Professional Documents
Culture Documents
Looker 2017
Uploaded by
Zakia DrajatCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Looker 2017
Uploaded by
Zakia DrajatCopyright:
Available Formats
Articles
Effect of HSV-2 infection on subsequent HIV acquisition:
an updated systematic review and meta-analysis
Katharine J Looker*, Jocelyn A R Elmes*, Sami L Gottlieb, Joshua T Schiffer, Peter Vickerman, Katherine M E Turner, Marie-Claude Boily
Summary
Background HIV and herpes simplex virus type 2 (HSV-2) infections cause a substantial global disease burden and are Lancet Infect Dis 2017
epidemiologically correlated. Two previous systematic reviews of the association between HSV-2 and HIV found Published Online
evidence that HSV-2 infection increases the risk of HIV acquisition, but these reviews are now more than a decade old. August 23, 2017
http://dx.doi.org/10.1016/
S1473-3099(17)30405-X
Methods For this systematic review and meta-analysis, we searched PubMed, MEDLINE, and Embase (from Jan 1, 2003,
See Online/Comment
to May 25, 2017) to identify studies investigating the risk of HIV acquisition after exposure to HSV-2 infection, either http://dx.doi.org/10.1016/
at baseline (prevalent HSV-2 infection) or during follow-up (incident HSV-2 infection). Studies were included if they S1473-3099(17)30493-0
were a cohort study, controlled trial, or case-control study (including case-control studies nested within a cohort study *Joint first authors
or clinical trial); if they assessed the effect of pre-existing HSV-2 infection on HIV acquisition; and if they determined School of Social and
the HSV-2 infection status of study participants with a type-specific assay. We calculated pooled random-effect Community Medicine
estimates of the association between prevalent or incident HSV-2 infection and HIV seroconversion. We also extended (K J Looker PhD,
Prof P Vickerman DPhil), and
previous investigations through detailed meta-regression and subgroup analyses. In particular, we investigated the Bristol Veterinary School
effect of sex and risk group (general population vs higher-risk populations) on the relative risk (RR) of HIV acquisition (K M E Turner PhD), University
after prevalent or incident HSV-2 infection. Higher-risk populations included female sex workers and their clients, of Bristol, Bristol, UK;
men who have sex with men, serodiscordant couples, and attendees of sexually transmitted infection clinics. Department of Infectious
Disease Epidemiology, Imperial
College London, London, UK
Findings We identified 57 longitudinal studies exploring the association between HSV-2 and HIV. HIV acquisition (J A R Elmes PhD,
was almost tripled in the presence of prevalent HSV-2 infection among general populations (adjusted RR 2·7, 95% CI Prof M-C Boily PhD);
2·2–3·4; number of estimates [Ne]=22) and was roughly doubled among higher-risk populations (1·7, 1·4–2·1; Department of Reproductive
Health and Research, World
Ne=25). Incident HSV-2 infection in general populations was associated with the highest risk of acquisition of HIV Health Organization, Geneva,
(4·7, 2·2–10·1; Ne=6). Adjustment for confounders at the study level was often incomplete but did not significantly Switzerland (S L Gottlieb MD);
affect the results. We found moderate heterogeneity across study estimates, which was explained by risk group, world Vaccine and Infectious Disease
region, and HSV-2 exposure type (prevalent vs incident). Division, and Clinical Research
Division, Fred Hutchinson
Cancer Research Center,
Interpretation We found evidence that HSV-2 infection increases the risk of HIV acquisition. This finding has Seattle, WA, USA
important implications for management of individuals diagnosed with HSV-2 infection, particularly for those who (J T Schiffer MD); and
Department of Medicine,
are newly infected. Interventions targeting HSV-2, such as new HSV vaccines, have the potential for additional benefit
University of Washington,
against HIV, which could be particularly powerful in regions with a high incidence of co-infection. Seattle, WA, USA (J T Schiffer)
Correspondence to:
Funding World Health Organization. Dr Katharine J Looker, School of
Social and Community Medicine,
Copyright This is an Open Access article published under the CC BY-NC-ND 3.0 IGO license which permits University of Bristol,
Bristol BS8 2BN, UK
unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any katharine.looker@bristol.ac.uk
use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services.
The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.
Introduction symptomatic, most transmissions are thought to occur
HIV and herpes simplex virus type 2 (HSV-2) are when the source partner is asymptomatic.4 Genital
two global health problems. In 2015, 36·7 million people HSV-2 infection can considerably affect relationships
were estimated to be living with HIV/AIDS globally.1 In through feelings of shame and stigma and concerns
2012, an estimated 417 million people aged 15–49 years about risk of transmission.5,6
had HSV-2 infection.2 70% of HIV infections are in HIV and HSV-2 are both lifelong sexually transmitted
sub-Saharan Africa, which also has the highest HSV-2 infections (STIs) that are associated with similar risk
prevalence.1,2 HSV-2 causes genital herpes, which, when factors (eg, age, sex, partner change rate, condom use,
symptomatic, is characterised by periodic recurrences male circumcision).7–10 Additionally, evidence exists of
of painful genital ulcers.3 Although genital herpes direct and reciprocal biological interactions between HIV
is asymptomatic or unrecognised in about 80–90% and HSV-2.11,12 Active HSV-2 infection, regardless of
of individuals, asymptomatic viral reactivation and symptoms, involves high concentrations of activated
shedding are common.3 Thus, although individuals CD4-positive T cells, which are target cells for HIV, in the
with HSV-2 are most infectious when they are genital area and can lead to breaks in the mucosal layer
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 1
Articles
Research in context
Evidence before this study HSV-2 infection and almost twice the risk associated with
Herpes simplex virus type 2 (HSV-2) and HIV are both lifelong exposure to prevalent HSV-2 infection. These findings provide a
infections sharing common risk factors and widely co-occur strong indication for a biological effect of HSV-2 infection on
geographically. Two meta-analytic systematic reviews of HIV, because the frequency and severity of genital ulceration,
longitudinal studies have been published to date and have viral shedding, and associated inflammation in the genital tract
shown the adjusted risk of HIV acquisition among individuals are highest in new HSV-2 infections and tend to decrease with
with prevalent HSV-2 infection to be two to three times the risk time after infection. The association was higher among general
in those without. This increased risk is thought to be caused by populations than among higher-risk populations. Study-level
the recruitment of activated CD4-positive T cells to the genital adjustment for confounders was often incomplete, but did not
area, which are target cells for HIV, and breaks in the protective meaningfully affect the association when comparing crude and
epithelial layer during active HSV-2 infection. However, the adjusted pooled estimates. Heterogeneity across study
most recent of these reviews is now more than a decade old and estimates was moderate. We extended previous reviews
only included 19 studies, limiting the scope for assessing the through detailed assessment of heterogeneity using
effect of heterogeneity and study quality. The substantial meta-regression and sub-pooling and through extensive
number of new studies published on the subject since then assessment of potential biases. We found limited evidence of
allows for more in-depth investigation, including, for the first publication bias.
time, quantification of the effect of exposure to incident in
Implications of all the available evidence
addition to prevalent HSV-2 infection on pooled estimates of
Our results provide evidence in support of a direct effect of
the association with HIV acquisition. For this systematic review
HSV-2 infection on HIV acquisition, which is strengthened by
and meta-analysis, we searched PubMed, MEDLINE, and
our finding of significantly higher HIV risk associated with
Embase between Jan 1, 2003, and May 25, 2017, for studies of
incident HSV-2 infection than with prevalent HSV-2 infection.
the association between incident or prevalent HSV-2 infection
At the population level, new interventions targeting HSV-2,
and HIV infection. Studies were included if they were a cohort
such as new vaccines or microbicides, could have an additional
study, controlled trial, or case-control study (including
indirect benefit on HIV as a consequence of the interactions
case-control studies nested within a cohort or controlled trial);
between HIV and HSV-2. Such synergies could greatly enhance
were designed to assess the effect of preceding HSV-2 infection
the effect of combination prevention for HIV infection,
on HIV acquisition; and used a type-specific antibody assay to
particularly in settings with high HIV prevalence. The
determine HSV-2 infection (serostatus). 57 longitudinal studies
magnitude of this public health benefit now needs to be
met our inclusion criteria, which was 38 more than the last
carefully estimated for different settings by use of
systematic search and review (by Freeman and colleagues).
mathematical models informed by the most recent evidence
Added value of this study of the associations between HSV and HIV.
We report that the pooled adjusted risk of HIV acquisition after
incident HSV-2 infection is almost five times the risk without
through which HIV can enter.13 Because genital ulceration therapy against HSV-2 have not shown reduced risk of
and viral shedding occur most frequently in the first year HIV acquisition or transmission,24–26 perhaps because
of HSV-2 infection,14–16 the increase in HIV susceptibility agents were not used at sufficient doses or for sufficient
might be highest for incident HSV-2 infections. Co- duration, new vaccines against HSV-2 that are currently
infection with HIV increases HSV-2 genital shedding and under development27 could hold more promise for HIV
transmissibility, while HSV-2 infection correlates with prevention.
increased HIV viraemia and transmissibility.17–20 Two systematic reviews and meta-analyses of the
Development of multipurpose prevention products association between HSV-2 infection and subsequent
that could protect against multiple STIs (eg, topical HIV acquisition have been done: one in 200212 and the
microbicides and oral pre-exposure prophylaxis) other in 200611 (the one in 2006 was briefly updated in
would provide exciting opportunities to simultaneously an editorial28). These reviews reported a two to three
reduce the burden of disease of more than one times increase in the risk of HIV infection with
infection.21–23 Quantifying the effect of HSV-2 infection baseline prevalent HSV-2 infection;11,12 estimates of the
on HIV acquisition has important public health association tended to be lower for high-risk populations
implications, particularly in high-prevalence settings than for low-risk populations. Here we update and
where co-infection is common, because prevention of substantially augment these reviews to modernise our
HSV-2 infection (with single-purpose or multipurpose understanding of the interaction between HSV-2
prevention tools) might indirectly prevent HIV infection. infection and HIV, in line with the pace of advancing
Although trials of use of daily suppressive antiviral prevention efforts against HSV-2 and HIV.
