SriNo ratings yet
- Atorvastatin Statin in CVD ManagementDocument37 pagesAtorvastatin Statin in CVD ManagementSriNo ratings yet
- Arni PPT 2 PDFDocument19 pagesArni PPT 2 PDFKumarsai Durusoju100% (1)
- Acute Respiratory Failure, Uncontrolled Diabetes, and Decompensated Heart FailureDocument9 pagesAcute Respiratory Failure, Uncontrolled Diabetes, and Decompensated Heart FailureAshok AgarwalNo ratings yet
- Management of Stroke Prevention in Atrial Fibrillation Patients with Multimorbid: Focus on Elderly and Renal ImpairmentDocument33 pagesManagement of Stroke Prevention in Atrial Fibrillation Patients with Multimorbid: Focus on Elderly and Renal ImpairmentSofia KusumadewiNo ratings yet
- CCO Madrid 2017 Highlights SlidesetDocument52 pagesCCO Madrid 2017 Highlights SlidesetAgustin Fau MaravillaNo ratings yet
- The Safety of COX-2 Inhibitors: A Review of Clinical Trial DataDocument29 pagesThe Safety of COX-2 Inhibitors: A Review of Clinical Trial DataHerry HendrayadiNo ratings yet
- Biomedik 3 Rational TherapyDocument51 pagesBiomedik 3 Rational TherapyMarissaMatinahoruNo ratings yet
- 3740s 01 GenelabsDocument129 pages3740s 01 GenelabsYulestrina WidiastutiNo ratings yet
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDocument65 pagesLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranNo ratings yet
- Presenter Conflict Disclosure SummaryDocument39 pagesPresenter Conflict Disclosure SummaryRirin ChandrikaNo ratings yet
- TWILIGHT DM AjitDocument21 pagesTWILIGHT DM Ajitajit jadhavNo ratings yet
- Ticagrelor Aspirin Stroke Study ResultsDocument2 pagesTicagrelor Aspirin Stroke Study ResultsDanny PhamNo ratings yet
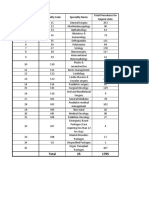
- Total Specialty Procedures GujaratDocument300 pagesTotal Specialty Procedures GujaratSumit Soni0% (1)
- ADVANCE-On EASD Study Rationale and DesignDocument26 pagesADVANCE-On EASD Study Rationale and Designmariatul fithriasariNo ratings yet
- Management of CAD: Role of Beta BlockerDocument89 pagesManagement of CAD: Role of Beta BlockerPragnesh ShahNo ratings yet
- 3740s 01 GenelabsDocument129 pages3740s 01 GenelabsIvan VeriswanNo ratings yet
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 pagesManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaNo ratings yet
- Alloon-Pump Assisted Oronary Ntervention Tudy: B C I SDocument24 pagesAlloon-Pump Assisted Oronary Ntervention Tudy: B C I SdoctordocsNo ratings yet
- 09.30 Professor John Townend, Chest Pain and Troponins On The Acute TakeDocument39 pages09.30 Professor John Townend, Chest Pain and Troponins On The Acute Takeamir ahmadNo ratings yet
- Beta Blockers: An Essential Therapy for Cardiovascular DiseaseDocument88 pagesBeta Blockers: An Essential Therapy for Cardiovascular DiseaseMostafa Hosny100% (1)
- DIABertelt2017 14Document7 pagesDIABertelt2017 14marsim92No ratings yet
- TRITON Anterior Depressions For AHADocument18 pagesTRITON Anterior Depressions For AHAyuda dwiNo ratings yet
- Clear PlateletsDocument17 pagesClear PlateletsJorge Peregrino BragaNo ratings yet
- Recent Advances in Management Of: Diabetic NephropathyDocument63 pagesRecent Advances in Management Of: Diabetic NephropathyA9 El-EbidiNo ratings yet
- Clinical Manifestations and Treatment Results of Patients With Cervical Cancer: A Report From IranDocument4 pagesClinical Manifestations and Treatment Results of Patients With Cervical Cancer: A Report From IranBayu Surya DanaNo ratings yet
