You might also like
- Prevention of Dental Caries: A Review of Effective TreatmentsDocument7 pagesPrevention of Dental Caries: A Review of Effective TreatmentsJuan José Ignacio Narvaez FischerNo ratings yet
- Fluoride Toothpaste Prevents Caries in Children and Adolescents at Fluoride Concentrations of 1000 PPM and AboveDocument2 pagesFluoride Toothpaste Prevents Caries in Children and Adolescents at Fluoride Concentrations of 1000 PPM and AboveEnrique Ignacio Tejeda MeloNo ratings yet
- Taf PDFDocument14 pagesTaf PDFrania azzahraNo ratings yet
- 1063 FullDocument10 pages1063 FullJavier Farias VeraNo ratings yet
- Systematic Review of Controlled Trials On The Effectiveness of Fluoride Gels For The Prevention of Dental Caries in ChildrenDocument11 pagesSystematic Review of Controlled Trials On The Effectiveness of Fluoride Gels For The Prevention of Dental Caries in ChildrenJavangula Tripura PavitraNo ratings yet
- Comm Dent Oral Epid - 2017 - SteinDocument8 pagesComm Dent Oral Epid - 2017 - SteinSherienNo ratings yet
- Evidence-Based Clinical Recommendations For Fluoride Use: A ReviewDocument6 pagesEvidence-Based Clinical Recommendations For Fluoride Use: A ReviewshafanabilahNo ratings yet
- Fluoride Mouthrinses For Preventing Dental Caries in Children and AdolescentsDocument2 pagesFluoride Mouthrinses For Preventing Dental Caries in Children and AdolescentsRhena Fitria KhairunnisaNo ratings yet
- 2022 Article 2086Document11 pages2022 Article 2086gbaez.88No ratings yet
- Linking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Document5 pagesLinking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Ana CernaianuNo ratings yet
- EAPDDocument20 pagesEAPDNishant MehtaNo ratings yet
- Linking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Document6 pagesLinking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Catalina VenegasNo ratings yet
- Fluoride Toothpastes of Different Concentrations For Preventing Dental CariesDocument3 pagesFluoride Toothpastes of Different Concentrations For Preventing Dental CariesMarita JiménezNo ratings yet
- Professionally Applied Topical FluoridesDocument13 pagesProfessionally Applied Topical FluoridesHan Sung HyoNo ratings yet
- TurmericDocument4 pagesTurmericEllizabeth LilantiNo ratings yet
- Dehghan IDocument7 pagesDehghan IincisivusNo ratings yet
- GJHS 8 211Document6 pagesGJHS 8 211Susi SimangunsongNo ratings yet
- JC 4Document29 pagesJC 4rahafalqadi1No ratings yet
- Sealants For Preventing Dental Decay in The Permanent Teeth (Review)Document4 pagesSealants For Preventing Dental Decay in The Permanent Teeth (Review)براءة أحمد السلاماتNo ratings yet
- Factores de Riesgo de CariesDocument10 pagesFactores de Riesgo de CariesKarla González GNo ratings yet
- Efficacy of Dental Floss and Chlorhexidine Mouth Rinse As An Adjunct To Toothbrushing in Removing Plaque and Gingival InflammationDocument8 pagesEfficacy of Dental Floss and Chlorhexidine Mouth Rinse As An Adjunct To Toothbrushing in Removing Plaque and Gingival Inflammationflavia_pop_12No ratings yet
- Carranza 2020Document40 pagesCarranza 2020Soo SoniNo ratings yet
- Clinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-AnalysisDocument33 pagesClinical E Oral-Health Promotion in Dental Caries Prevention Among Children: Systematic Review and Meta-Analysisnadia syestiNo ratings yet
- Martini 2021Document17 pagesMartini 2021Matheus JacobinaNo ratings yet
- Role of Chlorhexidine in Caries PreventionDocument7 pagesRole of Chlorhexidine in Caries PreventionHarry ArdiyantoNo ratings yet
- Oral Care in Ventilation MechanicDocument8 pagesOral Care in Ventilation MechanicRusida LiyaniNo ratings yet
- Editorial June 2016Document3 pagesEditorial June 2016Risha faricha NabilaNo ratings yet