2 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
Methods Two authors (KJL and JARE) did the systematic review
Search strategy and selection criteria and meta-analysis, according to PRISMA29 and MOOSE30
For this systematic review and meta-analysis, we searched guidelines. Conflicts about inclusion were resolved
PubMed, MEDLINE, and Embase between Jan 1, 2003, through discussion between reviewers.
and May 25, 2017, to identify studies of the relative risk
(RR) of HIV acquisition after exposure to HSV-2 infection Data analysis
either at baseline (ie, prevalent infection) or during Based on previous evidence suggesting differential
follow-up (ie, incident infection), published since the susceptibility to HIV and HSV-2 by sex,7–9 after exposure
review by Freeman and colleagues.11 For PubMed, we to incident HSV-2 infection,14–16 and by risk behaviour,10
searched for articles and abstracts using the terms we defined a priori that our primary outcomes would be
(“HIV”, “human immunodeficiency virus”, “human pooled RR estimates of the association between incident
immunedeficiency virus”, “human immune deficiency HIV infection and pre-existing prevalent or incident
virus”, OR “human immuno deficiency virus”) AND HSV-2 infection, for both women and men and by risk
(“HSV”, “herpes simplex”, “herpes virus type 2”, “herpes group (general population vs higher-risk populations),
virus 2”, “herpesvirus 2”, “genital herpes” OR “herpes also allowing for comparisons with previous pooled
genitalis”). Articles in PubMed were also searched with estimates.11 Higher-risk populations included female sex
the Medical Subject Headings terms (“herpes simplex” workers and their clients, men who have sex with men,
OR “simplexvirus”) AND (“human immunodeficiency serodiscordant couples, and attendees of STI clinics. No
virus”, “HIV infection”, “HIV antibodies”, “HIV other stratification was used. To minimise biases due to
seronegativity”, OR “HIV seroprevalence”). We included reverse causation, pooled RR estimates for the association
studies if they were a cohort study, controlled trial, or between HIV infection and exposure to incident HSV-2
case-control study (including case-control studies nested infection were restricted to study estimates when HSV-2
within a cohort or controlled trial); were designed to seroconversion was definitely known to have occurred
assess the effect of preceding HSV-2 infection, compared before HIV seroconversion.
with HSV-2 negativity, on HIV acquisition (ie, excluding To assess study quality, we used the Newcastle-Ottawa
case-control studies based on samples from only one Scale31 to define nine criteria assessing selection of study
point in time and studies that only looked at the effect of participants, sample representativeness, exposure or
pre-existing HIV infection on HSV-2 acquisition); and outcome ascertainment, and confounding for the extracted
determined the HSV-2 infection status of study information about participant and study characteristics. A
participants with an antibody-type-specific assay. star was awarded for each predetermined criterion that was
Individuals were defined as HSV-2 negative (unexposed) met (appendix). This assessment was done at the estimate
if they remained HSV-2 seronegative throughout follow- level, not the study level. The effect of the number of stars
up (preferably) or were HSV-2 seronegative at baseline (for awarded and other measures of study quality related to
those studies in which HSV-2 testing was not done during study characteristics on RR estimates was subsequently
follow-up; repeat testing that was done but not reported explored with meta-regression and subgroup analyses.
was noted as a possible source of reporting bias for the We investigated the effect of heterogeneity across
subsequent assessment of study quality). For full details of independent RR estimates using the I² statistic.32 Sources
the search, selection criteria, and data extraction, see the of heterogeneity were explored with univariate
appendix. meta-regression analysis of independent adjusted RR See Online for appendix
For studies measuring incident HSV-2 infection, we estimates, which estimated the fraction of the between-
classified RR estimates of HIV acquisition after exposure to study variance in adjusted RR estimates (ie, R²) explained
incident HSV-2 infection into five subcategories for timing by participant characteristics (eg, world region), study
sequence. These subcategories reflected uncertainty in the characteristics (eg, study design), and study quality (eg,
exact timing of HSV-2 and HIV seroconversion: (1) HSV-2 number of Newcastle-Ottawa Scale stars). Multivariate
seroconversion was observed in a previous time interval meta-regression analysis was also done with estimates
and thus HSV-2 infection happened before HIV (definitely for exposure to prevalent HSV-2 infection, but not with
before); (2) HSV-2 seroconversion was observed in the estimates for exposure to incident HSV-2 infection
same time interval as HIV seroconversion and so HSV-2 because of the small number of estimates (Ne).
infection might have happened before or after HIV Additionally, we did separate subgroup analyses of
infection (indeterminably close); (3) HSV-2 seroconversion adjusted RR estimates for the incident and prevalent
was observed in a previous or in the same time interval as HSV-2 exposures (appendix).
HIV seroconversion (before and indeterminably close); Publication bias was assessed quantitatively at the
(4a) some HSV-2 seroconversion might have occurred after estimate level, not the study level, in two ways. First, we
HIV infection (maybe after and indeterminably close produced funnel plots33 and did Egger’s test for
or before); and (4b) some HSV-2 seroconversion was publication bias34 for both crude RR and adjusted
observed after HIV infection (after and indeterminably RR estimates and for exposure to prevalent compared
close or before; appendix). with exposure to incident HSV-2 infection (appendix).
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 3
Articles
HIV/AIDS (UNAIDS). SLG from WHO commissioned
6037 publications identified from PubMed, MEDLINE, and Embase the study, contributed to the direction of the work, and
commented on the drafts. KJL and JARE had full access
to all the data in the study and had final responsibility
1469 duplicate publications removed
for the decision to submit for publication.
4658 abstracts examined (or title if no abstract was available) Results
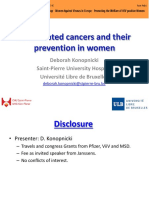
We identified 96 relevant publications from
57 independent studies in the systematic review (figure 1).
4191 non-relevant publications removed
54 studies reported on the RR of HIV acquisition after
exposure to prevalent HSV-2 infection and 28 studies
377 full-text articles retrieved for more detailed examination reported on the RR of HIV acquisition after exposure to
incident HSV-2 infection (table 1; appendix). More
studies reported on men than on women and on female
311 publications excluded on the basis of selection
criteria (including 2 papers not retrieved) sex workers, men who have sex with men, and other
higher-risk groups than on general populations (table 1).
30 additional relevant publications identified Most studies were done in Africa, in populations where
21 identified through searches of reference
lists
baseline HSV-2 prevalence was greater than 30%, and
9 identified from a previous systematic review were observational cohort studies with follow-up
8 identified from a parallel search* exceeding 1 year. Additionally, most studies tested for
HIV every 6 months or more frequently and defined the
96 publications from 57 studies investigated HIV incidence in unexposed group for exposure to prevalent HSV-2
HSV-2 seropositive versus HSV-2 seronegative individuals infection as participants who were HSV-2 (sero)negative
at baseline. Key potential confounders that were adjusted
2 studies not included in the analysis
for included age and sexual behaviour, while several
1 reported the significance of the association studies inappropriately adjusted for genital ulcer disease.
but no estimates 39 studies reported 55 adjusted RR estimates for our
1 investigated the association but did not
report any findings primary outcome: HIV acquisition after exposure to
prevalent or incident HSV-2 infection (timing of HSV-2
infection definitely before HIV infection) among general
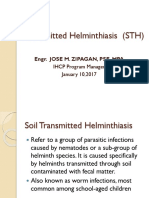
55 studies had available estimates for effect of prevalent or and higher-risk populations, by sex (figure 2). No significant
incident HSV-2 infection on HIV acquisition
differences were seen in the associations among general
populations by sex. The overall pooled adjusted RR for
Figure 1: Study selection general populations was 2·7 (95% CI 2·2–3·4; Ne=22;
*The search was done in parallel by two reviewers (KJL and JARE). The results for one reviewer are shown; the I²=59%) for exposure to prevalent HSV-2 infection and 4·7
results were very similar between the two reviewers. Each reviewer found eight publications to be relevant that the
other reviewer did not. HSV-2=herpes simplex virus type 2. (2·2–10·1; Ne=6; I²=64%) for exposure to incident HSV-2
infection. The results for higher-risk populations were
similar to those for general populations, but the magnitude
Second, we assessed with meta-regression analysis of the associations was lower: the overall pooled adjusted
whether crude RR estimates calculated from the available RR estimate for higher-risk populations was 1·7 (1·4–2·1;
data were less likely to be significant than those provided Ne=25; I²=45%) for exposure to prevalent HSV-2 infection
directly in the paper. Third, we qualitatively assessed and 2·9 (1·7–5·0; Ne=2; I²=0%) for exposure to incident
whether there was evidence of selective reporting of HSV-2 infection.
significant results. 50 studies reported on 64 crude RR estimates for our
All meta-analyses, meta-regressions, subgroup primary outcome (appendix). Pooled crude RR estimates
analyses, and forest plots were done with R version 3.2.2. overall and by sex were similar to pooled adjusted RR
We derived pooled RR estimates with natural log- estimates, although the pooled crude RR estimates for
transformed study estimates and SEs with random-effect exposure to incident HSV-2 infection were somewhat
models, based on the DerSimonian-Laird inverse- higher than the adjusted RR estimates for general
variance method,35 using the metafor package in R.36 populations and were lower than the adjusted RR
Pooled estimates were then back-transformed to the estimates for higher-risk populations. Crude estimates
original scale (further details in the appendix). were generally more heterogeneous than adjusted
estimates (figure 2; appendix).