- Project Presentation-Sydney StratfordDocument17 pagesProject Presentation-Sydney Stratfordapi-611918048No ratings yet
- Slides Del SitoDocument27 pagesSlides Del SitoNagatzulNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)Document26 pagesNonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)ROHITNo ratings yet
- Outcomes of SGLT2i in diabetic kidney disease: is it all diabetesDocument29 pagesOutcomes of SGLT2i in diabetic kidney disease: is it all diabetesVaibhav DafaleNo ratings yet
- TWILIGHTDocument24 pagesTWILIGHTRodrigo MartinNo ratings yet
- Recognition and Management of Toxicities: Faculty BiographyDocument35 pagesRecognition and Management of Toxicities: Faculty BiographyDaniela SerbanNo ratings yet
- Garrett Terhune SBP Ich Grand RoundsDocument31 pagesGarrett Terhune SBP Ich Grand Roundsapi-648757084No ratings yet
- Coronary Artery DiseaseDocument82 pagesCoronary Artery Diseasecortassa265No ratings yet
- DR MK Code Stroke in Pandemic EraDocument40 pagesDR MK Code Stroke in Pandemic EramayyamaharaniNo ratings yet
- Hospital Admission For Heart Failure: An Opportunity To Optimize Heart Failure Therapy?Document27 pagesHospital Admission For Heart Failure: An Opportunity To Optimize Heart Failure Therapy?juloc34No ratings yet
- Oppligerleibundgut 2012Document5 pagesOppligerleibundgut 2012HEARTJUGGLERNo ratings yet
- The Biology of Chronic Fatigue SyndromeDocument46 pagesThe Biology of Chronic Fatigue SyndromeAgustinus Benediktus Danang PutroNo ratings yet
- Dr-Rarsari - ARNI The New ParadigmDocument25 pagesDr-Rarsari - ARNI The New ParadigmBintang UbamnataNo ratings yet
- Cerebrovascular Diseases: Global Burden and Prevention StrategiesDocument28 pagesCerebrovascular Diseases: Global Burden and Prevention StrategiesbagussofianNo ratings yet
- AsundexianDocument25 pagesAsundexianshahane musayelyanNo ratings yet
- Dr. Azhari Gani, SpPD-KKV. FCIC - finaSIM - Rivaroxaban-Lesson Learned From EINSTEIN Revisi 1Document20 pagesDr. Azhari Gani, SpPD-KKV. FCIC - finaSIM - Rivaroxaban-Lesson Learned From EINSTEIN Revisi 1Yudi SfNo ratings yet
- Department of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoDocument1 pageDepartment of Haematology - : Mr. Nagaraja N 72yr 0Mth 3days Male Uhid Sin /LRN W/Bno/RefnoPrashanth NNo ratings yet
- Control Clinical TrialDocument14 pagesControl Clinical TrialNeha SinghNo ratings yet
- Dangas 2014 DiabetesDocument9 pagesDangas 2014 Diabetesmoroni.cayseNo ratings yet
- CCO Cytokine TX in MM ExpressPointsDocument18 pagesCCO Cytokine TX in MM ExpressPointsveaceslav coscodanNo ratings yet
- Pediatric LeukemiasDocument42 pagesPediatric LeukemiasslyfoxkittyNo ratings yet
- 2022 ESMO V AC Prostate Cancer Metastatic Hormone Sensitive Prostate Cancer FSDocument23 pages2022 ESMO V AC Prostate Cancer Metastatic Hormone Sensitive Prostate Cancer FScatp38647No ratings yet
- Predictors of Prognosis in Patients With Peripartum CardiomyopathyDocument4 pagesPredictors of Prognosis in Patients With Peripartum CardiomyopathynatayaregizaNo ratings yet
- 10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHADocument32 pages10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHAEmdan SengadjiNo ratings yet
- J Amjcard 2012 02 043Document5 pagesJ Amjcard 2012 02 043Efe Ge KaNo ratings yet
