You might also like
- Opiates 1986 George R Lenz Suzanne M Evans D Eric Walters Anton J Hopfinger Academic Press ISBN 012443830X 0-12-443830 X 978 0124438309Document287 pagesOpiates 1986 George R Lenz Suzanne M Evans D Eric Walters Anton J Hopfinger Academic Press ISBN 012443830X 0-12-443830 X 978 0124438309Nick Coffey100% (4)
- (Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioDocument455 pages(Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioEsteban Gonzàlez RodriguezNo ratings yet
- Health and Safety Standards in D&TDocument9 pagesHealth and Safety Standards in D&TAnnie HawkinsNo ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet
- Perioperative Concepts and Nursing ManagementDocument107 pagesPerioperative Concepts and Nursing ManagementHarley Justiniani Dela CruzNo ratings yet
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- Food Safety Plan For CateringDocument80 pagesFood Safety Plan For CateringNghia Khang100% (1)
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Risk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeDocument3 pagesRisk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeSenyorita KHaye75% (12)
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)
- Understanding Lupus NephritisDocument21 pagesUnderstanding Lupus Nephritissaritha Oruganti100% (1)
- Systemic - Sclerosis Nature Review 2014Document22 pagesSystemic - Sclerosis Nature Review 2014CT TANNo ratings yet
- Assessment of Membrane Erythrocyte Cholesterol Level in Sickle Cell DiseaseDocument9 pagesAssessment of Membrane Erythrocyte Cholesterol Level in Sickle Cell DiseaseSely wulan widya ningsihNo ratings yet
- CSR 2018 s40942-018-0137-8Document5 pagesCSR 2018 s40942-018-0137-8Felix Valerian HalimNo ratings yet
- Veterinary Science Histopathological Retrospective Study of Canine Renal Disease in Korea, 2003 2008Document7 pagesVeterinary Science Histopathological Retrospective Study of Canine Renal Disease in Korea, 2003 2008ninaNo ratings yet
- DRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisDocument4 pagesDRESS Syndrome in A Patient On Sulfasalazine For Rheumatoid ArthritisChistian LassoNo ratings yet
- Leptospirosis CasosDocument2 pagesLeptospirosis CasosfelipeNo ratings yet
- Megaloblastic Anemia Case in Addison's Disease PatientDocument4 pagesMegaloblastic Anemia Case in Addison's Disease PatientIzzan Ferdi AndrianNo ratings yet
- Cat Blood NeutrophilsDocument12 pagesCat Blood Neutrophilsnora ivanovaNo ratings yet
- Dental Sealant ToxicityDocument14 pagesDental Sealant ToxicityGuru SvamiNo ratings yet
- Amyloid Beta Multiple Mechanisms of Toxicity and Only Some Protective EffectsDocument16 pagesAmyloid Beta Multiple Mechanisms of Toxicity and Only Some Protective EffectsEvernim OmpacanNo ratings yet
- Rekam Anusha Et Al.Document3 pagesRekam Anusha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Uremic neuropathy overview: causes, diagnosis and treatmentDocument6 pagesUremic neuropathy overview: causes, diagnosis and treatmentRizki Muhammad RanandaNo ratings yet
- Renal Involvement in Leptospirosis - New Insights Into Pathophysiology and TreatmentDocument5 pagesRenal Involvement in Leptospirosis - New Insights Into Pathophysiology and TreatmentCandy Garcia Aceveda ReyesNo ratings yet
- Toxicon: SciencedirectDocument14 pagesToxicon: SciencedirectNa d'Nazaie CodeNo ratings yet
- Primer: Systemic SclerosisDocument21 pagesPrimer: Systemic Sclerosishumberto_620No ratings yet
- Primer: BronchiectasisDocument18 pagesPrimer: BronchiectasisAnanta Bryan Tohari WijayaNo ratings yet
- 329-Article Text-1006-2-10-20200429Document5 pages329-Article Text-1006-2-10-20200429Drina PaglinawanNo ratings yet