- Clinical Effectiveness and Cost-Effectiveness of Fissure Sealants in Children and Adolescents With A High Caries RiskDocument9 pagesClinical Effectiveness and Cost-Effectiveness of Fissure Sealants in Children and Adolescents With A High Caries RiskAstri Ggamjong Xiao LuNo ratings yet
- Acta Odontologica Scandinavica: Shweta Sharda, Arpit Gupta, Ashima Goyal & Krishan GaubaDocument17 pagesActa Odontologica Scandinavica: Shweta Sharda, Arpit Gupta, Ashima Goyal & Krishan GaubaAnonymous tIwg2AyNo ratings yet
- Pharmacology Literature ReviewDocument7 pagesPharmacology Literature Reviewapi-703336450No ratings yet
- Etiologies and Treatments of Odontogenic Maxillary Sinusitis: A Systematic ReviewDocument7 pagesEtiologies and Treatments of Odontogenic Maxillary Sinusitis: A Systematic ReviewMuhammad Octa PernadiNo ratings yet
- G EBD Sealants1Document17 pagesG EBD Sealants1Naviatul UlfaNo ratings yet
- Are Combined Bleaching Techniques Better Than Their Sole Application? A Systematic Review and Meta-AnalysisDocument17 pagesAre Combined Bleaching Techniques Better Than Their Sole Application? A Systematic Review and Meta-Analysisgerson fabian arangoNo ratings yet
- 4 CHX Comparison BestDocument6 pages4 CHX Comparison BestWilliam LovellNo ratings yet
- Evidence-Based Clinical Practice Guideline For The Use of Pit-and-Fissure SealantsDocument17 pagesEvidence-Based Clinical Practice Guideline For The Use of Pit-and-Fissure Sealantsnona aryanNo ratings yet
- Tooth-Bleaching: A Review of The Efficacy and Adverse Effects of Various Tooth Whitening ProductsDocument6 pagesTooth-Bleaching: A Review of The Efficacy and Adverse Effects of Various Tooth Whitening ProductsMuhammad AbazaNo ratings yet
- Fluoride Knowledge Among Texas DentistsDocument6 pagesFluoride Knowledge Among Texas Dentistscarmen mendo hernandezNo ratings yet
- Evidence-Based Guide to Pit-and-Fissure Sealants Prevents Tooth DecayDocument17 pagesEvidence-Based Guide to Pit-and-Fissure Sealants Prevents Tooth DecayMarthaNo ratings yet
- 41 ST JC - SindhuDocument8 pages41 ST JC - SindhuDadi SindhuNo ratings yet
- The Effect of Listerine Mouthwash On Dental Plaque Gingival Inflammation and C Reactive Protein CRP 2161 1122.1000191Document5 pagesThe Effect of Listerine Mouthwash On Dental Plaque Gingival Inflammation and C Reactive Protein CRP 2161 1122.1000191Bagus RahmawanNo ratings yet
- Efectos AdversosDocument10 pagesEfectos Adversosjeimmy dulceyNo ratings yet
- Polak Et Al-2015-Journal of Clinical Periodontology PDFDocument13 pagesPolak Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- 11th JC - SINDHUDocument22 pages11th JC - SINDHUDadi SindhuNo ratings yet
- Caries-Preventive Effect of Glass Ionomer and Resin-Based Fissure Sealants On Permanent Teeth: A Meta AnalysisDocument0 pagesCaries-Preventive Effect of Glass Ionomer and Resin-Based Fissure Sealants On Permanent Teeth: A Meta AnalysisPascalis Adhi KurniawanNo ratings yet
- 7123 Waterpik IrrigationDocument5 pages7123 Waterpik IrrigationvianbulanNo ratings yet
- The Rational Use of Fluoride ToothpasteDocument6 pagesThe Rational Use of Fluoride ToothpasteDeaa IndiraNo ratings yet
- Comprehensive review of new caries assessment systemsDocument2 pagesComprehensive review of new caries assessment systemsSOMVIR KUMARNo ratings yet
- Effectiveness of Herbal and Non-Herbal Toothpastes in Reducing Dental Plaque AccumulationDocument5 pagesEffectiveness of Herbal and Non-Herbal Toothpastes in Reducing Dental Plaque AccumulationMuhammad SubhiNo ratings yet
- The First Permanent Molar Most Affected by Dental Caries - A Longitudinal StudyDocument6 pagesThe First Permanent Molar Most Affected by Dental Caries - A Longitudinal StudyQuęęn MirianeNo ratings yet