Role of the funding source In the univariate meta-regression analysis of
This study was funded by WHO through the Unified 48 independent adjusted estimates (Ne=40 for prevalent
Budget, Results and Accountability Framework HSV-2 infection; Ne=8 for incident HSV-2 infection),
(UBRAF) from the Joint United Nations Programme on only risk group (higher-risk population vs general
4 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
Prevalent HSV-2 infection* Incident HSV-2 infection†
Number of Number of estimates Number of Number of estimates
studies (n=54) studies (n=28)
Crude RR Adjusted RR Crude RR Adjusted RR
Participant characteristics
Mean or median age‡§
≤25 years 15 18 17 10 9 12
>25 years 39 68 54 20 31 35
Not reported 2 4 1 1 1 0
Sex‡
All women 28 41 34 11 14 24
General population 11 17 15 4 10 13
Female sex workers 8 9 13 2 1 7
Other higher-risk populations¶ 10 15 6 5 3 4
All men 28 37 31 17 23 19
General population 10 14 18 6 11 13
Men who have sex with men 13 16 9 9 11 3
Other higher-risk populations|| 5 7 4 3 1 3
Women and men combined** 8 12 7 5 4 4
WHO region
Africa 35 64 56 16 27 38
Americas 8 11 5 5 7 3
Europe 1 1 0 1 1 0
Eastern Mediterranean 0 0 0 0 0 0
Southeast Asia 5 7 7 4 4 6
Western Pacific 4 4 2 2 2 0
World (not including Africa) 1 3 2 0 0 0
HSV-2 prevalence‡
≤30% 13 14 12 8 8 6
>30% 42 75 59 21 33 41
Not reported 1 1 1 0 0 0
Study characteristics
Study year (mid-point)‡
Pre-2000 16 31 32 11 20 20
2000 onwards 33 54 34 16 19 25
Not reported 6 5 6 2 2 2
Study design
Cohort 27 34 38 15 14 21
Case-control†† 7 8 4 6 7 2
Controlled trial 20 48 30 7 20 24
Study design for analysis of controlled trial data
Prospective 17 33 18 6 10 12
Nested case-control†† 3 15 12 2 10 12
Controlled trial intervention group‡
Intervention 6 8 2 1 2 2
Control 6 8 3 1 2 2
Combined 20 32 25 7 16 20
Overall number of participants for study‡
≤1000 31 49 36 13 23 15
>1000 24 41 36 16 18 32
(Table 1 continues on next page)
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 5
Articles
Prevalent HSV-2 infection* Incident HSV-2 infection†
Number of Number of estimates Number of Number of estimates
studies (n=54) studies (n=28)
Crude RR Adjusted RR Crude RR Adjusted RR
(Continued from previous page)
Follow-up duration‡
≤1 year 14 22 15 7 11 9
>1 year 37 64 52 18 26 37
Not reported 4 4 5 4 4 1
Length of time between tests for HIV
≤6 months 36 55 41 17 22 27
>6 months 6 17 16 4 12 12
Mixture of short and long intervals 3 4 4 2 3 5
Not reported 9 14 11 5 4 3
HSV-2 assay cutoff (only studies with Focus HerpeSelect as known assay)
1·1/manufacturer’s recommendation/unknown 14 22 15 8 9 13
>1·1 9 11 14 4 4 9
Definition of prevalent HSV-2 infection exposure‡
Baseline 47 79 60 NA NA NA
Baseline and >60 days before HIV seroconversion 1 2 7 NA NA NA
Baseline or >2 years before HIV seroconversion 1 1 1 NA NA NA
Before, or at same visit as, HIV seroconversion 3 5 2 NA NA NA
Same interval as HIV seroconversion 1 1 0 NA NA NA
At visit 6 months before HIV seroconversion 1 1 1 NA NA NA
Anytime 1 1 1 NA NA NA
Definition of incident HSV-2 infection exposure‡
≤60 days before HIV seroconversion NA NA NA 1 0 1
60 days before HIV seroconversion NA NA NA 1 0 5
≤6 months before HIV seroconversion NA NA NA 2 2 1
>6 months before HIV seroconversion NA NA NA 1 1 1
≤2 years before HIV seroconversion NA NA NA 1 1 1
Before, or at same visit as, HIV seroconversion NA NA NA 2 2 1
Visit before HIV seroconversion NA NA NA 1 1 1
Same interval as HIV seroconversion NA NA NA 1 1 0
Anytime NA NA NA 21 33 34
Not reported NA NA NA 1 0 2
Definition of unexposed group‡
HSV-2 negative at baseline 28 40 24 0 0 0
HSV-2 negative throughout follow-up 21 39 40 28 38 44
Not reported 6 11 8 1 3 3
Extraction of crude estimate‡‡‡
Reported 32 45 NA 14 20 NA
Calculated from available data 23 45 NA 11 21 NA
Adjusted for male circumcision status (men or women and men combined)‡§§¶¶
Yes 9 NA 14 5 NA 6
No 15 NA 21 9 NA 17
Unknown 3 NA 3 0 NA 0
Adjusted for condom use‡§§¶¶
Yes 15 NA 25 8 NA 18
No 23 NA 43 12 NA 27
Unknown 4 NA 4 1 NA 2
(Table 1 continues on next page)
6 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
Prevalent HSV-2 infection* Incident HSV-2 infection†
Number of Number of estimates Number of Number of estimates
studies (n=54) studies (n=28)
Crude RR Adjusted RR Crude RR Adjusted RR
(Continued from previous page)
Adjusted for female hormonal contraceptive use (women or women and men combined)‡§§¶¶
Yes 6 NA 13 4 NA 10
No 16 NA 26 8 NA 16
Unknown 2 NA 2 1 NA 2
Adjusted for any sexual behaviour (excluding condom use)‡§§¶¶
Yes 29 NA 48 16 NA 33
No 8 NA 21 3 NA 12
Unknown 3 NA 3 1 NA 2
Adjusted for genital ulcer disease‡§§¶¶
Yes 9 NA 18 8 NA 16
No 29 NA 51 11 NA 30
Unknown 3 NA 3 1 NA 1
Adjusted for number of sexual partnersদ
Yes 20 NA 33 11 NA 24
No 16 NA 32 8 NA 18
Unknown 5 NA 7 3 NA 5
Adjusted for ageদ
Yes 34 NA 63 14 NA 41
No 8 NA 9 5 NA 5
Unknown 0 NA 0 1 NA 1
Timing of incident HSV-2 infection relative to HIV acquisition‡||||
1 (definitely before) NA NA NA 7 8 14
2 (indeterminably close) NA NA NA 2 2 0
3 (before and indeterminably close) NA NA NA 12 12 11
4a (maybe after and indeterminably close or before) NA NA NA 8 14 17
4b (after and indeterminably close or before) NA NA NA 5 5 5
Type of estimate‡
Hazard ratio 29 31 43 15 13 25
Incidence ratio 17 22 11 8 8 9
Odds ratio 21 37 18 11 20 13
HSV-2=herpes simplex virus type 2. RR=relative risk. NA=not applicable. STI=sexually transmitted infection. *The crude number of estimates for all studies was 90 and the
adjusted number of estimates for all studies was 72. †The crude number of estimates for all studies was 41 and the adjusted number of estimates for all studies was 47.
‡Same study included in more than one subcategory. §Values might be estimated from ranges. ¶Women with higher-risk sexual behaviour, women working in food and
recreational facilities, STI clinic attendees, bar workers, and women in an HIV serodiscordant partnership (grouped with female sex workers in figures). ||Men with higher-risk
sexual behaviour (likely to be men who have sex with men), STI clinic attendees, male trucking company employees, clients of female sex workers, Thai military conscripts
(grouped with men who have sex with men in figures). **Estimates by sex could not be obtained. ††All case-control studies were subsequently analysed together. ‡‡Only studies
providing crude estimates or sufficient information to calculate a crude estimate. §§Includes probable adjustment, and variable not included in multivariate model because of
non-significance. ¶¶Only studies providing adjusted estimates. ||||Five subcategories for the timing sequence of HSV-2 and HIV seroconversion are defined in Methods.
Table 1: Description of studies and RR estimates of the association between HIV incidence and exposure to HSV-2 infection by participant and study
characteristics
population; R²=31%), world region (Africa vs outside 0·39–0·82), for incident HSV-2 infection compared with
Africa; R²=24%), definition of HSV-2 unexposed group prevalent HSV-2 infection (1·96, 1·16–3·31), and when
(HSV-2 negative at baseline vs HSV-2 negative the definition for the unexposed group was not reported
throughout follow-up; R²=24%), and HSV-2 exposure compared with when the definition for the unexposed
type (prevalent vs incident; R²=17%) significantly group was HSV-2 negative throughout follow-up (1·84,
explained the variation across study estimates (all 1·08–3·14). Variation across study estimates was not
p<0·05; table 2). The risk of HIV acquisition was about explained by confounder adjustment or any of the other
twice as large for general populations compared with factors explored, including star rating based on the
higher-risk populations (RR 0·53, 95% CI 0·38–0·75), Newcastle-Ottawa Scale. In a multivariate meta-
for Africa compared with outside Africa (0·57, regression analysis restricted to estimates for prevalent
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 7
Articles
Ne Adjusted RR (95% CI) I²
General population (women only)
Kamali et al (2003)37* 5·7 (3·0–10·7)
Biraro et al (2013)38 3·7 (2·2–6·2)
Kebede et al (2004)39 2·3 (0·5–10·6)
Brown et al (2007)40 4·4 (2·7–7·2)
Brown et al (2007)40 2·8 (1·5–5·3)
Brown et al (2007)40 8·6 (4·3–17·1)
Brown et al (2007)40 4·6 (1·6–13·1)
Mavedzenge et al (2011)41 2·6 (1·6–4·1)
Mavedzenge et al (2011)41 12·6 (4·4–36·3)
Todd et al (2006)42 2·9 (0·9–9·0)
Serwadda et al (2003)43 2·1 (1·2–3·7)
Mavedzenge et al (2011)41 1·6 (1·1–2·5)
Mavedzenge et al (2011)41 1·2 (0·6–2·3)
Mavedzenge et al (2011)41 3·0 (0·7–13·2)
Mavedzenge et al (2011)41 5·4 (0·7–39·5)
Gray et al (2011)44 1·0 (0·5–1·9)
Pooled estimate (prevalent) 11 2·5 (1·8–3·4) 68%
Pooled estimate (incident) 5 7·2 (4·5–11·5) 0%
General population (men only)
Kamali et al (2003)37* 7·5 (3·3–16·9)
Kebede et al (2004)39 1·3 (0·3–5·3)
Rositch et al (2014)45 2·0 (1·0–3·8)
Tobian et al (2009)46 2·9 (1·7–4·9)