- 10 11648 J Ijidt 20200501 12Document5 pages10 11648 J Ijidt 20200501 12hern andesNo ratings yet
- HS BCSH Sept 2011Document40 pagesHS BCSH Sept 2011lidya_zhuangNo ratings yet
- Leptospirosis-Associated Acute Kidney Injury: Pdate RticleDocument8 pagesLeptospirosis-Associated Acute Kidney Injury: Pdate RticleFadhilatul KhairNo ratings yet
- The Rationale For Extracorporeal Therapies in SepsisDocument9 pagesThe Rationale For Extracorporeal Therapies in SepsisLoudry ElfaNo ratings yet
- Thesis Jessica KattanDocument45 pagesThesis Jessica Kattanaztigan100% (2)
- 1543-2165-133.12.1943 Mass General AutopsiesDocument6 pages1543-2165-133.12.1943 Mass General AutopsiesgasfgdNo ratings yet
- CriptococoseDocument6 pagesCriptococoseEllen MoreiraNo ratings yet
- 1 s2.0 S0268960X22000182 MainDocument10 pages1 s2.0 S0268960X22000182 Mainafg_19No ratings yet
- Oral Findings and Diagnosis of Systemic Lupus ErythematosusDocument6 pagesOral Findings and Diagnosis of Systemic Lupus ErythematosusArditya Dwi YudistiraNo ratings yet
- Pathophysiology, Diagnosis and Treatment of Neonatal Sepsis: Review ArticleDocument7 pagesPathophysiology, Diagnosis and Treatment of Neonatal Sepsis: Review ArticleZakia DrajatNo ratings yet
- Multiple Organ Dysfunction SyndromeDocument4 pagesMultiple Organ Dysfunction SyndromeAna Reyes100% (1)
- Diagnosing and predicting outcome in leptospirosis: the need for clinically relevant basic sciences researchDocument3 pagesDiagnosing and predicting outcome in leptospirosis: the need for clinically relevant basic sciences researchAnonymous fOcbAtNo ratings yet
- Multiple Organ Dysfunction SyndromeDocument4 pagesMultiple Organ Dysfunction SyndromeSha NaNo ratings yet
- Chronic Inflammatory Response Syndrome Diagnosis and Treatment by Kellyn Milani 2Document6 pagesChronic Inflammatory Response Syndrome Diagnosis and Treatment by Kellyn Milani 2Marcel PuscasNo ratings yet
- Nejmoa 1114576Document11 pagesNejmoa 1114576mz zumrodinNo ratings yet
- Staphylococcal Scalded Skin Syndrome in Child A CADocument6 pagesStaphylococcal Scalded Skin Syndrome in Child A CAsalshabilaNo ratings yet
- Systemic Disorders Associated With Peripheral Corneal UlcerationDocument4 pagesSystemic Disorders Associated With Peripheral Corneal UlcerationYoga KharismaNo ratings yet
- Prasad 2012Document5 pagesPrasad 2012Gladys OliviaNo ratings yet
- Henter 2007Document8 pagesHenter 2007RaffaharianggaraNo ratings yet
- 02 NewhorizonsDocument8 pages02 NewhorizonsgloriaNo ratings yet
- Artritis SépticaDocument10 pagesArtritis SépticaCirugía General HUBUNo ratings yet
- Lecture Note of PathologyDocument73 pagesLecture Note of PathologyRafez JoneNo ratings yet
- The Classification of Glomerulonephritis in Systemic Lupus Erythematosus RevisitedDocument10 pagesThe Classification of Glomerulonephritis in Systemic Lupus Erythematosus RevisiteddionNo ratings yet
- Trauma Inflamatie Terapie Volemica F BunDocument19 pagesTrauma Inflamatie Terapie Volemica F BunCroitoru CosminNo ratings yet
- SIMI - Volume Comunicazioni Orali e PosterDocument212 pagesSIMI - Volume Comunicazioni Orali e Postermaria wahyuniNo ratings yet
- Potential Pathogenic Mechanisms Involved in The As PDFDocument8 pagesPotential Pathogenic Mechanisms Involved in The As PDFEndah KusumaNo ratings yet
- UK & KoagulasiDocument9 pagesUK & KoagulasiAnonymous 77IwVByMONo ratings yet
- Fetch ObjectDocument12 pagesFetch ObjectJoel FlosanNo ratings yet
- Clinical-Pathological Characteristics of Renal Injuries Identify Different Clusters in Patients With Antiphospholipid AntibodiesDocument10 pagesClinical-Pathological Characteristics of Renal Injuries Identify Different Clusters in Patients With Antiphospholipid AntibodiesMayra D' Wonka ToddNo ratings yet
