You might also like
- Advanced Hypnosis Certification ManualDocument57 pagesAdvanced Hypnosis Certification ManualElita Purcille100% (3)
- Policy & Politics in Nursing and Health Ca - Diana J. MasonDocument1,650 pagesPolicy & Politics in Nursing and Health Ca - Diana J. MasonChristine Villamayor100% (15)
- 2021-07-01 Reader's Digest CanadaDocument118 pages2021-07-01 Reader's Digest CanadaAkil NohNo ratings yet
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocument213 pages2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNo ratings yet
- Non-Convulsive Status EpilepticusDocument17 pagesNon-Convulsive Status EpilepticusjossNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- GTG 17 PDFDocument18 pagesGTG 17 PDFFlorida RahmanNo ratings yet
- gtg60 Cervicalcerclage PDFDocument21 pagesgtg60 Cervicalcerclage PDFLijoeliyas100% (1)
- Ultrasound in Gynecology N ObstetricDocument9 pagesUltrasound in Gynecology N ObstetricKarthik RajvNo ratings yet
- Practice Bulletin No 144 Multifetal Gestations .40Document15 pagesPractice Bulletin No 144 Multifetal Gestations .40Jose Luis Morales Bautista100% (1)
- Cannulation Camp: Basic Needle Cannulation Training For Dialysis StaffDocument7 pagesCannulation Camp: Basic Needle Cannulation Training For Dialysis Staffcharlenetan18100% (3)
- Cave Rescue Assignment 1Document3 pagesCave Rescue Assignment 1ريناد جناديNo ratings yet
- Tubal Ectopic Pregnancy PB193Document13 pagesTubal Ectopic Pregnancy PB193Sheyla Orellana PurillaNo ratings yet
- Overview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateDocument27 pagesOverview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateRopiNo ratings yet
- Prediction of Preterm Delivery in Twins by Cervical Assessment at 23 WeeksDocument4 pagesPrediction of Preterm Delivery in Twins by Cervical Assessment at 23 WeeksBudi Darmawan DiswanNo ratings yet
- Desi Rahayu (153112540120468Document53 pagesDesi Rahayu (153112540120468Bella FebriyantiNo ratings yet
- Frequency of Uterine Contractions and The Risk of Spontaneous Preterm DeliveryDocument7 pagesFrequency of Uterine Contractions and The Risk of Spontaneous Preterm DeliveryiullNo ratings yet
- Yolk Sac Shape OutcomeDocument11 pagesYolk Sac Shape OutcomeSofyan QadriNo ratings yet
- 2.april 2020 Estimation of Risk Factors For MultiparousDocument4 pages2.april 2020 Estimation of Risk Factors For MultiparousTushar BahetiNo ratings yet
- Antenatal Betamethasone For Women at RiskDocument10 pagesAntenatal Betamethasone For Women at RiskThapakorn JalearnyingNo ratings yet
- Good18.Prenatally Diagnosed Vasa Previa A.30Document9 pagesGood18.Prenatally Diagnosed Vasa Previa A.30wije0% (1)
- Acog Practice Bulletin: Early Pregnancy LossDocument11 pagesAcog Practice Bulletin: Early Pregnancy LossAlberto Kenyo Riofrio PalaciosNo ratings yet
- Female Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001Document5 pagesFemale Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001International Journal of Innovative Science and Research TechnologyNo ratings yet
- Ijss Jan Oa25 - 2017Document4 pagesIjss Jan Oa25 - 2017Esther Ellise AbundoNo ratings yet
- The Role of Ultrasound in ObstetricsDocument9 pagesThe Role of Ultrasound in ObstetricsHanun FaizaNo ratings yet
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- The Role of Ultrasound in Obstetric and Gynaecology: Max Brinsmead PHD Franzcog May 2006Document9 pagesThe Role of Ultrasound in Obstetric and Gynaecology: Max Brinsmead PHD Franzcog May 2006alhassanmohamedNo ratings yet
- 140 140 1 PBDocument4 pages140 140 1 PBMina LelymanNo ratings yet
- Ultrasound in Prenatal DiagnosisDocument11 pagesUltrasound in Prenatal DiagnosisValentina Grajales RestrepoNo ratings yet
- SGABiophysical TestsDocument2 pagesSGABiophysical TestsalotfyaNo ratings yet
- Prolonged Pregnancy:When Should We Intervene?Document11 pagesProlonged Pregnancy:When Should We Intervene?Raul DoctoNo ratings yet
- Frederiksen 2018Document7 pagesFrederiksen 2018WinniaTanelyNo ratings yet
- Clinical Factors Affecting The Accuracy Of.15Document8 pagesClinical Factors Affecting The Accuracy Of.15naveen597No ratings yet
- Journal Ectopic Pregnancy-A Rising TrendDocument5 pagesJournal Ectopic Pregnancy-A Rising TrendEricNo ratings yet
- Routine Prenatal Ultrasonography As A Screening ToolDocument17 pagesRoutine Prenatal Ultrasonography As A Screening ToolYulia MufidahNo ratings yet
- Tubal Ectopic Pregnancy: (Replaces Practice Bulletin Number 191, February 2018)Document18 pagesTubal Ectopic Pregnancy: (Replaces Practice Bulletin Number 191, February 2018)Rubio Sanchez JuanNo ratings yet
- OBST aNALISIS-DE-LONGITUD-CERVICAL-Y-RIESGOYDocument6 pagesOBST aNALISIS-DE-LONGITUD-CERVICAL-Y-RIESGOYEduardo Agustín Vargas CamposNo ratings yet
- 03mb01 4Document3 pages03mb01 4matchman_headNo ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Late Termination of Pregnancy. Professional Dilemmas: Isack Kandel and Joav MerrickDocument11 pagesLate Termination of Pregnancy. Professional Dilemmas: Isack Kandel and Joav Merrickvyola chaniaNo ratings yet
- Role of Ultrasonography in Diagnosis of Ectopic Pregnancy With Clinical Analysis and Management in Tertiary Care HospitalDocument4 pagesRole of Ultrasonography in Diagnosis of Ectopic Pregnancy With Clinical Analysis and Management in Tertiary Care HospitalRizka AdiNo ratings yet
- Normal Lebih Baik Dari Sesar (Gemeli)Document4 pagesNormal Lebih Baik Dari Sesar (Gemeli)Juwita Valen RamadhanniaNo ratings yet
- Amnioinfusion Compared With No Intervention In.18Document8 pagesAmnioinfusion Compared With No Intervention In.18owadokunquick3154No ratings yet
- Poster Session II: Diabetes, Doppler, Labor, Ultrasound-ImagingDocument1 pagePoster Session II: Diabetes, Doppler, Labor, Ultrasound-ImagingRegina PizanNo ratings yet
- Week 5Document2 pagesWeek 5yannahlrNo ratings yet
- LK 1Document4 pagesLK 1SuciPurnamarzaNo ratings yet
- Sectio Pada Preeclampsia BeratDocument4 pagesSectio Pada Preeclampsia BeratJosepb SimarmataNo ratings yet
- Cervical Cerclage A Review of Current EvidenceDocument5 pagesCervical Cerclage A Review of Current EvidenceAnonymous LzJqA5d5EfNo ratings yet
- Predicting Cesarean Section AnDocument5 pagesPredicting Cesarean Section AnKEANNA ZURRIAGANo ratings yet
- 1 PDFDocument7 pages1 PDFAlfa FebriandaNo ratings yet
- C-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Document7 pagesC-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Aris SugiatnoNo ratings yet
- Jurnal KEDocument16 pagesJurnal KEMuhammad Harris ZainalNo ratings yet
- 2011 9 PDFDocument6 pages2011 9 PDFRamesh Kumar SNo ratings yet
- Cervical Length Measurement Using An Improvised Cervicometer As A Predictor of Spontaneous Preterm BirthDocument6 pagesCervical Length Measurement Using An Improvised Cervicometer As A Predictor of Spontaneous Preterm BirthImarie RamosNo ratings yet
- Sibai PDFDocument2 pagesSibai PDFAdriana PajueloNo ratings yet
- Nama: Zaimah Shalsabilla Kelas: Alpha NIM: 04011181520071Document11 pagesNama: Zaimah Shalsabilla Kelas: Alpha NIM: 04011181520071shalsaNo ratings yet
- Tubal Ectopic PregnancyDocument38 pagesTubal Ectopic Pregnancy6ixSideCreate MNo ratings yet
- OBST Prediction of Patient-Specific Risk of Early Preterm DeliveryDocument6 pagesOBST Prediction of Patient-Specific Risk of Early Preterm DeliveryEduardo Agustín Vargas CamposNo ratings yet
- Simcox 2009Document6 pagesSimcox 2009Aulya ArchuletaNo ratings yet
- Cap. 26Document6 pagesCap. 26Familia CieletNo ratings yet
- Study of Management in Patient With Ectopic Pregnancy: Key WordsDocument3 pagesStudy of Management in Patient With Ectopic Pregnancy: Key WordsparkfishyNo ratings yet
- Prediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery DopplerDocument6 pagesPrediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery Dopplerganesh reddyNo ratings yet
- Practic Buletin Early Pregnancy Loss PDFDocument10 pagesPractic Buletin Early Pregnancy Loss PDFsiantan ngebutNo ratings yet
