You might also like
- The SAGES Manual of Robotic SurgeryFrom EverandThe SAGES Manual of Robotic SurgeryAnkit D. PatelNo ratings yet
- Residual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentFrom EverandResidual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentNo ratings yet
- 10.1186@s12891 020 03579 6Document6 pages10.1186@s12891 020 03579 6Han's OfficialNo ratings yet
- Bmri2021 5018791Document15 pagesBmri2021 5018791OstazNo ratings yet
- Technology in ArthroplastyDocument10 pagesTechnology in Arthroplastybá anh ngôNo ratings yet
- Damme Rer 2021Document10 pagesDamme Rer 2021son leNo ratings yet
- CT Terminology LexiconDocument12 pagesCT Terminology LexiconjtbushbergNo ratings yet
- Jain 2013Document15 pagesJain 2013Mohan DesaiNo ratings yet
- Hamilton 2014Document1 pageHamilton 2014DavidBeatonComuladaNo ratings yet
- Training Safer Orthopedic SurgeonsDocument6 pagesTraining Safer Orthopedic SurgeonsDania ZaidNo ratings yet
- ACL Tibial Fixation MedthodsDocument8 pagesACL Tibial Fixation MedthodsCleff FlowersNo ratings yet
- Artificial Intelligence and Machine Learning On Diagnosis and Classification of Hip Fracture: Systematic ReviewDocument13 pagesArtificial Intelligence and Machine Learning On Diagnosis and Classification of Hip Fracture: Systematic ReviewMEHDI JAHANIRADNo ratings yet
- Complications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic ReviewDocument15 pagesComplications and Downsides of The Robotic Total Knee Arthroplasty: A Systematic Reviewmamyeu1801No ratings yet
- The Accuracy of Digital Templating in Uncemented Total Hip ArthroplastyDocument6 pagesThe Accuracy of Digital Templating in Uncemented Total Hip Arthroplastyson leNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Robotic-Assisted Versus Laparoscopic Cholecystectomy: Outcome and Cost Analyses of A Case-Matched Control StudyDocument7 pagesRobotic-Assisted Versus Laparoscopic Cholecystectomy: Outcome and Cost Analyses of A Case-Matched Control StudyAndrei GheorghitaNo ratings yet
- An Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTDocument9 pagesAn Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTBounegta AhmedNo ratings yet
- Igrt ThesisDocument8 pagesIgrt Thesislisanetkowiczerie100% (1)
- Ghid Plex Brahial Conturaj PDFDocument7 pagesGhid Plex Brahial Conturaj PDFMiruna MafteiNo ratings yet
- ContohDocument9 pagesContohVino DoangNo ratings yet
- Robotic Assistance For Ultrasound Guided Prostate BrachytherapyDocument9 pagesRobotic Assistance For Ultrasound Guided Prostate Brachytherapykk_kamalakkannanNo ratings yet
- s13018 018 0814 1Document9 pagess13018 018 0814 1Someshwar GuptNo ratings yet
- Cone Beam CT Literature ReviewDocument6 pagesCone Beam CT Literature Reviewm1dyhuh1jud2100% (1)
- Uncemented, Curved, Short Endoprosthesis Stem For Distal Femoral Reconstruction: Early Follow-Up OutcomesDocument11 pagesUncemented, Curved, Short Endoprosthesis Stem For Distal Femoral Reconstruction: Early Follow-Up Outcomesyerich septaNo ratings yet
- A Literature Review On Pneumatic Operated CPM Machine For Knee and AnkleDocument5 pagesA Literature Review On Pneumatic Operated CPM Machine For Knee and AnkleIJRASETPublicationsNo ratings yet
- 意大利2018 共识声明:同种异体移植物在前交叉韧带重建术中的应用Document9 pages意大利2018 共识声明:同种异体移植物在前交叉韧带重建术中的应用Roger PanNo ratings yet
- CH 05Document8 pagesCH 05Omkar KongariNo ratings yet
- 2018 Preoperative CT-Based Three-Dimensional Templating in Robot-Assisted Total Knee Arthroplasty More Accurately Predicts Implant Sizes Than Two-Dimensional TemplatingDocument7 pages2018 Preoperative CT-Based Three-Dimensional Templating in Robot-Assisted Total Knee Arthroplasty More Accurately Predicts Implant Sizes Than Two-Dimensional Templatingsumon.huqNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- Patient Specific Implants: Scope For The Future: Tka Symposium (P Sancheti, Section Editor)Document6 pagesPatient Specific Implants: Scope For The Future: Tka Symposium (P Sancheti, Section Editor)NILADRI ACHARYYANo ratings yet