Tobian et al (2009)46 1·1 (0·4–3·1)
Heffron et al (2011)47 6·0 (1·7–20·9)
Todd et al (2006)42 3·7 (1·3–10·4)
McFarland et al (1999)48 3·5 (2·2–5·8)
Serwadda et al (2003)43 1·5 (0·9–2·5)
Sobngwi−Tambekou et al (2009)49 3·3 (1·5–7·4)
Gray et al (2011)44 4·9 (2·0–11·8)
Pooled estimate (prevalent) 10 3·1 (2·2–4·3) 48%
Pooled estimate (incident) 1 1·1 (0·4–3·1) 0%
General population (men and women)
Guwatudde et al (2009)50 8·7 (1·1–67·2)
Pooled estimate (prevalent) 1 8·7 (1·1–67·2) 0%
Pooled estimate (incident) 0
Overall pooled estimate (all prevalent) 22 2·7 (2·2–3·4) 59%
Overall pooled estimate (all incident) 6 4·7 (2·2–10·1) 64%
Higher-risk populations (women only)
Kaul et al (2004)51 6·3 (1·5–27·1)
Riedner et al (2006)52 1·1 (0·4–2·7)
Masese et al (2015)53 2·5 (1·5–4·1)
Kapiga et al (2007)54 4·3 (1·5–12·4)
Figure 2: Pooled adjusted RR Masese et al (2015)53 3·0 (1·6–5·3)
estimates of the association Braunstein (2011 and 2012)55, 56 1·4 (0·5–3·8)
Kapiga et al (2013)57 1·8 (0·8–4·1)
between HIV incidence and Vandepitte et al (2013)58 1·6 (0·6–3·9)
exposure to HSV-2 infection Ramjee et al (2005)59 0·6 (0·2–1·7)
Mlisana et al (2012)60 2·1 (0·4–10·5)
Estimates for effect of both Nagot et al (2005)61 2·5 (0·7–8·3)
prevalent and incident HSV-2 Kilmarx et al (1998)62 0·6 (0·3–1·3)
Reynolds et al (2003)63* 0·5 (0·2–1·1)
infection on HIV acquisition
(timing 1; ie, HSV-2 Pooled estimate (prevalent) 12 1·5 (0·9–2·3) 63%
Pooled estimate (incident) 1 3·0 (1·6–5·3) 0%
seroconversion was observed
in a previous time interval and Higher-risk populations (men only)
so definitely occurred before Rakwar et al (1999)64 3·3 (1·2–9·2)
Turner et al (2003)65 1·1 (0·3–4·4)
HIV seroconversion) are Brown et al (2006)66 1·5 (1·1–2·1)
shown. Estimates are shown Holmberg et al (1988)67 2·4 (1·1–5·9)
Kingsley et al (199)68 0·9 (0·3–2·4)
for women and men Renzi et al (2003)69 2·8 (0·8–10·1)
combined when they could Nopkesorn et al (1998)70 2·0 (0·6–6·1)
not be obtained separately by Nelson et al (1997)71 3·1 (1·2–7·9)
van Griensven et al (2013)72 1·5 (1·1–2·1)
sex. Multiple estimates for the Reynolds et al (2003)63* 2·0 (1·4–2·8)
same study corresponding to Li et al (2012)73 4·0 (1·6–10·0)
Barnabas et al (2011)74 2·2 (1·4–3·5)
different study countries or
Pooled estimate (prevalent) 11 1·8 (1·5–2·2) 13%
areas are shown when these Pooled estimate (incident) 1 2·8 (0·8–10·1) 0%
could not be combined or
when it was not appropriate to Higher-risk populations (men and women)
do so (ie, countries spanning Celum et al (2010)26 2·0 (1·1–3·6)
He et al (2013)75 1·1 (0·3–3·9)
two sub-regions); however, all Pooled estimate (prevalent) 2 1·8 (1·1–3·0) 0%
estimates are independent Pooled estimate (incident) 0
(ie, for non-overlapping study Overall pooled estimate (all prevalent) 25 1·7 (1·4–2·1) 45%
populations) within each Overall pooled estimate (all incident) 2 2·9 (1·7–5·0) 0%
HSV-2 exposure subcategory.
Ne=number of estimates.
RR=relative risk. HSV-2=herpes 0·01 0·1 1 10 100
HSV-2 exposure type
simplex virus type 2. Incident HSV-2 infection Adjusted RR (log scale)
*Data from these studies were Prevalent HSV-2 infection
obtained from reference 11.
8 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
HSV-2 infection, risk group, world region, and definition
of the HSV-2 unexposed group were all significant
modifiers of the association with HIV infection (results Number of Adjusted RR Variance p value
not shown). However, we could not disentangle the estimates (95% CI) explained
effect of world region from that of risk group because no R² (%)
estimates for general populations were from outside Participant characteristics
Africa. Mean or median age
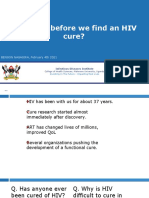
Figure 3 shows the pooled adjusted RR estimates from ≤25 years 14 1·00 0% 0·40
our subgroup analysis for exposure to prevalent or >25 years 33 1·34 (0·88–2·04) ·· ··
incident HSV-2 infection by key risk factors. Prevalent
Not reported 1 1·26 (0·32–4·88) ·· ··
HSV-2 infection was associated with a significantly
Sex
(95% CI did not overlap) higher risk of HIV acquisition
in general populations (adjusted RR 2·7, 95% CI 2·2–3·4; Women 23 1·00 0% 0·97
Ne=22; I²=59%) than in higher-risk populations Men 22 1·02 (0·68–1·53) ·· ··
(1·7, 1·4–2·1; Ne=25; I²=45%; same as shown in figure 2) Combined* 3 0·90 (0·36–2·25) ·· ··
and in Africa (2·5, 2·1–3·0; Ne=34; I²=52%) than outside Risk group
Africa (1·5, 1·2–2·0; Ne=13; I²=56%), but not for any General population 22 1·00 31% 0·0004
other characteristic explored. Higher-risk population 26 0·53 (0·38–0·75) ·· ··
For exposure to incident HSV-2 infection, the risk of
World region (derived from WHO region)
HIV acquisition was significantly higher in younger
African region 34 1·00 24% 0·003
(≤25 years; adjusted RR 7·6, 95% CI 4·4–13·3; Ne=3;
Outside Africa 14 0·57 (0·39–0·82) ·· ··
I²=0%; figure 3) than in older (>25 years; 2·5, 1·6–3·9;
Ne=4; I²=3%) individuals; however, no study estimates HSV-2 prevalence
were available for younger individuals in higher-risk ≤30% 10 1·00 6% 0·08
populations, whereas two of four estimates for older >30% 37 0·97 (0·63–1·51) ·· ··
individuals were from higher-risk populations. The risk Not reported 1 0·24 (0·07–0·85) ·· ··
of HIV acquisition after exposure to incident HSV-2 Study characteristics
infection was also significantly higher when HIV testing Study year (mid-point)
was done every 6 months or less (5·0, 3·1–8·1; Ne=7;
Pre-2000 18 1·00 0% 0·85
I²=38%) than when tests were done at a mixture of short
2000 onwards 24 1·13 (0·74–1·71) ·· ··
and long intervals (1·1, 0·4–3·1; Ne=1; I²=0%), although
this analysis was based on only one study. No other Not reported 6 1·05 (0·51–2·14) ·· ··
significant differences were observed, although the Study design
magnitude of the association tended to be larger for Cohort 25 1·00 0% 0·69
women than for men. Notably, most study estimates Controlled trial 15 1·20 (0·77–1·86) ·· ··
came from women in general populations in Africa. Our Case-control (including nested case-control) 8 0·98 (0·56–1·71) ·· ··
subgroup analysis showed that pooled adjusted RR Controlled trial intervention group
estimates were increased, although not significantly, Control 0 ·· ·· ··
when exposure to incident HSV-2 infection was known
Intervention 0 ·· ·· ··
to have or might have occurred after HIV (timing 4a and
Combined 19 NA ·· ··
4b vs timing 1; figure 3).
The study characteristics relevant to the evaluation of Follow-up duration
study quality, and the results of the Newcastle-Ottawa ≤1 year 12 1·00 0% 0·97
Scale assessment, are summarised in the appendix. Of >1 year 32 0·95 (0·59–1·52) ·· ··
the 55 adjusted estimates included in our principal Not reported 4 0·94 (0·39–2·25) ·· ··
meta-analysis, a seven-star or eight-star rating was the Length of time between tests for HIV
most common (Ne=31). The most common reasons for ≤6 months 31 1·00 0% 0·98
loss of a star were defining the HSV-2 unexposed group
>6 months 6 0·99 (0·55–1·78) ·· ··
by use of baseline status and no matching or adjustment
Mixture of short and long intervals 3 0·86 (0·37–2·04) ·· ··
for number of sexual partners. However, a star could
Not reported 8 1·07 (0·62–1·84) ·· ··
also be lost if the required information for assessment
was not reported in the paper, which is not necessarily HSV-2 assay cutoff (only those studies with Focus HerpeSelect as known assay)
the same as poor study quality. Conversely, a star could 1·1/manufacturer’s recommendation/ 12 1·00 19% 0·20
unknown
have been awarded for adequate participant retention
(low loss to follow-up), which was assessed on the basis >1·1 7 1·57 (0·79–3·10) ·· ··
of the information in the publication but which might (Table 2 continues on next page)
not have mentioned all dropouts.
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 9
Articles
available for exposure to incident HSV-2 infection than
Number of Adjusted RR Variance p value
estimates (95% CI) explained
for exposure to prevalent HSV-2 infection made the
R² (%) assessment for incident HSV-2 infection more difficult.
(Continued from previous page)
In a meta-regression analysis, crude RR estimates
calculated from the available data were lower than those
HSV-2 exposure type
reported in the studies (0·79, 95% CI 0·57–1·09;
Prevalent 40 1·00 17% 0·01
R²=2·5%; p=0·15), although the difference was not
Incident 8 1·96 (1·16–3·31) ·· ··
significant. Our qualitative assessment found some
Definition of unexposed group evidence of selective reporting of estimates based on
HSV-2 negative throughout follow-up 21 1·00 24% 0·005 significance (eg, studies reporting crude but not
HSV-2 negative at baseline 19 0·76 (0·52–1·11) ·· ·· adjusted estimates or only mentioning the significance
Not reported 8 1·84 (1·08–3·14) ·· ·· of an association without presenting any estimates;
Adjusted for male circumcision status (men or women and men combined) appendix).
