You might also like
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Dr. LitaDocument30 pagesDr. LitaIzka P RahmaniaNo ratings yet
- Injection JointDocument58 pagesInjection JointNghĩa Nguyễn TrọngNo ratings yet
- Anestesi Lokal Pada Lesi Superfisial: Huntal NapoleonDocument12 pagesAnestesi Lokal Pada Lesi Superfisial: Huntal NapoleonshevinesaNo ratings yet
- New Zealand Data Sheet: 1. Product NameDocument25 pagesNew Zealand Data Sheet: 1. Product Nameurfi85No ratings yet
- Local Anesthetic TechniquesDocument81 pagesLocal Anesthetic TechniquesMohanad BraziNo ratings yet
- Artrocenseis - Libro de Reumato en InglesDocument15 pagesArtrocenseis - Libro de Reumato en InglesPabloNo ratings yet
- Common Soft Tissue Problems of The Upper LimbDocument46 pagesCommon Soft Tissue Problems of The Upper LimbVaikunthan RajaratnamNo ratings yet
- Anestesi LokalDocument12 pagesAnestesi LokalKurniatiKhasanahQhafisaQurratul'ainNo ratings yet
- 14 InjectionDocument35 pages14 InjectionArismunandar SosiloNo ratings yet
- Joint and Soft Tissue Injection Guidelines PCRSDocument12 pagesJoint and Soft Tissue Injection Guidelines PCRSMartijn JohanNo ratings yet
- Knee Joint Inj and AspirationsDocument2 pagesKnee Joint Inj and AspirationsUmmu Nur FathonahNo ratings yet
- Local Anesthesia: Classification, Mechanism of Action, Complications and Recent AdvancementsDocument80 pagesLocal Anesthesia: Classification, Mechanism of Action, Complications and Recent AdvancementsRiya JainNo ratings yet
- Untitled PresentationDocument41 pagesUntitled PresentationOmar KojerNo ratings yet
- Regional Conditions of WristDocument54 pagesRegional Conditions of WristSreekar ReddyNo ratings yet
- Acute Wound CareDocument73 pagesAcute Wound CareDikaNo ratings yet
- 8-IM Injections 2Document21 pages8-IM Injections 2arlixNo ratings yet
- CM Extravasation: Signs, Risks, Prevention & TreatmentDocument19 pagesCM Extravasation: Signs, Risks, Prevention & Treatmentzainab sawanNo ratings yet
- PARENTERALS: ROUTES OF ADMINISTRATIONDocument158 pagesPARENTERALS: ROUTES OF ADMINISTRATIONJennifer Kierstine ChuaNo ratings yet
- L3General Principles of Periodontal Surgery LastDocument38 pagesL3General Principles of Periodontal Surgery LastHaneen Al-HajjNo ratings yet
- SURGERY OF THE EXTRAOCULAR MUSCLES: TECHNIQUES AND COMPLICATIONSDocument29 pagesSURGERY OF THE EXTRAOCULAR MUSCLES: TECHNIQUES AND COMPLICATIONSArdyNo ratings yet
- Open Fractures: DR Gourav RamukaDocument30 pagesOpen Fractures: DR Gourav RamukaGaurav Ramuka100% (1)
- Knee Joint AND Hip Joint PuncturesDocument13 pagesKnee Joint AND Hip Joint PuncturesTimbur IgorNo ratings yet
- Maxillary Techniques LecturesDocument151 pagesMaxillary Techniques Lecturespeter samaanNo ratings yet
- Maxillary Techniques LecturesDocument151 pagesMaxillary Techniques Lecturespeter samaanNo ratings yet
- Outline ReportDocument5 pagesOutline ReportRogerQuxNo ratings yet
- BOTOX Summary for Injection PowderDocument40 pagesBOTOX Summary for Injection PowderpsdsportsdocNo ratings yet
- AmeenaDocument10 pagesAmeenaCH SaddamNo ratings yet
- Open FractureDocument106 pagesOpen FractureNizwan ShamNo ratings yet
- IMI'sDocument6 pagesIMI'sanitha lakshminarayanaNo ratings yet
- Pwritten Report Id Im SCDocument17 pagesPwritten Report Id Im SCPauleen Gail LinsanganNo ratings yet
- C 15 ParenteralsDocument158 pagesC 15 ParenteralsRizzalaine CaringalNo ratings yet
- Injection TechniquesDocument11 pagesInjection TechniquesLeon OngNo ratings yet
- Recent Advances in OtorhinolaryngologyDocument22 pagesRecent Advances in OtorhinolaryngologyInderdeep Arora100% (1)
- Tourniquet Mahyudin, DRDocument44 pagesTourniquet Mahyudin, DRyudi tikaNo ratings yet
- Orthopedic Study GuideDocument17 pagesOrthopedic Study GuideD'Arby Janelle SmithNo ratings yet
