You might also like
- Design and Finite Element-Based Fatigue Prediction of A New Self-Expandable Percutaneous Mitral Valve StentDocument6 pagesDesign and Finite Element-Based Fatigue Prediction of A New Self-Expandable Percutaneous Mitral Valve StenthanNo ratings yet
- PIIS0022522311007525Document10 pagesPIIS0022522311007525Enrico SquiccimarroNo ratings yet
- Minimally Invasive Mitral Valve Surgery: "The Leipzig Experience"Document7 pagesMinimally Invasive Mitral Valve Surgery: "The Leipzig Experience"Enrico SquiccimarroNo ratings yet
- Mitral Annular CalcificationDocument8 pagesMitral Annular CalcificationJiawei ZhouNo ratings yet
- 2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryDocument11 pages2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryOmán P. Jiménez A.No ratings yet
- Planning For Minimally Invasive Aortic Valve Replacement - Key Steps For Patient AssessmentDocument6 pagesPlanning For Minimally Invasive Aortic Valve Replacement - Key Steps For Patient AssessmentlkulacogluNo ratings yet
- A Novel User-Friendly Transcatheter Edge-To-Edge Mitral Valve Repair Device in A Porcine ModelDocument7 pagesA Novel User-Friendly Transcatheter Edge-To-Edge Mitral Valve Repair Device in A Porcine ModelEdson CarneiroNo ratings yet
- A Narrative Review About Technology and Desing of PICCs 1618312743Document3 pagesA Narrative Review About Technology and Desing of PICCs 1618312743Raquel CechinelNo ratings yet
- Folliguet 2009Document10 pagesFolliguet 2009CIRUGIA CARDIOTORÁCICA MINIMAMENTE INVASIVANo ratings yet
- 10 1093icvtsivy076Document9 pages10 1093icvtsivy076mukhlis akmalNo ratings yet
- Bankart repair versus open Latarjet procedure for recurrent shoulder dislocationDocument9 pagesBankart repair versus open Latarjet procedure for recurrent shoulder dislocationmarcelogascon.oNo ratings yet
- Oup Accepted Manuscript 2020Document7 pagesOup Accepted Manuscript 2020Enrico SquiccimarroNo ratings yet
- ANSYS Fluent - CFD Software PDFDocument3 pagesANSYS Fluent - CFD Software PDFSafi AhmedNo ratings yet
- 2022 Article 1790Document7 pages2022 Article 1790juajimenez55No ratings yet
- Keys to Successful Orthotopic Bladder SubstitutionFrom EverandKeys to Successful Orthotopic Bladder SubstitutionUrs E. StuderNo ratings yet
- 43044_2022_Article_298Document11 pages43044_2022_Article_298Faradiba MaricarNo ratings yet
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- Heart Valve Scaffold Fabrication - Bioinspired Control of Macro-Scale Morphology, Mechanics and Micro-Structure PDFDocument13 pagesHeart Valve Scaffold Fabrication - Bioinspired Control of Macro-Scale Morphology, Mechanics and Micro-Structure PDFMarcio AlfeoNo ratings yet
- Mitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsDocument7 pagesMitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsEnrico SquiccimarroNo ratings yet
- Clark 1998Document10 pagesClark 1998Yordhanno Xavier Fallaque RuizNo ratings yet
- Improvement in Coronary Anastomosis WitDocument6 pagesImprovement in Coronary Anastomosis WitTerymar SthefannyNo ratings yet
- Design and Material Optimization VentilatorDocument8 pagesDesign and Material Optimization VentilatorHadhi Hassan KhanNo ratings yet
- European J of Heart Fail - 2017 - Swol - Tracheostomy As A Bridge To Spontaneous Breathing and Awake ECMO in Non TransplantDocument4 pagesEuropean J of Heart Fail - 2017 - Swol - Tracheostomy As A Bridge To Spontaneous Breathing and Awake ECMO in Non Transplantjorge escobar pintoNo ratings yet