No 15 1·00 0% 0·48
Yes 7 1·33 (0·84–2·10) ·· ··
Discussion
This systematic review and meta-analysis provided new
Not reported 3 1·08 (0·57–2·05) ·· ··
insight into the effect of HSV-2 infection on risk of HIV
Adjusted for condom use acquisition by analysis of 57 longitudinal studies of
No 27 1·00 0% 0·88 different study designs. We found good evidence that
Yes 17 1·10 (0·72–1·68) ·· ·· HIV incidence in general populations is roughly tripled
Not reported 4 1·13 (0·52–2·48) ·· ·· by exposure to prevalent HSV-2 infection (adjusted
Adjusted for female hormonal contraceptive use (women or women and men combined) RR 2·7, 95% CI 2·2–3·4), with an even larger increase in
No 17 1·00 0% 0·70 HIV risk after exposure to incident HSV-2 infection
Yes 7 1·25 (0·58–2·69) ·· ··
(4·7, 2·2–10·1). The greater cofactor effect for incident
HSV-2 infection than for prevalent HSV-2 infection might
Not reported 2 1·82 (0·34–9·81) ·· ··
be because newly acquired HSV-2 infection is associated
Adjusted for any sexual behaviour (excluding condom use)
with an increased frequency and severity of genital
No 9 1·00 0% 0·48 ulceration, viral shedding, and inflammation in the
Yes 36 1·39 (0·81–2·37) ·· ·· genital tract, symptoms and manifestations that decrease
Not reported 3 1·46 (0·58–3·69) ·· ·· with time after infection.14–16 These biological mechanisms
Adjusted for genital ulcer disease and gradient in risk strengthen the argument for a
No 36 1·00 10% 0·14 genuine biological effect of HSV-2 infection on HIV
Yes 9 1·54 (0·97–2·45) ·· ··
acquisition risk.
In addition to differences by prevalent versus incident
Not reported 3 1·61 (0·60–4.34) ·· ··
HSV-2 infection, heterogeneity in the magnitude of the
Adjusted for number of sexual partners
association across adjusted RR estimates was also
No 19 1·00 0% 0·46
explained by population risk group. The associations
Yes 23 0·85 (0·55–1·31) ·· ·· remained significant but were somewhat lower
Not reported 6 0·68 (0·36–1·26) ·· ·· among higher-risk populations than among general
Adjusted for age populations, perhaps because these populations have an
No 6 1·00 0% 0·99 increased risk of HIV independent of HSV-2 or because
Yes 42 1·00 (0·54–1·85) ·· ·· higher-risk individuals infected with HSV-2 might be
Estimate type
more likely to use condoms or abstain from sex when
symptomatic.
Hazard ratio or incidence ratio 39 1·00 0% 0·25
The results of our systematic review and meta-analysis
Odds ratio 9 0·74 (0·45–1·23) ·· ··
were generally in line with, and strengthen results from,
Study quality (as defined by number of stars awarded with Newcastle-Ottawa scale) previous meta-analyses.11,12 The 38 studies published
Increase of 1 star (continuous variable) 48 1·00 (0·85–1·17) 0% 0·96 since the last systematic search and review,11 and the
Only independent adjusted RR estimates were included. RR=relative risk. HSV-2=herpes simplex virus type 2.
large body of study information extracted, allowed us to
NA=not applicable. *Estimates by sex could not be obtained. comprehensively review existing evidence on the
association between HSV-2 and HIV infections and
Table 2: Results of univariate meta-regression analysis of adjusted RR estimates
assess the effects of a wide range of factors related to
participant and study characteristics, including study
There was little indication of publication bias from the quality, which have not been previously explored. We
funnel plots (appendix): most study estimates were also produced the first pooled estimates of the association
evenly distributed around the overall pooled crude and between exposure to incident HSV-2 infection and
adjusted RR estimates. However, the fewer RR estimates subsequent HIV acquisition.
10 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
Ne Adjusted RR (95% CI) I²
Timing of incident HSV-2 infection relative to HIV acquisition
1 (definitely before) 8 4·1 (2·3–7·2) 58%
2 (indeterminably close) 0 ·· ··
3 (before and indeterminably close) 8 2·8 (1·7–4·6) 56%
4a (maybe after and indeterminably close or before) 8 5·7 (4·2–7·7) 0
4b (after and indeterminably close or before) 4 5·5 (3·9–7·6) 6%
World region
Incident HSV-2 infection
Outside Africa 1 2·8 (0·8–10·1) 0%
Africa 7 4·3 (2·3–8·0) 63%
Prevalent HSV-2 infection
Outside Africa 13 1·5 (1·2–2·0) 56%
Africa 34 2·5 (2·1–3·0) 52%
Sex
Incident HSV-2 infection
Women 6 5·4 (3·2–9·2) 43%
Women and men 0 ·· ··
Men 2 1·6 (0·6–4·1) 25%
Prevalent HSV-2 infection
Women 23 1·9 (1·5–2·6) 69%
Women and men 3 2·0 (1·0–4·2) 28%
Men 21 2·4 (1·9–2·9) 50%
FSWs or MSM
Incident HSV-2 infection
FSWs 1 3·0 (1·6–5·3) 0%
MSM 1 2·8 (0·8–2·7) 0%
Prevalent HSV-2 infection
FSWs 7 1·5 (0·8-2·7) 65%
MSM 7 1·7 (1·4–2·1) 26%
Population risk group
Incident HSV-2 infection
General population 6 4·7 (2·2–10·1) 64%
Higher-risk population 2 2·9 (1·7–5·0) 0%
Prevalent HSV-2 infection
General population 22 2·7 (2·2–3·4) 59%
Higher-risk population 25 1·7 (1·4–2·1) 45%
Mean or median age
Incident HSV-2 infection
≤25 years 3 7·6 (4·4–13·3) 0%
>25 years 4 2·5 (1·6–3·9) 3%
Not reported 0 ·· ··
Prevalent HSV-2 infection
≤25 years 16 1·9 (1·3–2·8) 74%
>25 years 34 2·3 (2·0–2·8) 50%
Not reported 1 2·4 (1·1–5·9) 0%
Definition of unexposed group
Incident HSV-2 infection
HSV-2 negative at baseline 0 ·· ··
HSV-2 negative throughout follow−up 5 3·4 (1·7–6·7) 67%
Not reported 3 6·9 (2·8–17·2) 20%
Prevalent HSV-2 infection
HSV-2 negative at baseline 20 1·8 (1·4–2·2) 33%
HSV-2 negative throughout follow−up 20 2·3 (1·8–3·0) 64%
Not reported 8 2·7 (1·7–4·1) 71%
Length of time between testing for HIV
Incident HSV-2 infection
≤6 months 7 5·0 (3·1–8·1) 38%
>6 months 0 ·· ··
Mixture of short and long intervals 1 1·1 (0·4–3·1) 0%
Not reported 0 ·· ··
Prevalent HSV-2 infection
≤6 months 30 2·0 (1·7–2·4) 59%
>6 months 6 2·3 (1·6–3·4) 39%
Mixture of short and long intervals 3 2·9 (1·9–4·3) 0%
Not reported 8 2·4 (1·3–4·4) 75%
HSV-2 exposure type 0·1 0 10 100
Incident HSV-2 infection Adjusted RR (log scale)
Prevalent HSV-2 infection
Figure 3: Sub-pooled adjusted RR estimates of the association between HIV incidence and exposure to HSV-2 infection
Estimates for effect of both prevalent and incident HSV-2 infection on HIV acquisition (timing 1; ie, HSV-2 seroconversion was observed in a previous time interval
and so definitely occurred before HIV seroconversion) are shown. Estimates were added for sub-pooling if they were available by subcategories, although only
independent study estimates were included within a subcategory. RR=relative risk. HSV-2=herpes simplex virus type 2. Ne=number of estimates. FSWs=female sex
workers. MSM=men who have sex with men.
HSV-2 and HIV are lifelong infections that affect estimates. However, the risk of residual confounding
genital sites and have similar risk factors, such as could not be totally eliminated because many potential
sexual behaviour, which increases the risk of spurious confounding factors were often not controlled for, even
association in observational studies because of in adjusted estimates. The presence of HSV-2 infection
confounding. We minimised the risk of confounding at (particularly incident HSV-2 infection) might be a marker
the study level by focusing our analysis on adjusted of having had sex with a partner infected with HIV
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 11
Articles
because of the higher prevalence of HSV-2 among HIV- sufficiently frequently to disentangle the sequence of
infected than among non-HIV-infected individuals.76–78 infection. However, those estimates that included known
Except for serodiscordant-couple studies, in which or possible HIV infection before HSV-2 acquisition were
partner HIV status was known, few studies controlled for not significantly different to our estimate for timing 1.
partner characteristics. Additionally, some studies Our qualitative assessment of selective reporting of
inappropriately adjusted for genital ulcer disease, which crude and adjusted estimates based on significance found
might have biased pooled estimates toward the null value some evidence of publication bias. However, publication
because HSV-2 commonly causes genital ulcers and bias was not significant from either funnel plots or our
these act as a point of entry for HIV.13 Nevertheless, we meta-regression comparing reported crude estimates
did not find any notable difference between crude and with crude estimates derived from available data. We did
adjusted pooled estimates, and, in the meta-regression not find any evidence in our meta-regression that study
analysis, we found that adjustment for key confounders quality influenced the association between HSV-2 and
was not associated with the effect size. Confounding HIV, except where the definition of HSV-2 negative was
could also have arisen from combining estimates from not reported, which was associated with a significantly
heterogeneous studies, which is an important reason for increased risk of HIV acquisition due to HSV-2.
doing detailed meta-regression and subgroup analyses. Understanding the effect of HSV-2 infection on HIV risk
Fewer estimates for incident HSV-2 than for prevalent is essential for several reasons. From a clinical perspective,
HSV-2 increased the risk of confounding when knowledge of this association informs the advice and
combining heterogeneous studies, but also precluded a information given to individuals diagnosed with genital
multivariate meta-regression analysis for incident HSV-2 herpes, who might be at increased risk of acquiring HIV.
infection. No estimates were available for general Much, if not most, of HSV-associated HIV transmission is
populations outside Africa for either prevalent or incident thought to occur outside symptomatic episodes, including
HSV-2 infection, meaning that our results might not be among individuals who harbour HSV-2 infection but have
generalisable to general populations outside this setting. never had symptoms of genital herpes. Thus, from a
Furthermore, our finding of a higher risk of HIV with population perspective, understanding the interaction
HSV-2 among general populations than among higher- between HSV-2 and HIV is also important for informing
risk populations could have been confounded by world public health interventions for the control of both
region (or vice versa). infections, because an intervention targeting HSV-2 might
Another potential threat to validity was misclassification have additional, indirect benefits on HIV.