- ArthroscopesDocument5 pagesArthroscopesCRISTY YAHIDIBI FARRUFIA RENTERIANo ratings yet
- Comparison of Total Patellectomy and Osteosynthesis With Tension Band WiringDocument11 pagesComparison of Total Patellectomy and Osteosynthesis With Tension Band WiringAldrovando JrNo ratings yet
- Ultrasound Machine Research PaperDocument5 pagesUltrasound Machine Research Paperpukytij0wyg3100% (1)
- TAC en traumaDocument9 pagesTAC en traumasamuelfdiaz.0103No ratings yet
- Pi is 0883540322007379Document6 pagesPi is 0883540322007379Debangshu KumarNo ratings yet
- Use of Computer Navigation in Orthopedic OncologyDocument8 pagesUse of Computer Navigation in Orthopedic OncologyFrontiersNo ratings yet
- CJRT 51 69Document3 pagesCJRT 51 69api-354040213No ratings yet
- Analysis of Total Knee Arthroplasty Revision Causes: Researcharticle Open AccessDocument6 pagesAnalysis of Total Knee Arthroplasty Revision Causes: Researcharticle Open AccessCláudia SilvaNo ratings yet
- Computer Technology Applications in Surgical Implant Dentistry: A Systematic ReviewDocument18 pagesComputer Technology Applications in Surgical Implant Dentistry: A Systematic ReviewsujeetNo ratings yet
- 10.1007@s00167 020 05997 4Document7 pages10.1007@s00167 020 05997 4Residentes TyONo ratings yet
- Final DraftDocument18 pagesFinal Draftapi-334402872No ratings yet
- Reliability of virtual implant planningDocument5 pagesReliability of virtual implant planningBlas García GarcíaNo ratings yet
- Cost and Safety Evaluation of Simultaneous Bilateral Total Knee Arthroplasty Versus Unilateral KneeDocument5 pagesCost and Safety Evaluation of Simultaneous Bilateral Total Knee Arthroplasty Versus Unilateral KneeazevedoNo ratings yet
- Total Ankle Replacement Surgery (Arthroplasty)Document12 pagesTotal Ankle Replacement Surgery (Arthroplasty)ashut1No ratings yet
- Implementation of Modern Technologies in Total Knee ReplacementDocument4 pagesImplementation of Modern Technologies in Total Knee ReplacementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ICS Guidelines on Urodynamic Equipment PerformanceDocument10 pagesICS Guidelines on Urodynamic Equipment PerformanceJuan Sebastian Martinez OvalleNo ratings yet
- Quality Assurance For Image-Guided Radiation Therapy Utilizing CT-basedDocument18 pagesQuality Assurance For Image-Guided Radiation Therapy Utilizing CT-based2016508吳翊晨No ratings yet
- Three-Dimensional Computerized Orthognathic Surgical Treatment PlanningDocument10 pagesThree-Dimensional Computerized Orthognathic Surgical Treatment PlanningRajan KarmakarNo ratings yet
- JRM-CC: Clinical CommunicationsDocument7 pagesJRM-CC: Clinical CommunicationsOstazNo ratings yet
- The Open Orthopaedics JournalDocument7 pagesThe Open Orthopaedics JournalhuynhkimhieuNo ratings yet
- The CT Handbook Optimizing Protocols For Today's Feature Rich Scanners Chapter 1Document35 pagesThe CT Handbook Optimizing Protocols For Today's Feature Rich Scanners Chapter 1Abdullah AliNo ratings yet
- Measurements of Computed Tomography Dose Index For Axial and Spiral CT ScannersDocument7 pagesMeasurements of Computed Tomography Dose Index For Axial and Spiral CT ScannersSaikat NandyNo ratings yet
- Comparison of Isocentric C-Arm 3-DimensionaDocument7 pagesComparison of Isocentric C-Arm 3-Dimensionagevowo3277No ratings yet
- Totalsegmentator: Robust Segmentation of 104 Anatomical Structures in CT ImagesDocument44 pagesTotalsegmentator: Robust Segmentation of 104 Anatomical Structures in CT ImagesanhtainguyenluuNo ratings yet