- Comparing Effects of Columellar Strut vs Septal Extension Grafts for Tip Support in RhinoplastyDocument8 pagesComparing Effects of Columellar Strut vs Septal Extension Grafts for Tip Support in RhinoplastyDanielBallesterosNo ratings yet
- The CathPilot A Novel Approach For Accurate Interventional Device Steering and TrackingDocument12 pagesThe CathPilot A Novel Approach For Accurate Interventional Device Steering and TrackingAnand Kumar MishraNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Evidence-Based Concepts and Procedures For Bonded Inlays and Onlays. Part III. A Case Series With Long-Term Clinical Results and Follow-UpDocument17 pagesEvidence-Based Concepts and Procedures For Bonded Inlays and Onlays. Part III. A Case Series With Long-Term Clinical Results and Follow-UpCamilo SestoNo ratings yet
- Finite Element Simulation of Mechanical Behaviors of Coronary Stent in A Vessel With PlaqueDocument9 pagesFinite Element Simulation of Mechanical Behaviors of Coronary Stent in A Vessel With PlaqueSALMA MOHIENo ratings yet
- Flow DiversionDocument13 pagesFlow Diversiondhaval thakkarNo ratings yet
- Clinical Effects of Pleurotomy On Patients Undergoing CABGDocument5 pagesClinical Effects of Pleurotomy On Patients Undergoing CABGBeshoy KhelaNo ratings yet
- FDP AvulsionDocument8 pagesFDP AvulsionNico BrantesNo ratings yet
- J Wneu 2019 05 148Document11 pagesJ Wneu 2019 05 148Cristian OñateNo ratings yet
- Proximal Anterolateral Accessory Portal Use Improves Peripheral Compartment Access and Capsular Management With T-CapsulotomyDocument5 pagesProximal Anterolateral Accessory Portal Use Improves Peripheral Compartment Access and Capsular Management With T-CapsulotomyMoustafa MohamedNo ratings yet
- Cost-Utility Analysis: Sartorius Flap Versus Negative Pressure Therapy For Infected Vascular Groin Graft ManagmentDocument11 pagesCost-Utility Analysis: Sartorius Flap Versus Negative Pressure Therapy For Infected Vascular Groin Graft ManagmentamdreyNo ratings yet
- Vitrectomy Surgery For Primary Retinal DetachmentDocument8 pagesVitrectomy Surgery For Primary Retinal DetachmentAvluz AdiansuhNo ratings yet
- Thin-Film Nitinol (Niti) : A Feasibility Study For A Novel Aortic Stent Graft MaterialDocument6 pagesThin-Film Nitinol (Niti) : A Feasibility Study For A Novel Aortic Stent Graft MaterialPaulNo ratings yet
- Reuse Cateter SafeDocument2 pagesReuse Cateter Safegadhang dewanggaNo ratings yet
- Pulsatile Flow Pump Based On An Iterative Controlled Piston PumpDocument7 pagesPulsatile Flow Pump Based On An Iterative Controlled Piston Pumpyue jiangNo ratings yet
- Repair CDLDocument6 pagesRepair CDLYuliastuti Mamah ChelseaNo ratings yet
- Aesculap Ds Appendectomy ClipDocument12 pagesAesculap Ds Appendectomy ClipdoniNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Finite Bukala 4 2014Document9 pagesFinite Bukala 4 2014alexis jonathanNo ratings yet
- Transcatheter Mitral Valve Replacement Still A Long Way To Go!Document4 pagesTranscatheter Mitral Valve Replacement Still A Long Way To Go!hanNo ratings yet
- Immediate Loading in The Complete Edentulous Maxilla-A Clinical CaseDocument8 pagesImmediate Loading in The Complete Edentulous Maxilla-A Clinical CasePreecha PaijitrochanaNo ratings yet