bias of the exposure to HSV-2 infection. Misclassification Current prevention and treatment options for HSV-2
bias can occur if HSV-2 exposure is defined solely infection are imperfect and limited by the often
according to HSV-2 antibody status at baseline and some asymptomatic presentation of HSV-2 infection.3
unexposed individuals seroconvert to HSV-2 during the However, development of new interventions is underway.
study. Although exposure status was defined solely on Multipurpose prevention technologies (eg, microbicides)
baseline HSV-2 infection status in half of the studies that target both HIV and HSV-2 infection hold promise,
estimating the association between prevalent HSV-2 but developments have been hampered by low
infection and HIV acquisition, we found only weak compliance and acceptability among women.22 The best
indication that the association between HSV-2 and HIV option is likely to be an effective vaccine against HSV-2
was lower in those studies. However, in our meta- infection. Efforts to develop an HSV-2 vaccine are
regression analyses, estimates were significantly underway.27 HSV-2 infection is a common infection
increased for unknown definition of the unexposed globally, but has a particularly high incidence in specific
comparison group, which might be a proxy for poor settings where HIV is endemic, such as sub-Saharan
study quality more generally. Africa, and among higher-risk groups, who are important
To minimise the risk of reverse causation, we only in concentrated HIV epidemics. Therefore, addressing
included longitudinal studies and categorised estimates the interactions between HSV-2 and HIV could produce
for effect of incident HSV-2 infection on HIV acquisition substantial health and economic gains. This meta-
according to the timing of HSV-2 infection compared analysis is an important step towards clearer
with HIV seroconversion. For our principal meta- quantification of the potential magnitude of that benefit.
analysis and meta-regression, we restricted inclusion of Contributors
estimates for incident HSV-2 infection to when incident KJL, SLG, and M-CB designed the study with input from all coauthors.
HSV-2 infection was known with greatest certainty to KJL and JARE contributed equally to the literature search, data
extraction, forest plots, meta-regression, and subgroup analysis.
have occurred before HIV seroconversion (ie, timing 1), KJL wrote the first version of the manuscript with input from JARE.
excluding any estimates for which HSV-2 infection was M-CB supervised JARE, gave advice on the direction of the analysis, and
known to or might have occurred after HIV infection. By guided the different aspects of the analysis. SLG oversaw the study and
erring on the side of caution, we might have inadvertently provided advice on the different stages as required. JTS contributed
expertise on HSV-2. KMET and PV supervised KJL and contributed
excluded estimates for when HSV-2 infection occurred technical expertise. All authors contributed to the interpretation of
before HIV in studies where testing was not done results and revised the different versions of the manuscript.
12 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
Articles
Declaration of interests 16 Corey L, Holmes KK. Genital herpes simplex virus infections:
KJL reports personal fees from WHO during the conduct of the study. current concepts in diagnosis, therapy, and prevention.
JARE reports grants from the US National Institutes of Health (NIH) Ann Intern Med 1983; 98: 973–83.
during the conduct of the study and grants from the Wellcome Trust 17 Todd J, Riedner G, Maboko L, et al. Effect of genital herpes on
outside of the submitted work. KMET reports personal fees and other cervicovaginal HIV shedding in women co-infected with HIV and
support from Aquarius Population Health outside the submitted work. HSV-2 in Tanzania. PLoS One 2013; 8: e59037.
M-CB reports non-financial support from WHO and grants from the NIH 18 Gray RH, Wawer MJ, Brookmeyer R, et al, for the Rakai Project
through the HIV Prevention Trials Network (HPTN), both during the Team. Probability of HIV-1 transmission per coital act in
monogamous, heterosexual, HIV-1-discordant couples in Rakai,
conduct of the study. SLG, JTS, and PV declare no competing interests.
Uganda. Lancet 2001; 357: 1149–53.
Acknowledgments 19 Augenbraun M, Feldman J, Chirgwin K, et al. Increased genital
KJL, PV, and KMET thank the National Institute for Health Research shedding of herpes simplex virus type 2 in HIV-seropositive
(NIHR) Health Protection Research Unit (HPRU) in Evaluation of women. Ann Intern Med 1995; 123: 845–47.
Interventions at the University of Bristol for research support. JARE and 20 Schacker T, Zeh J, Hu HL, Hill E, Corey L. Frequency of
M-CB acknowledge partial support from the HPTN Modelling Centre, symptomatic and asymptomatic herpes simplex virus type 2
which is funded by the US National Institutes of Health (NIH UM1 reactivations among human immunodeficiency virus-infected men.
AI068617) through HPTN. JTS acknowledges funding from the NIH J Infect Dis 1998; 178: 1616–22.
National Institute of Allergy and Infectious Diseases (NIAID; 21 Schelar E, Polis CB, Essam T, et al. Multipurpose prevention
P01 AI030731). SLG acknowledges support from NIH/NIAID technologies for sexual and reproductive health: mapping global
(U01 AI108543). PV was also supported by the National Institute for needs for introduction of new preventive products. Contraception
2016; 93: 32–43.
Drug Abuse (R01 DA037773-01A1), the HIV Modelling Consortium
funded by the Bill & Melinda Gates Foundation, and the NIHR HPRU in 22 Abdool Karim SS, Abdool Karim Q, Kharsany AB, et al.
Tenofovir gel for the prevention of herpes simplex virus type 2
Sexually Transmitted Infections and Blood Borne Viruses. These funders
infection. N Engl J Med 2015; 373: 530–39.
had no role in the writing of the manuscript nor in the decision to
23 Celum C, Morrow RA, Donnell D, et al. Daily oral tenofovir and
submit the manuscript for publication. The authors thank
emtricitabine-tenofovir preexposure prophylaxis reduces herpes
Birgitte Giersing from WHO for helping to coordinate funding support simplex virus type 2 acquisition among heterosexual
for this work. SLG is a staff member of WHO. The views expressed are HIV-1-uninfected men and women: a subgroup analysis of a
those of the authors and not necessarily those of WHO, the UK National randomized trial. Ann Intern Med 2014; 161: 11–19.
Health Service, the NIHR, the Department of Health, Public Health 24 Celum C, Wald A, Hughes J, et al, for the HPTN 039 Protocol Team.
England, or any of the institutions with which the authors are affiliated. Effect of aciclovir on HIV-1 acquisition in herpes simplex virus 2
References seropositive women and men who have sex with men: a randomised,
1 WHO. Global Health Observatory (GHO) data: HIV/AIDS. double-blind, placebo-controlled trial. Lancet 2008; 371: 2109–19.
http://www.who.int/gho/hiv/en (accessed April 8, 2016). 25 Watson-Jones D, Weiss HA, Rusizoka M, et al. Effect of herpes
2 Looker KJ, Magaret AS, Turner KME, Vickerman P, Gottlieb SL, simplex suppression on incidence of HIV among women in
Newman LM. Global estimates of prevalent and incident herpes Tanzania. N Engl J Med 2008; 358: 1560–71.
simplex virus type 2 infections in 2012. PLoS One 2015; 1: e114989. 26 Celum C, Wald A, Lingappa JR, et al. Acyclovir and transmission of
3 Gupta R, Warren T, Wald A. Genital herpes. Lancet 2007; 370: 2127–37. HIV-1 from persons infected with HIV-1 and HSV-2. N Engl J Med
2010; 362: 427–39.
4 Schiffer JT, Corey L. Rapid host immune response and viral dynamics
in herpes simplex virus-2 infection. Nat Med 2013; 19: 280–90. 27 Johnston C, Gottlieb SL, Wald A. Status of vaccine research and
development of vaccines for herpes simplex virus. Vaccine 2016;
5 Catotti DN, Clarke P, Catoe KE. Herpes revisited. Still a cause of 34: 2948–52.
concern. Sex Transm Dis 1993; 20: 77–80.
28 Glynn JR, Biraro S, Weiss H. Herpes simplex virus type 2:
6 Fisman DN. Health related quality of life in genital herpes: a pilot a key role in HIV incidence. AIDS 2009; 23: 1595–98.
comparison of measures. Sex Transm Dis 2005; 81: 267–70.
29 Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting
7 Glynn JR, Carael M, Auvert B, et al, for the Study Group on the items for systematic reviews and meta-analyses: the PRISMA
Heterogeneity of HIV Epidemics in African Cities. Why do young statement. PLoS Med 2009; 6: e1000097.
women have a much higher prevalence of HIV than young men?
A study in Kisumu, Kenya and Ndola, Zambia. AIDS 2001; 30 Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of
15 (suppl 4): S51–60. observational studies in epidemiology: a proposal for reporting.
Meta-analysis Of Observational Studies in Epidemiology (MOOSE)
8 Holmes KK, Sparling PF, Stamm WE, et al. Genital Herpes. group. JAMA 2000; 283: 2008–12.
In: Corey L, Wald A, eds. Sexually transmitted diseases, 4th edn.
New York, NY: McGraw-Hill Medical, 2008. 31 Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale
(NOS) for assessing the quality of nonrandomised studies in
9 Kaushic C, Roth KL, Anipindi V, Xiu F. Increased prevalence of meta-analyses. http://www.ohri.ca/programs/clinical_
sexually transmitted viral infections in women: the role of female epidemiology/oxford.asp 11/01/2017 (accessed Jan 11, 2017).
sex hormones in regulating susceptibility and immune responses.
J Reprod Immunol 2011; 88: 204–09. 32 Higgins JP, Thompson SG. Quantifying heterogeneity in a
meta-analysis. Stat Med 2002; 21: 1539–58.
10 Tobian AA, Serwadda D, Quinn TC, et al. Male circumcision for the
prevention of HSV-2 and HPV infections and syphilis. N Engl J Med 33 Sterne JAC, Harbord RM. Funnel plots in meta-analysis.
2009; 360: 1298–309. Stata J 2004; 4: 127–41.
11 Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, 34 Egger M, Davey Smith G, Schneider M. Bias in meta-analysis
Hayes RJ. Herpes simplex virus 2 infection increases HIV detected by a simple, graphical test. BMJ 1997; 315: 629–34.
acquisition in men and women: systematic review and meta- 35 Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for
analysis of longitudinal studies. AIDS 2006; 20: 73–83. examining heterogeneity and combining results from several
12 Wald A, Link K. Risk of human immunodeficiency virus infection studies in meta-analysis. In: Egger M, Smith GD, Altman DG, eds.
in herpes simplex virus type 2-seropositive persons: a meta-analysis. Systematic reviews in health care: meta-analysis in context. 2nd
J Infect Dis 2002; 185: 45–52. edn. London: BMJ Publishing Group, 2001.