- Tissue Damaging Toxins in Snake VenomsDocument17 pagesTissue Damaging Toxins in Snake Venomsandrés Felipe CepedaNo ratings yet
- Interest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportDocument4 pagesInterest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportIJAR JOURNALNo ratings yet
- Wang-Orlow2018 Article KeratosisPilarisAndItsSubtypesDocument25 pagesWang-Orlow2018 Article KeratosisPilarisAndItsSubtypesdaily of sinta fuNo ratings yet
- Levofloxacin-Induced Delirium Case ReportDocument3 pagesLevofloxacin-Induced Delirium Case ReportDastinAndreNo ratings yet
- Cellulitis: Current Insights Into Pathophysiology and Clinical ManagementDocument13 pagesCellulitis: Current Insights Into Pathophysiology and Clinical Managementtucto849915No ratings yet
- Lepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeDocument2 pagesLepromatous Leprosy in Erythema Nodosum Leprosum Reaction Mimicking Sweet's SyndromeAstri MelistriNo ratings yet
- Example Research Paper On LupusDocument8 pagesExample Research Paper On Lupuswhrkeculg100% (1)
- Rosacea Pathogen Es IsDocument10 pagesRosacea Pathogen Es IsAlien_42No ratings yet
- Thesis On Sickle Cell DiseaseDocument8 pagesThesis On Sickle Cell Diseaseafbtfukel100% (1)
- CC 9290Document12 pagesCC 9290elektifppra2022No ratings yet
- Cocaine and AncaDocument7 pagesCocaine and AncaSundar Ramanathan100% (1)
- The Histopathological Evaluation of Drug-Induced Liver InjuryDocument13 pagesThe Histopathological Evaluation of Drug-Induced Liver InjuryAnonymous 01bH8iNo ratings yet
- International Review of Experimental Pathology: Kidney DiseaseFrom EverandInternational Review of Experimental Pathology: Kidney DiseaseG. W. RichterRating: 5 out of 5 stars5/5 (1)
- Guided Reflection 2Document4 pagesGuided Reflection 2Summer SeedsNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet
- Mercury in The MistDocument2 pagesMercury in The MistAnand BhagwaniNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- Radam, Sandralane C., Journal ReviewDocument3 pagesRadam, Sandralane C., Journal ReviewSandralane C. RadamNo ratings yet
- TWC Final Settlement DocsDocument374 pagesTWC Final Settlement DocsTHROnlineNo ratings yet
- 11.0 - Safety in The Heat v3.0 EnglishDocument14 pages11.0 - Safety in The Heat v3.0 EnglishAnonymous hBBam1nNo ratings yet
- Careers Surrey 20181Document15 pagesCareers Surrey 20181Kevin_Nguyen117No ratings yet
- Multi-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseDocument28 pagesMulti-Omic Machine Learning Predictor of Breast Cancer Therapy ResponseSobek1789No ratings yet
- List of Beed Researchers 2 Semester SY 2020-2021 Beed-ADocument5 pagesList of Beed Researchers 2 Semester SY 2020-2021 Beed-AAndamin MalaNo ratings yet
- List of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atDocument2 pagesList of Mandatory Documents: Document Checklist For Medical Treatment Visa Forms Can Be Downloaded atAdegokeNo ratings yet
- Unit 1Document15 pagesUnit 1kunalNo ratings yet
- Persuasive Speech TextDocument2 pagesPersuasive Speech TextAnindya Azzahra0% (1)
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
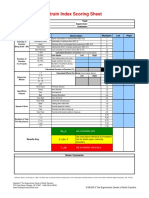
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- UKHO Survey Specification Acoustic V3 Jul18Document102 pagesUKHO Survey Specification Acoustic V3 Jul18Iqbal FauzanNo ratings yet
- DISC2-14071 AppealLetter PublicCommentsDocument17 pagesDISC2-14071 AppealLetter PublicCommentsJames ParsonsNo ratings yet
- PIL For Sudafed DecongestantDocument2 pagesPIL For Sudafed DecongestantOdunlamiNo ratings yet