- Materials Today: Proceedings: Jayant Giri, Niraj Kshirsagar, Aishwary WanjariDocument6 pagesMaterials Today: Proceedings: Jayant Giri, Niraj Kshirsagar, Aishwary WanjarianujNo ratings yet
- New Concepts in Transcatheter Mitral Valve ReplacementDocument210 pagesNew Concepts in Transcatheter Mitral Valve ReplacementhanNo ratings yet
- Novel Robotic Meshworm With Segment-Bending Anchoring for ColonoscopyDocument7 pagesNovel Robotic Meshworm With Segment-Bending Anchoring for ColonoscopyNguyen SyNo ratings yet
- Midterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?Document12 pagesMidterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?mony saNo ratings yet
- Mid Term Outcomes of Stentless Bio Bentall vs. David Reimplantation For Aortic Root ReplacementDocument8 pagesMid Term Outcomes of Stentless Bio Bentall vs. David Reimplantation For Aortic Root ReplacementStefanie MelisaNo ratings yet
- A Comparison of Electrothermal Bipolar Vessel Sealing System and Electrocautery in Selective Neck DissectionDocument4 pagesA Comparison of Electrothermal Bipolar Vessel Sealing System and Electrocautery in Selective Neck DissectionGöksel TurhalNo ratings yet
- Delta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesDocument4 pagesDelta Wiring Technique To Treat Bony Mallet Fracture Technique Description and Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patient-Specific Neurovascular Simulator For Evaluating The Performance of Medical Robots and InstrumensDocument6 pagesPatient-Specific Neurovascular Simulator For Evaluating The Performance of Medical Robots and Instrumenspatogol278No ratings yet
- 2019 Cortical Button Fixation Vs Interference Screw FixationDocument9 pages2019 Cortical Button Fixation Vs Interference Screw FixationFreddy Churata SuriNo ratings yet
- Journal of Cardiothoracic SurgeryDocument9 pagesJournal of Cardiothoracic SurgeryThanh BinhNo ratings yet
- Robotic Lobectomy Right Upper LobectomyDocument14 pagesRobotic Lobectomy Right Upper LobectomyalfonsoNo ratings yet
- Transcatheter Aortic Valve Implantation: Current Status and Future PerspectivesDocument13 pagesTranscatheter Aortic Valve Implantation: Current Status and Future Perspectivesخديجة عمرNo ratings yet
- 2021 Article 2310Document6 pages2021 Article 2310Catharina Berla BerlianaNo ratings yet
- 2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsDocument7 pages2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsMikiNo ratings yet
- Aparicio C. Periodontology 2000Document19 pagesAparicio C. Periodontology 2000Luis Alberto Carpio MorenoNo ratings yet
- Finite Element Analysis For Fatigue Behaviour of A Self-Expanding NitinolDocument10 pagesFinite Element Analysis For Fatigue Behaviour of A Self-Expanding NitinolhanNo ratings yet
- Fluid Dynamics Modeling and Sound Analysis of A Bileaflet MechaniDocument135 pagesFluid Dynamics Modeling and Sound Analysis of A Bileaflet MechanihanNo ratings yet
- New Concepts in Transcatheter Mitral Valve ReplacementDocument210 pagesNew Concepts in Transcatheter Mitral Valve ReplacementhanNo ratings yet
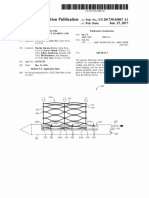
- Medtronic Vascular Patent US20170165067A1Document17 pagesMedtronic Vascular Patent US20170165067A1hanNo ratings yet