13 Van de Perre P, Segondy M, Foulongne V, et al. Herpes simplex virus 36 Viechtbauer W. Conducting meta-analyses in R with the metafor
and HIV-1: deciphering viral synergy. Lancet Infect Dis 2008; 8: 490–97. package. J Stat Softw 2010; 36: 1–48.
14 Phipps W, Saracino M, Magaret A, et al. Persistent genital herpes 37 Kamali A, Quigley M, Nakiyingi J, et al. Syndromic management of
simplex virus-2 shedding years following the first clinical episode. sexually-transmitted infections and behaviour change interventions
J Infect Dis 2011; 203: 180–87. on transmission of HIV-1 in rural Uganda: a community
randomised trial. Lancet 2003; 361: 645–52.
15 Corey L, Adams HG, Brown ZA, Holmes KK. Genital herpes
simplex virus infections: clinical manifestations, course, and 38 Biraro S, Kamali A, White R, et al. Effect of HSV-2 on
complications. Ann Intern Med 1983; 98: 958–72. population-level trends in HIV incidence in Uganda between 1990
and 2007. Trop Med Int Health 2013; 18: 1257–66.
www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X 13
Articles
39 Kebede Y, Dorigo-Zetsma W, Mengistu Y, et al. Transmission of 60 Mlisana K, Naicker N, Werner L, et al. Symptomatic vaginal
herpes simplex virus type 2 among factory workers in Ethiopia. discharge is a poor predictor of sexually transmitted infections and
J Infect Dis 2004; 190: 365–72. genital tract inflammation in high-risk women in South Africa.
40 Brown JM, Wald A, Hubbard A, et al. Incident and prevalent herpes J Infect Dis 2012; 206: 6–14.
simplex virus type 2 infection increases risk of HIV acquisition 61 Nagot N, Ouedraogo A, Ouangre A, et al. Is sexually transmitted
among women in Uganda and Zimbabwe. AIDS 2007; 21: 1515–23. infection management among sex workers still able to mitigate the
41 Mavedzenge SN, Weiss HA, Montgomery ET, et al. Determinants of spread of HIV infection in West Africa? J Acquir Immune Defic Syndr
differential HIV incidence among women in three southern African 2005; 39: 454–58.
locations. J Acquir Immune Defic Syndr 2011; 58: 89–99. 62 Kilmarx PH, Limpakarnjanarat K, Mastro TD, et al. HIV-1
42 Todd J, Grosskurth H, Changalucha J, et al. Risk factors influencing seroconversion in a prospective study of female sex workers in
HIV infection incidence in a rural African population: a nested northern Thailand: continued high incidence among brothel-based
case-control study. J Infect Dis 2006; 193: 458–66. women. AIDS 1998; 12: 1889–98.
43 Serwadda D, Gray RH, Sewankambo NK, et al. Human 63 Reynolds SJ, Risbud AR, Shepherd ME, et al. Recent herpes
immunodeficiency virus acquisition associated with genital ulcer simplex virus type 2 infection and the risk of human
disease and herpes simplex virus type 2 infection: a nested immunodeficiency virus type 1 acquisition in India. J Infect Dis
case-control study in Rakai, Uganda. J Infect Dis 2003; 188: 1492–97. 2003; 187: 1513–21.
44 Gray GE, Allen M, Moodie Z, et al, for the HVTN 503/Phambili 64 Rakwar J, Lavreys L, Thompson ML, et al. Cofactors for the
study team. Safety and efficacy of the HVTN 503/Phambili study of acquisition of HIV-1 among heterosexual men: prospective cohort
a clade-B-based HIV-1 vaccine in South Africa: a double-blind, study of trucking company workers in Kenya. AIDS 1999;
randomised, placebo-controlled test-of-concept phase 2b study. 13: 607–14.
Lancet Infect Dis 2011; 11: 507–15. 65 Turner KR, McFarland W, Kellogg TA, et al. Incidence and prevalence
45 Rositch AF, Mao L, Hudgens MG, et al. Risk of HIV acquisition of herpes simplex virus type 2 infection in persons seeking repeat HIV
among circumcised and uncircumcised young men with penile counseling and testing. Sex Transm Dis 2003; 30: 331–34.
human papillomavirus infection. AIDS 2014; 28: 745–52. 66 Brown EL, Wald A, Hughes JP, et al. High risk of human
46 Tobian AA, Ssempijja V, Kigozi G, et al. Incident HIV and herpes immunodeficiency virus in men who have sex with men with
simplex virus type 2 infection among men in Rakai, Uganda. herpes simplex virus type 2 in the EXPLORE study. Am J Epidemiol
AIDS 2009; 23: 1589–94. 2006; 164: 733–41.
47 Heffron R, Chao A, Mwinga A, et al. High prevalent and incident 67 Holmberg SD, Stewart JA, Gerber AR, et al. Prior herpes simplex
HIV-1 and herpes simplex virus 2 infection among male migrant virus type 2 infection as a risk factor for HIV infection. JAMA 1988;
and non-migrant sugar farm workers in Zambia. Sex Transm Infect 259: 1048–50.
2011; 87: 283–88. 68 Kingsley LA, Armstrong J, Rahman A, Ho M, Rinaldo CR Jr.
48 McFarland W, Gwanzura L, Bassett MT, et al. Prevalence and No association between herpes simplex virus type-2 seropositivity or
incidence of herpes simplex virus type 2 infection among male anogenital lesions and HIV seroconversion among homosexual
Zimbabwean factory workers. J Infect Dis 1999; 180: 1459–65. men. J Acquir Immune Defic Syndr 1990; 3: 773–79.
49 Sobngwi-Tambekou J, Taljaard D, Lissouba P, et al. Effect of HSV-2 69 Renzi C, Douglas JM Jr, Foster M, et al. Herpes simplex virus type 2
serostatus on acquisition of HIV by young men: results of a infection as a risk factor for human immunodeficiency virus acquisition
longitudinal study in Orange Farm, South Africa. J Infect Dis 2009; in men who have sex with men. J Infect Dis 2003; 187: 19–25.
199: 958–64. 70 Nopkesorn T, Mock PA, Mastro TD, et al. HIV-1 subtype E incidence
50 Guwatudde D, Wabwire-Mangen F, Eller LA, et al. Relatively low HIV and sexually transmitted diseases in a cohort of military conscripts
infection rates in rural Uganda, but with high potential for a rise: in northern Thailand. J Acquir Immune Defic Syndr Hum Retrovirol
a cohort study in Kayunga District, Uganda. PLoS One 2009; 4: e4145. 1998; 18: 372–79.
51 Kaul R, Kimani J, Nagelkerke NJ, et al. Monthly antibiotic 71 Nelson KE, Eiumtrakul S, Celentano D, et al. The association of herpes
chemoprophylaxis and incidence of sexually transmitted infections simplex virus type 2 (HSV-2), Haemophilus ducreyi, and syphilis with
and HIV-1 infection in Kenyan sex workers: a randomized HIV infection in young men in northern Thailand. J Acquir Immune
controlled trial. JAMA 2004; 291: 2555–62. Defic Syndr Hum Retrovirol 1997; 16: 293–300.
52 Riedner G, Hoffmann O, Rusizoka M, et al. Decline in sexually 72 van Griensven F, Thienkrua W, McNicholl J, et al. Evidence of an
transmitted infection prevalence and HIV incidence in female explosive epidemic of HIV infection in a cohort of men who have
barworkers attending prevention and care services in Mbeya sex with men in Thailand. AIDS 2013; 27: 825–32.
Region, Tanzania. AIDS 2006; 20: 609–15. 73 Li D, Li S, Liu Y, et al. HIV incidence among men who have sex with
53 Masese L, Baeten JM, Richardson BA, et al. Changes in the men in Beijing: a prospective cohort study. BMJ Open 2012; 2: e001829.
contribution of genital tract infections to HIV acquisition among 74 Barnabas RV, Wasserheit JN, Huang Y, et al, for the NIAID HIV
Kenyan high-risk women from 1993 to 2012. AIDS 2015; 29: 1077–85. Vaccine Trials Network. Impact of herpes simplex virus type 2 on
54 Kapiga SH, Sam NE, Bang H, et al. The role of herpes simplex virus HIV-1 acquisition and progression in an HIV vaccine trial
type 2 and other genital infections in the acquisition of HIV-1 among (the Step study). J Acquir Immune Defic Syndr 2011; 57: 238–44.
high-risk women in northern Tanzania. J Infect Dis 2007; 195: 1260–69. 75 He N, Duan S, Ding Y, et al. Antiretroviral therapy reduces HIV
55 Braunstein SL, Ingabire CM, Kestelyn E, et al. High human transmission in discordant couples in rural Yunnan, China.
immunodeficiency virus incidence in a cohort of Rwandan female PLoS One 2013; 8: e77981.
sex workers. Sex Transm Dis 2011; 38: 385–94. 76 Lemieux-Mellouki P, Drolet M, Brisson J, et al. Assortative mixing
56 Braunstein SL, van de Wijgert JH, Vyankandondera J, Kestelyn E, as a source of bias in epidemiological studies of sexually transmitted
Ntirushwa J, Nash D. Risk factor detection as a metric of STARHS infections: the case of smoking and human papillomavirus.
performance for HIV incidence surveillance among female sex Epidemiol Infect 2016; 144: 1490–99.
workers in Kigali, Rwanda. Open AIDS J 2012; 6: 112–21. 77 Boily M-C, Anderson RM. Human immunodeficiency virus
57 Kapiga SH, Ewings FM, Ao T, et al. The epidemiology of HIV and transmission and the role of other sexually transmitted diseases.
HSV-2 infections among women participating in microbicide and Measures of association and study design. Sex Transm Dis 1996;
vaccine feasibility studies in Northern Tanzania. PLoS One 2013; 23: 312–32.
8: e68825. 78 Malagón T, Lemieux-Mellouki P, Laprise JF, Brisson, M. Bias due to
58 Vandepitte J, Weiss HA, Bukenya J, et al. Alcohol use, mycoplasma correlation between times-at-risk for infection in epidemiologic
genitalium, and other STIs associated with HIV incidence among studies measuring biological interactions between sexually
women at high risk in Kampala, Uganda. J Acquir Immune Defic Syndr transmitted infections: a case study using human papillomavirus
2013; 62: 119–26. type interactions. Am J Epidemiol 2016; 184: 873–83.
59 Ramjee G, Williams B, Gouws E, Van Dyck E, De Deken B,
Karim SA. The impact of incident and prevalent herpes simplex
virus-2 infection on the incidence of HIV-1 infection among
commercial sex workers in South Africa. J Acquir Immune Defic Syndr
2005; 39: 333–39.
14 www.thelancet.com/infection Published online August 23, 2017 http://dx.doi.org/10.1016/S1473-3099(17)30405-X
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TRF 9999 NaDocument8 pagesTRF 9999 NaZakia DrajatNo ratings yet
- The Effectiveness of Surgical Procedures To PreventDocument9 pagesThe Effectiveness of Surgical Procedures To PreventZakia DrajatNo ratings yet
- Patient Care Breakthrough by SlidesgoDocument47 pagesPatient Care Breakthrough by SlidesgoZakia DrajatNo ratings yet
- Overactive Bladder Syndrome and Nocturia: Chapter OutlineDocument27 pagesOveractive Bladder Syndrome and Nocturia: Chapter OutlineZakia DrajatNo ratings yet
- The Effectiveness of Surgical Procedures To PreventDocument17 pagesThe Effectiveness of Surgical Procedures To PreventZakia DrajatNo ratings yet
- Covid-19 Human Igm Igg Assay Kit: Catalog Number Ka5826 96 AssaysDocument9 pagesCovid-19 Human Igm Igg Assay Kit: Catalog Number Ka5826 96 AssaysZakia DrajatNo ratings yet
- Review ArticleDocument15 pagesReview ArticleZakia DrajatNo ratings yet
- LalalalalDocument6 pagesLalalalalZakia DrajatNo ratings yet
- Bilateral Giant Fibroadenoma of The Breast: A CaseDocument4 pagesBilateral Giant Fibroadenoma of The Breast: A CaseNatalindah Jokiem Woecandra T. D.No ratings yet
- Research ArticleDocument7 pagesResearch ArticleZakia DrajatNo ratings yet
- Gude Man 2015Document15 pagesGude Man 2015Zakia DrajatNo ratings yet
- Interleukin-6 - A Key Regulator of Colorectal Cancer DevelopmentDocument6 pagesInterleukin-6 - A Key Regulator of Colorectal Cancer DevelopmentZakia DrajatNo ratings yet
- Effectiveness of Physically AbDocument12 pagesEffectiveness of Physically Abnur amalinaNo ratings yet
- Spectrums of Sexually Transmitted Infections in HIV-infected Patients in A Tertiary Care Teaching HospitalDocument5 pagesSpectrums of Sexually Transmitted Infections in HIV-infected Patients in A Tertiary Care Teaching HospitalZakia DrajatNo ratings yet
- Prevalence of Anogenital Warts in Men With HIV/AIDS and Associated FactorsDocument6 pagesPrevalence of Anogenital Warts in Men With HIV/AIDS and Associated FactorsZakia DrajatNo ratings yet
- The Diagnosis and Treatments of Inguinal Hernia After Radical ProstatectomyDocument6 pagesThe Diagnosis and Treatments of Inguinal Hernia After Radical ProstatectomyZakia DrajatNo ratings yet
- Ofy 017Document9 pagesOfy 017Zakia DrajatNo ratings yet
- Case Series of Syphilis and HIV Co-InfectionsDocument3 pagesCase Series of Syphilis and HIV Co-InfectionsZakia DrajatNo ratings yet
- Asm 2014122913444017Document7 pagesAsm 2014122913444017Zakia DrajatNo ratings yet
- The Diagnosis and Treatments of Inguinal Hernia After Radical ProstatectomyDocument6 pagesThe Diagnosis and Treatments of Inguinal Hernia After Radical ProstatectomyZakia DrajatNo ratings yet
- 5 6314175921729306716Document34 pages5 6314175921729306716Zakia DrajatNo ratings yet
- 18 Chapter 02 - Autopsy Legal, Social, and Ethical IssuesDocument9 pages18 Chapter 02 - Autopsy Legal, Social, and Ethical IssuesZakia DrajatNo ratings yet
- The Epidemiology and Etiology of Azoospermia: ReviewDocument12 pagesThe Epidemiology and Etiology of Azoospermia: ReviewZakia DrajatNo ratings yet
- NIH Public Access: Syphilis and HIV Co-Infection in Patients Who Attend An AIDS Outpatient Clinic in Vitoria, BrazilDocument10 pagesNIH Public Access: Syphilis and HIV Co-Infection in Patients Who Attend An AIDS Outpatient Clinic in Vitoria, BrazilZakia DrajatNo ratings yet
- Renal Colic: Pathophysiology, Diagnosis and Treatment: European UrologyDocument9 pagesRenal Colic: Pathophysiology, Diagnosis and Treatment: European UrologyZakia DrajatNo ratings yet
- Ulipristal Acetate: Approved Indication: FibroidsDocument2 pagesUlipristal Acetate: Approved Indication: FibroidsZakia DrajatNo ratings yet
- Spectrums of Sexually Transmitted Infections in HIV-infected Patients in A Tertiary Care Teaching HospitalDocument5 pagesSpectrums of Sexually Transmitted Infections in HIV-infected Patients in A Tertiary Care Teaching HospitalZakia DrajatNo ratings yet
- Ulipristal Acetate Clinical Pharmacology and PharmacokineticsDocument8 pagesUlipristal Acetate Clinical Pharmacology and PharmacokineticsZakia DrajatNo ratings yet
- Nazari An 2018Document16 pagesNazari An 2018Zakia DrajatNo ratings yet
- Slow Virus and Prion DiseaseDocument31 pagesSlow Virus and Prion DiseaseMimi Morallos-EspirituNo ratings yet
- Catalog Product BD Difco Dan Thermofisher (Gibco)Document6 pagesCatalog Product BD Difco Dan Thermofisher (Gibco)Billy PontenNo ratings yet
- Department of Molecular Biology. Covid 19 RT PCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Molecular Biology. Covid 19 RT PCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodnikhilaNo ratings yet
- Feline Panleukopenia Balram YadavDocument16 pagesFeline Panleukopenia Balram Yadavsanchi ranaNo ratings yet
- Malaria Mosquitoes (Anopheles) - Biogents AGDocument1 pageMalaria Mosquitoes (Anopheles) - Biogents AGscralettNo ratings yet
- Soil Transmitted HelminthiasisDocument9 pagesSoil Transmitted HelminthiasisSuperboinkyNo ratings yet
- Covid-19 RNA PCR For PIA: MPL ID: 029826 MR Syed Muhammad Jafar Abbas BokhariDocument1 pageCovid-19 RNA PCR For PIA: MPL ID: 029826 MR Syed Muhammad Jafar Abbas BokhariKamran KhalidNo ratings yet
- Measles Virus (Rubeola) SummaryDocument10 pagesMeasles Virus (Rubeola) SummaryTammy Utami DewiNo ratings yet
- The Impact of Wolbachia On Virus InfectionDocument13 pagesThe Impact of Wolbachia On Virus InfectionShirly DiazgranadosNo ratings yet
- JevaxDocument2 pagesJevaxjovedNo ratings yet
- Facts About MeaslesDocument4 pagesFacts About MeaslesTrishana GreenNo ratings yet
- Antiviral ChemotherapyDocument11 pagesAntiviral ChemotherapyAsmaa HwaidNo ratings yet
- Flipbook SummaryDocument5 pagesFlipbook SummaryMario Jr S. FloraNo ratings yet
- ZIRAA'AH, Volume 45 Nomor 1, Pebruari 2020 Halaman 1-9 p-ISSN 1412-1468 e-ISSN 2355-3545Document9 pagesZIRAA'AH, Volume 45 Nomor 1, Pebruari 2020 Halaman 1-9 p-ISSN 1412-1468 e-ISSN 2355-3545Muhamad DenaldiNo ratings yet
- English 5 Quarter 3 Week 1 Las 3Document2 pagesEnglish 5 Quarter 3 Week 1 Las 3Cristine Joy Villajuan AndresNo ratings yet
- Diagnosa Non SpesialistikDocument12 pagesDiagnosa Non SpesialistikWahyu PedjeNo ratings yet
- Goat DiseasesDocument33 pagesGoat DiseasesThe Municipal AgriculturistNo ratings yet
- Effictiveness of Eucalyptus Oil As Mosquito RepellentDocument1 pageEffictiveness of Eucalyptus Oil As Mosquito RepellentSHEAN GAYLE ANGNo ratings yet
- Disease by BacteriaDocument10 pagesDisease by BacteriaPratimaNo ratings yet
- How Long Before We Find An HIV Cure?: BENSON NASASIRA, February 4th 2021Document20 pagesHow Long Before We Find An HIV Cure?: BENSON NASASIRA, February 4th 2021Nasasira BensonNo ratings yet
- WebpageDocument4 pagesWebpageapi-443100867No ratings yet
- Chapter 65 (Introduction To Viruses)Document16 pagesChapter 65 (Introduction To Viruses)leoNo ratings yet
- Yaws Eradication ProgrammeDocument82 pagesYaws Eradication ProgrammeAparna Aby50% (2)
- Claforan (Cefotaxime) PDFDocument18 pagesClaforan (Cefotaxime) PDFdinniNo ratings yet
- GI Tract InfectionsDocument29 pagesGI Tract InfectionsMahrukh SiddiquiNo ratings yet
- Bacteria and Viruses ExamDocument9 pagesBacteria and Viruses ExamWillis Blade HumpreyNo ratings yet
- Development of Probiotics and PrebioticsDocument40 pagesDevelopment of Probiotics and PrebioticsJonathan LejarazuNo ratings yet
- Anatomy and Physiology MeaslesDocument3 pagesAnatomy and Physiology MeaslesCamila DaludadoNo ratings yet
- Prevention of DiseaseDocument18 pagesPrevention of Diseaserajforever17No ratings yet
- Casauay and Pacunana Group 15 1Document4 pagesCasauay and Pacunana Group 15 1Steve EstebanNo ratings yet