- William C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupDocument24 pagesWilliam C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupCardiologyNetwork.comNo ratings yet
- Arrhythmia risks after thrombolytic therapyDocument5 pagesArrhythmia risks after thrombolytic therapyTaniaNo ratings yet
- RidkerJUPITERslides - MPT - sld1Document12 pagesRidkerJUPITERslides - MPT - sld1Nawel BenNo ratings yet
- The Results of The Study of Heart and Renal Protection (SHARP)Document19 pagesThe Results of The Study of Heart and Renal Protection (SHARP)Surya MahardikaNo ratings yet
- 3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CDocument65 pages3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CAlexa GoteraNo ratings yet
- Anesthesia Considerations During Cytoreductive SurDocument9 pagesAnesthesia Considerations During Cytoreductive Surdrardigustian2986No ratings yet
- Effects of Ions on Heart Rate LabDocument5 pagesEffects of Ions on Heart Rate LabOkta Besti ArdikaNo ratings yet
- Resistant HypertensionDocument44 pagesResistant HypertensionKok Hui DiongNo ratings yet
- Cardiovascular System DiseaseDocument27 pagesCardiovascular System DiseasemarestelbaguiocajesNo ratings yet
- Reflection Paper On Anatomy and Physiology of HeartDocument7 pagesReflection Paper On Anatomy and Physiology of HeartSheryhan Tahir BayleNo ratings yet
- Maret 2021Document36 pagesMaret 2021Muhammad Pahlan PiruzziNo ratings yet
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- PO Adult-10-: Monitor ECG Periodically Prolonged TherapyDocument1 pagePO Adult-10-: Monitor ECG Periodically Prolonged Therapygeorgeloto12No ratings yet
- Cardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainDocument2 pagesCardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainDeepbluexNo ratings yet
- The Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityDocument10 pagesThe Impact of Coffee Subtypes On Incident Cardiovascular Disease, Arrhythmias, and MortalityJenny RojoNo ratings yet
- Acute Coronary SyndromeDocument30 pagesAcute Coronary SyndromeEndar EszterNo ratings yet
- Pharmaceutical care for hypertension patients to improve quality of lifeDocument55 pagesPharmaceutical care for hypertension patients to improve quality of lifeREYNER AURELINUS MAXIMUS 2018No ratings yet
- Functional and Structural Effects of Percutaneous Edge-To-edge Double-Orifice Repair Under Cardiac Cycle in Comparison With Suture RepairDocument13 pagesFunctional and Structural Effects of Percutaneous Edge-To-edge Double-Orifice Repair Under Cardiac Cycle in Comparison With Suture RepairhanNo ratings yet
- Oxy CadDocument21 pagesOxy CadrlinaoNo ratings yet
- 3 - Vascualr DisordersDocument7 pages3 - Vascualr DisordersKatelinne DabucolNo ratings yet
- ACLS-Study-Guide-2011 MADE EASYDocument2 pagesACLS-Study-Guide-2011 MADE EASYFrances Albaña TevesNo ratings yet
- Pdii Bipedal EdemaDocument5 pagesPdii Bipedal EdemacarlosNo ratings yet
- Patent Ductus ArteriosusDocument49 pagesPatent Ductus Arteriosusarchana vermaNo ratings yet
- Vital Signs/'Document30 pagesVital Signs/'Monika MinhasNo ratings yet
- Left Posterior Fascicular BlockDocument4 pagesLeft Posterior Fascicular BlockFathimah afifah zahrahNo ratings yet
- CBD Dr. Saugi - Robby GunawanDocument159 pagesCBD Dr. Saugi - Robby GunawanRobby GumawanNo ratings yet
- Cardiothoracic SurgeryDocument24 pagesCardiothoracic SurgeryMARTINNo ratings yet