- Lecture 7Document37 pagesLecture 7Dr. Rabail MalikNo ratings yet
- Oral SurgeryDocument40 pagesOral Surgeryshekinah echavezNo ratings yet
- Chronic venous insufficiency clinical presentation and treatmentDocument3 pagesChronic venous insufficiency clinical presentation and treatmentAlex Andrés Cuevas UrriolaNo ratings yet
- Local Complication Dea EdaitDocument21 pagesLocal Complication Dea Edaitمحمد ربيعيNo ratings yet
- Dry NeedlingDocument7 pagesDry NeedlingSalsabeel SalamahNo ratings yet
- Assessment and management of pressure soresDocument19 pagesAssessment and management of pressure soresugandanursingschool bwindi100% (1)
- Varicose Vein TreatmentDocument22 pagesVaricose Vein TreatmentRavi GuptaNo ratings yet
- Tic BookDocument19 pagesTic BookPersis NairNo ratings yet
- Treating Onychomycosis, Intermittent Claudication, Dermatitis, Charcot Arthropathy, Trophic UlcersDocument9 pagesTreating Onychomycosis, Intermittent Claudication, Dermatitis, Charcot Arthropathy, Trophic UlcersJairah CandaoNo ratings yet
- Compartment Syndrome of HandDocument29 pagesCompartment Syndrome of HandAdi KayanaNo ratings yet
- Arthritis CmeDocument13 pagesArthritis CmeBigabwa BernardNo ratings yet
- J S T A I (A) : Oint and Oft Issue Spiration and Njection RthrocentesisDocument19 pagesJ S T A I (A) : Oint and Oft Issue Spiration and Njection RthrocentesisSgantzos MarkosNo ratings yet
- opthalmologyDocument17 pagesopthalmologyKishan S GowdaNo ratings yet
- A) - Provisional Diagnosis For This PTDocument4 pagesA) - Provisional Diagnosis For This PTanees jamalNo ratings yet
- Minor - Surgery UpdateDocument3 pagesMinor - Surgery UpdateHemkerovner Keresztszegh von Kolowrat-KrakowskyNo ratings yet
- Trigger Finger Aug 2020 v5Document2 pagesTrigger Finger Aug 2020 v5Anne SerneoNo ratings yet
- Epicondylitis Cyriax Physiotherapy For Tennis Elbow/lateral: Br. J. Sports MedDocument4 pagesEpicondylitis Cyriax Physiotherapy For Tennis Elbow/lateral: Br. J. Sports MedJohana Huichaqueo CurinNo ratings yet
- Oral Surgery & Pain Managment 13-14Document175 pagesOral Surgery & Pain Managment 13-14Priya SargunanNo ratings yet
- Snake Bites NotesDocument22 pagesSnake Bites NotesgosegomangNo ratings yet
- Total Contact Cast Application: Ihsan Oesman, MD University of Indonesia Cipto Mangunkusumo HospitalDocument15 pagesTotal Contact Cast Application: Ihsan Oesman, MD University of Indonesia Cipto Mangunkusumo HospitalCheh FamsNo ratings yet
- Standard Operating Procedure IM RouteDocument17 pagesStandard Operating Procedure IM RouteSAQUIB HASSANNo ratings yet
- Angioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAngioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Laser Surgery For The Spine. A Pin Hole Appraoch.Document2 pagesLaser Surgery For The Spine. A Pin Hole Appraoch.Achmad Harun MuchsinNo ratings yet
- Artis Zee Brochure PDFDocument40 pagesArtis Zee Brochure PDFAchmad Harun MuchsinNo ratings yet
- Laser Surgery For The Spine. A Pin Hole Appraoch.Document2 pagesLaser Surgery For The Spine. A Pin Hole Appraoch.Achmad Harun MuchsinNo ratings yet
- Neuropathic Pain Colloca2017Document19 pagesNeuropathic Pain Colloca2017Achmad Harun MuchsinNo ratings yet
- Steroid Flare Reaction A Complication of Intraarticular Steroid Injection1Document4 pagesSteroid Flare Reaction A Complication of Intraarticular Steroid Injection1Achmad Harun MuchsinNo ratings yet
- Pituitary Tumors Engleza 2Document89 pagesPituitary Tumors Engleza 2Achmad Harun MuchsinNo ratings yet
- Cancer PainDocument4 pagesCancer PainAchmad Harun MuchsinNo ratings yet
- Clinical Evaluation of Melladerm Plus A Honey Based GelDocument7 pagesClinical Evaluation of Melladerm Plus A Honey Based GelAchmad Harun MuchsinNo ratings yet