- The Accuracy of Implant Placement With Computer-GuidedDocument11 pagesThe Accuracy of Implant Placement With Computer-GuidedRyan Ardi PradanaNo ratings yet
- Korir 2015Document11 pagesKorir 2015Rimo RimoNo ratings yet
- Total Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueDocument9 pagesTotal Knee Replacement Modifies The Preoperative Tibial Torsion Angle - Similar Results Between Computer-Assisted and Standard TechniqueJoko TriwardonoNo ratings yet
- Immobilisation FFFDocument8 pagesImmobilisation FFFSrinivas VenkataramanNo ratings yet
- Redesign of A Continuous Passive Motion Machine For Total Knee Replacement TherapyDocument13 pagesRedesign of A Continuous Passive Motion Machine For Total Knee Replacement TherapyAdi CrişanNo ratings yet
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- Water Treatment PDFDocument87 pagesWater Treatment PDFJubin KumarNo ratings yet
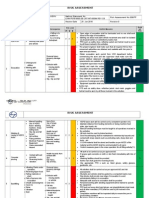
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
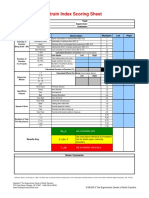
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- Pathology of the EndocardiumDocument31 pagesPathology of the EndocardiumAlexe VladNo ratings yet
- 50 Human Studies Identify High Risks of Prenatal Ultrasound - The Healthy Home EconomistDocument26 pages50 Human Studies Identify High Risks of Prenatal Ultrasound - The Healthy Home EconomistkromotNo ratings yet
- Psychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyDocument69 pagesPsychopathic Personality: Bridging The Gap Between Scientific Evidence and Public PolicyGokushimakNo ratings yet
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDocument75 pagesU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10No ratings yet
- Acute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010Document24 pagesAcute Respiratory Distress Syndrome: Jason D. Sciarretta, M.D. Critical Care Conference October 13, 2010JelenaNo ratings yet
- Amway ProductDocument9 pagesAmway ProductAbu Sayed Md. RashedNo ratings yet
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniNo ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Can Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.Document15 pagesCan Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.ALIXNo ratings yet
- Leni Robredo CredentialsDocument2 pagesLeni Robredo CredentialsJhelliene Rose V. De CastroNo ratings yet
- (Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioDocument455 pages(Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioEsteban Gonzàlez RodriguezNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet
- Cricket Academy Head Coach RoleDocument4 pagesCricket Academy Head Coach Roletauseef1716No ratings yet
- Musculoskeletal Physical TherapyDocument5 pagesMusculoskeletal Physical TherapyAbiha AnisNo ratings yet
- Hum. Reprod.-1999-Tesarik-1318-23Document6 pagesHum. Reprod.-1999-Tesarik-1318-23Meilana Sapta DNo ratings yet
- Neem by Ellen NortenDocument100 pagesNeem by Ellen NortenMano DrabuzeliaiNo ratings yet
- City of Peterborough 2023 Draft Capital BudgetDocument535 pagesCity of Peterborough 2023 Draft Capital BudgetPeterborough ExaminerNo ratings yet
- BlsDocument62 pagesBlspaediatrica89% (19)
- The30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Document17 pagesThe30 Itemand15 itemBostonnamingtestCzechBezdiceketal.2022Alexander OrzocoNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet
- Pulmonary TB RadiologyDocument45 pagesPulmonary TB RadiologyArina Windri RivartiNo ratings yet
- IELTS-Style Speaking Test Questions and Answers SportDocument4 pagesIELTS-Style Speaking Test Questions and Answers SportĐại Học Ôn ThiNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet