You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Daily Vagus Nerve Exercises A Self-Help G - Sherman SanderDocument90 pagesDaily Vagus Nerve Exercises A Self-Help G - Sherman Sanderscriberone100% (6)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Vitamin D3Document29 pagesVitamin D3Ambreen AmirNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Research Methodology and Medical Statistic Index and Sample Chapters PDFDocument21 pagesResearch Methodology and Medical Statistic Index and Sample Chapters PDFCHAUKHAMBHA PRAKASHAK50% (2)
- Will Maclean - Clinical Handbook of Chinese Herbs - Desk Reference, Revised Edition-Singing Dragon (2017)Document170 pagesWill Maclean - Clinical Handbook of Chinese Herbs - Desk Reference, Revised Edition-Singing Dragon (2017)amitlkoyogaNo ratings yet
- ATLS ProtocoloDocument21 pagesATLS Protocoloedgarjavier65100% (2)
- ATLSPracticeTest3 PDFDocument10 pagesATLSPracticeTest3 PDFRodrigo Sanjines75% (4)
- Oman-Guideline On Good Pharmacovigilance PracticesDocument30 pagesOman-Guideline On Good Pharmacovigilance PracticesAmrNo ratings yet
- Arterial Line and Central LineDocument32 pagesArterial Line and Central LineOrachorn AimarreeratNo ratings yet
- Listening Sample Test 2 Answer KeyDocument3 pagesListening Sample Test 2 Answer KeyRihab IsmaeelNo ratings yet
- Algorithm For The Treatment of Malaria in AdultsDocument1 pageAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNo ratings yet
- Hipertensi KrisisDocument30 pagesHipertensi KrisisLuthfan HakimNo ratings yet
- Ectoparasites Killed by Kle and Nco Soap: Kakawate (Gliricidia Sepium) LeafDocument2 pagesEctoparasites Killed by Kle and Nco Soap: Kakawate (Gliricidia Sepium) LeafRyan Bacarro BagayanNo ratings yet
- Case SheetDocument23 pagesCase SheetMuhammad SdiqNo ratings yet
- Oral Lichen PlanusDocument28 pagesOral Lichen PlanusParul SinghNo ratings yet
- E-Book C Arms-NewDocument9 pagesE-Book C Arms-NewHugoNo ratings yet
- Diabetes MellitusDocument8 pagesDiabetes MellitusJaja RamosNo ratings yet
- A Slice O F: MMR EditionDocument20 pagesA Slice O F: MMR EditionTomTomNo ratings yet
- Guia de Productos PDFDocument32 pagesGuia de Productos PDFJulio Cesar Ramirez OlaveNo ratings yet
- BPUDDocument26 pagesBPUDIvanNo ratings yet
- Barium MealDocument12 pagesBarium Mealbagasaditya480No ratings yet
- Revised Thesis Alternative SupplementsDocument40 pagesRevised Thesis Alternative Supplementsgiogiogio17No ratings yet
- Concept MapDocument1 pageConcept MapYalante BellNo ratings yet
- Novilyn C. Pataray BSN - Ii Otitis Media: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Otitis Media: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- SEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFDocument95 pagesSEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFuzairNo ratings yet
- Star Smiley 2007Document343 pagesStar Smiley 2007David Ajibade100% (1)
- Tugas Kelompok - Menganalisis Jurnal - Meet 3 - Kelompok 3Document4 pagesTugas Kelompok - Menganalisis Jurnal - Meet 3 - Kelompok 3Rizki HandayaniNo ratings yet
- Central Bank Vs CSCDocument6 pagesCentral Bank Vs CSCRonn PagcoNo ratings yet
- Catalog Tracoe 2014 PDFDocument94 pagesCatalog Tracoe 2014 PDFLiudmila RailescuNo ratings yet
- Cleveland Clinic and Hebrew University: A Virtual Partnership To Redefine Nanotechnology?Document10 pagesCleveland Clinic and Hebrew University: A Virtual Partnership To Redefine Nanotechnology?kirtiNo ratings yet
- Pathologist Job SpecificationDocument16 pagesPathologist Job SpecificationLalaluluNo ratings yet
- CSOMDocument29 pagesCSOMsuciNo ratings yet
- New Oakland Summer Day ProgramDocument2 pagesNew Oakland Summer Day Programapi-215085793No ratings yet
- Lab 7 NewDocument3 pagesLab 7 New202010187No ratings yet
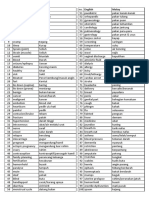
- Medic Term English MalayDocument1 pageMedic Term English MalaySyamimi SuhaimiNo ratings yet