- Synovial Fluid Analysis Reveals PseudogoutDocument31 pagesSynovial Fluid Analysis Reveals PseudogoutAchmad Harun MuchsinNo ratings yet
- Immunosuppressed Patients C Immunosuppressed-Patients-Clinical-Pathway - Pdflinical PathwayDocument2 pagesImmunosuppressed Patients C Immunosuppressed-Patients-Clinical-Pathway - Pdflinical PathwayAchmad Harun MuchsinNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Jurnalku DUDocument5 pagesJurnalku DUAchmad Harun MuchsinNo ratings yet
- Cuijpers (2008) Psychological Treatment of Depression A Meta-Analytic Database ofDocument6 pagesCuijpers (2008) Psychological Treatment of Depression A Meta-Analytic Database ofThamara Tapia-MunozNo ratings yet
- CT Bowel WallDocument12 pagesCT Bowel WallBrian LucasNo ratings yet
- Midwifery Pharmacology-7Document1 pageMidwifery Pharmacology-7georgeloto12No ratings yet
- Time Table Panitia - NewDocument3 pagesTime Table Panitia - NewcelinNo ratings yet
- Ruqyah Instructions and Symptoms: Symptoms of Evil EyeDocument2 pagesRuqyah Instructions and Symptoms: Symptoms of Evil Eyeempty_shake5319100% (1)
- Dr. G. M. Taori: Curriculum VitaeDocument12 pagesDr. G. M. Taori: Curriculum Vitaesrajan sahuNo ratings yet
- Drinking Water and Losing WeightDocument3 pagesDrinking Water and Losing WeightMathana SuriaNo ratings yet
- Fillable Anesthesia SheetDocument2 pagesFillable Anesthesia Sheetetchemendyvet70790% (1)
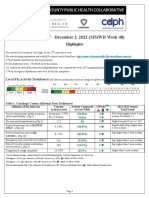
- 2022-23 Flu Surveillance Report - Week 48Document5 pages2022-23 Flu Surveillance Report - Week 48WKYC.comNo ratings yet
- Lession 1Document99 pagesLession 1BHUKYA USHARANINo ratings yet
- Rood Approach to Muscle Re-educationDocument33 pagesRood Approach to Muscle Re-educationRicha SoodNo ratings yet
- 01 Drug File MHNDocument29 pages01 Drug File MHNamit85% (13)
- Consensus ETON 1Document7 pagesConsensus ETON 1satyagraha84No ratings yet
- 01 - Introduction To DentistryDocument18 pages01 - Introduction To Dentistrymichal ben meronNo ratings yet
- ACUSON Antares Premium Edition BrochureDocument12 pagesACUSON Antares Premium Edition BrochureRanieh Al-Khatib100% (1)
- Critical Care NursingDocument12 pagesCritical Care NursingMoni Mbumba MelekeNo ratings yet
- Estradiol As Hemihydrate 3.2mg (Evorel - 50)Document20 pagesEstradiol As Hemihydrate 3.2mg (Evorel - 50)ddandan_2No ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet
- Pathologt of The HeartDocument40 pagesPathologt of The HeartJudithNo ratings yet
- Crown LengtheningDocument4 pagesCrown LengtheningArdelvie YoandaNo ratings yet
- Clinical Report of DR. Md. Murshidul Ahsan On E.coli & SalmonellaDocument51 pagesClinical Report of DR. Md. Murshidul Ahsan On E.coli & SalmonellamurshidvetNo ratings yet
- Reca Op Claim Form 12-11-0Document25 pagesReca Op Claim Form 12-11-0Ehren OertellNo ratings yet
- MCQ exam on pharmacology, medicine and treatmentsDocument10 pagesMCQ exam on pharmacology, medicine and treatmentsعزالدين الطيارNo ratings yet
- Skilled Birth Attendant Neonatal Resuscitation Training ProgramDocument48 pagesSkilled Birth Attendant Neonatal Resuscitation Training ProgramPradeep VermaNo ratings yet
- Lyme Disease InterventionsDocument3 pagesLyme Disease InterventionsahiNo ratings yet
- Prostate cancer differential diagnosis and key considerationsDocument4 pagesProstate cancer differential diagnosis and key considerationsRobert StolnicuNo ratings yet
- Pflipsen Anaphylaxis Recognition and ManagementDocument10 pagesPflipsen Anaphylaxis Recognition and ManagementOlivia McCuskerNo ratings yet
- RabiesDocument5 pagesRabiesutsav ashishNo ratings yet
- Deep Fungal InfectionsDocument33 pagesDeep Fungal Infectionstummalapalli venkateswara raoNo ratings yet
- Drugs Used in Disorders of CoagulationDocument6 pagesDrugs Used in Disorders of CoagulationAimee Redor100% (1)