- Packaging Materials and Handling Technique: Dr. Ranjeet SinghDocument48 pagesPackaging Materials and Handling Technique: Dr. Ranjeet Singharon demagiba100% (1)
- Separation and Purification TechnologyDocument10 pagesSeparation and Purification TechnologyPedro Henrique MagachoNo ratings yet
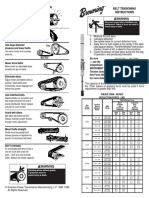
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- Maersk QuestionnaireDocument43 pagesMaersk QuestionnaireSahil SharmaNo ratings yet
- Aircraft Control Systems, Basic Construction, Wing and Fuselage ConstructionDocument146 pagesAircraft Control Systems, Basic Construction, Wing and Fuselage ConstructionTAMILSELVAM NALLUSAMYNo ratings yet
- ConvergeDocument22 pagesConvergekharynconvergeboholNo ratings yet
- Ahmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaDocument9 pagesAhmed Ali Alshehri Mobile 00966-508-217284 Address: P.O.Box 70132 Zipcode:31952 Riyadh Street, Al-Khobar, Saudi ArabiaShah KhalidNo ratings yet
- Blackmer Pump Parts ListDocument2 pagesBlackmer Pump Parts ListFelipe Ignacio PaillavilNo ratings yet
- Tugas Bahasa Inggris-1Document8 pagesTugas Bahasa Inggris-1Nur KomariyahNo ratings yet
- ISO 14000 - WikipediaDocument5 pagesISO 14000 - WikipediaalexokorieNo ratings yet
- Catalogo Tecnico Gb-S v07Document29 pagesCatalogo Tecnico Gb-S v07farou9 bmzNo ratings yet
- Slovakia C1 TestDocument7 pagesSlovakia C1 TestĐăng LêNo ratings yet
- Anatomy of A Plated HoleDocument5 pagesAnatomy of A Plated Holepbs0707No ratings yet
- Solar Collectors Final WordDocument14 pagesSolar Collectors Final WordVaibhav Vithoba NaikNo ratings yet
- FV10 Excel Flux Tutorial en 2Document36 pagesFV10 Excel Flux Tutorial en 2Ahcene BouzidaNo ratings yet
- GSL DIP Phase - 1 Cooler 45kWDocument1 pageGSL DIP Phase - 1 Cooler 45kWMuhasin PallikkalNo ratings yet
- Example of Gcse Science CourseworkDocument7 pagesExample of Gcse Science Courseworkbcrbcw6a100% (2)
- Changing Landscape and Ecotourism Development in A Large Dam SiteDocument16 pagesChanging Landscape and Ecotourism Development in A Large Dam Siteವಿನಯ್ ಎಮ್. ಆರ್No ratings yet
- The Practical Welding EngineerDocument154 pagesThe Practical Welding EngineerMohamed Atef0% (1)
- Fundamental Calculations To Convert Intensities Into Concentrations in Optical Emission Spectrochemical AnalysisDocument14 pagesFundamental Calculations To Convert Intensities Into Concentrations in Optical Emission Spectrochemical AnalysisPYDNo ratings yet
- The Affinity Laws of Centrifugal PumpsDocument5 pagesThe Affinity Laws of Centrifugal Pumpssba98No ratings yet
- Final Nasir GlassDocument57 pagesFinal Nasir GlassShuvo Taufiq Ahmed100% (2)
- Chapter 1 and 2Document67 pagesChapter 1 and 2Tle SupawidNo ratings yet
- Autocad Lab ManualDocument84 pagesAutocad Lab ManualRaghu RamNo ratings yet
- Estimation of Fabric Opacity by ScannerDocument7 pagesEstimation of Fabric Opacity by ScannerJatiKrismanadiNo ratings yet
- Eric Gamalinda - Amigo WarfareDocument88 pagesEric Gamalinda - Amigo Warfareenstone100% (1)
- TCB E-F 015cukDocument2 pagesTCB E-F 015cukTempcoNo ratings yet
- Friends of Hursley School: Late Summer NewsletterDocument6 pagesFriends of Hursley School: Late Summer Newsletterapi-25947758No ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- Guide 111: International Electrotechnical CommissionDocument7 pagesGuide 111: International Electrotechnical CommissionSayyid JifriNo ratings yet