- Term and Posterm PDFDocument7 pagesTerm and Posterm PDFRorschach VargasNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Epidemiology of Healthcare Associated Infection (HAI)Document58 pagesEpidemiology of Healthcare Associated Infection (HAI)Aan Dwi PrasetioNo ratings yet
- Jenis Kelamin Jenis Stroke Yang Diderita Pasien CrosstabulationDocument9 pagesJenis Kelamin Jenis Stroke Yang Diderita Pasien CrosstabulationAan Dwi PrasetioNo ratings yet
- Analysis of LED Value Projection On Clinical Improvement of Patients With Acute Ischemic StrokeDocument2 pagesAnalysis of LED Value Projection On Clinical Improvement of Patients With Acute Ischemic StrokeAan Dwi PrasetioNo ratings yet
- Seminar CNE 2018Document12 pagesSeminar CNE 2018Aan Dwi PrasetioNo ratings yet
- Bipolar Disorder in AdultDocument21 pagesBipolar Disorder in AdultAan Dwi PrasetioNo ratings yet
- Malignant Otitis Externa: Matthew J. Carfrae, MD, Bradley W. Kesser, MDDocument13 pagesMalignant Otitis Externa: Matthew J. Carfrae, MD, Bradley W. Kesser, MDAyuAnatrieraNo ratings yet
- Kangoroo Mother CareDocument15 pagesKangoroo Mother CareElok IslyonasariNo ratings yet
- Laporan PBL 4Document35 pagesLaporan PBL 4Adjest KingsCrown.No ratings yet
- LiveStock Jobs Advertisement 2022Document2 pagesLiveStock Jobs Advertisement 2022Sher ZamanNo ratings yet
- Agrarian Reform Policies HistoryDocument8 pagesAgrarian Reform Policies HistoryElla Marie MostralesNo ratings yet
- Fuel Tank Lifting REV01Document7 pagesFuel Tank Lifting REV01armagan55No ratings yet
- Renal Injuries: Penetrating and BluntDocument24 pagesRenal Injuries: Penetrating and BluntRhonda BushNo ratings yet
- Isoprenaline Infusion 2016Document3 pagesIsoprenaline Infusion 2016Glory Claudia KarundengNo ratings yet
- Love vs. Sexual Attraction: David Tian, PH.D., and Aura Transformation PresentDocument18 pagesLove vs. Sexual Attraction: David Tian, PH.D., and Aura Transformation PresentRicky KarmakarNo ratings yet
- Objective Test 1 - Ms Phuong - KEYDocument4 pagesObjective Test 1 - Ms Phuong - KEYHà AnhNo ratings yet
- Om 438906011 W365-3330H N M 2H01 enDocument24 pagesOm 438906011 W365-3330H N M 2H01 enAlejandro LeonNo ratings yet
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 pagesDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoNo ratings yet
- Viz. Sickness, Servants, Small Cattle, &C.: of The Sixth HouseDocument25 pagesViz. Sickness, Servants, Small Cattle, &C.: of The Sixth Housepanditrules100% (1)
- Axial Group H&S Profile 052019Document11 pagesAxial Group H&S Profile 052019Heramb TrifaleyNo ratings yet
- Journal of Gerontology & Geriatric ResearchDocument6 pagesJournal of Gerontology & Geriatric ResearchyuniaNo ratings yet
- CHN Midterm Long QuizDocument2 pagesCHN Midterm Long Quizkuma phNo ratings yet
- A Postgraduate Seminar On Shock CorrectedDocument69 pagesA Postgraduate Seminar On Shock Correctedboma georgeNo ratings yet
- Hubungan Motivasi Deteksi Dini Kanker Serviks Dengan Tindakan Pap Smear Pada Wanita Usia Subur Di Wilayah GonilanDocument7 pagesHubungan Motivasi Deteksi Dini Kanker Serviks Dengan Tindakan Pap Smear Pada Wanita Usia Subur Di Wilayah Gonilanevi yulia arvensiNo ratings yet
- PR 1Document10 pagesPR 1Trisha Kaye FloresNo ratings yet
- Nasal and Indoors Fungal Contamination in Healthy SubjectsDocument5 pagesNasal and Indoors Fungal Contamination in Healthy SubjectsAtlas CerboNo ratings yet
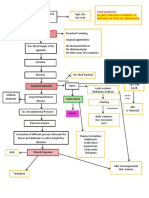
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- Clear Cell Acanthoma of The Mammary Region: A Case: Laporan Kasus Divisi TBKDocument12 pagesClear Cell Acanthoma of The Mammary Region: A Case: Laporan Kasus Divisi TBKJulian LeeNo ratings yet
- Leishmaniasis: Key FactsDocument6 pagesLeishmaniasis: Key FactsNurul Hikmah PratiwiNo ratings yet
- TH True Milk: Duy Tan UniversityDocument40 pagesTH True Milk: Duy Tan UniversityPi ĐôNo ratings yet