- Pit and Fissure Sealants in High Caries Risk IndividualsDocument25 pagesPit and Fissure Sealants in High Caries Risk IndividualsRisana RahoofNo ratings yet
- What Concentration of Fluoride Toothpaste Should Dental Teams Be RecommendingDocument2 pagesWhat Concentration of Fluoride Toothpaste Should Dental Teams Be RecommendingFărcășanu Maria-AndreeaNo ratings yet
- Advancing Infection Control in Dental Care SettingDocument12 pagesAdvancing Infection Control in Dental Care SettingEndang SetiowatiNo ratings yet
- JadaDocument14 pagesJadaadambear213No ratings yet
- Topical Fluorides in Caries Prevention and Management: A North American PerspectiveDocument6 pagesTopical Fluorides in Caries Prevention and Management: A North American PerspectivecsryderNo ratings yet
- Angela M Berry 2011Document6 pagesAngela M Berry 2011M Farid AzNo ratings yet
- Ecc Lit Review - PDocument7 pagesEcc Lit Review - Papi-720438286No ratings yet
- The Use of Prophylactic Antibiotics Prior To Dental Procedures in Patients With Prosthetic JointsDocument14 pagesThe Use of Prophylactic Antibiotics Prior To Dental Procedures in Patients With Prosthetic JointsalikaNo ratings yet
- Art Op 1Document12 pagesArt Op 1carolinagtzpNo ratings yet
- Management of Deep Carious LesionsFrom EverandManagement of Deep Carious LesionsFalk SchwendickeNo ratings yet
- Dentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthFrom EverandDentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthNo ratings yet
- Space Maintainer Treatment in Premature Loss Deciduous ToothDocument12 pagesSpace Maintainer Treatment in Premature Loss Deciduous ToothbanyubiruNo ratings yet
- Abu GosokDocument5 pagesAbu Gosokninda sekar ayuNo ratings yet
- (Journal) Anastesi BlockDocument8 pages(Journal) Anastesi Blockninda sekar ayuNo ratings yet
- (Journal) NanomedicinesDocument27 pages(Journal) Nanomedicinesninda sekar ayuNo ratings yet
- Nano-Crystalline Hydroxyapatite Bone Graft Combined With Bioresorbable Collagen Membrane in The Treatment of PeriodontaDocument13 pagesNano-Crystalline Hydroxyapatite Bone Graft Combined With Bioresorbable Collagen Membrane in The Treatment of Periodontaninda sekar ayuNo ratings yet
- The Oz DietDocument5 pagesThe Oz Dietkaren_wilkesNo ratings yet
- Sesame Seed: T. Y. Tunde-Akintunde, M. O. Oke and B. O. AkintundeDocument20 pagesSesame Seed: T. Y. Tunde-Akintunde, M. O. Oke and B. O. Akintundemarvellous ogbonnaNo ratings yet
- Unit 1 Advanced WordDocument115 pagesUnit 1 Advanced WordJorenn_AyersNo ratings yet
- VALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10Document6 pagesVALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10allyvluvyNo ratings yet
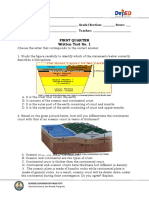
- Written Work 1 Q1 Science 10Document6 pagesWritten Work 1 Q1 Science 10JOEL MONTERDENo ratings yet
- Policy Based Routing On Fortigate FirewallDocument2 pagesPolicy Based Routing On Fortigate FirewalldanNo ratings yet
- Performance Theory For Hot Air Balloons: The Balloon Works, Inc., Statesville, N.CDocument4 pagesPerformance Theory For Hot Air Balloons: The Balloon Works, Inc., Statesville, N.CEbubekir ErkanNo ratings yet
- SMEspdfDocument13 pagesSMEspdflilpumpdidnothingwrong dNo ratings yet
- Wiring Diagram Obp 1 v2Document5 pagesWiring Diagram Obp 1 v2Jorge Luis Vera AlmeidaNo ratings yet
- Engineers Guide To Microchip 2018Document36 pagesEngineers Guide To Microchip 2018mulleraf100% (1)
- OUM Human Anatomy Final Exam QuestionsDocument5 pagesOUM Human Anatomy Final Exam QuestionsAnandNo ratings yet
- The Merchant of Venice QuestionsDocument9 pagesThe Merchant of Venice QuestionsHaranath Babu50% (4)
- What Is The Time Value of MoneyDocument6 pagesWhat Is The Time Value of MoneySadia JuiNo ratings yet
- Flex Id Driver Install InstructionsDocument24 pagesFlex Id Driver Install InstructionskingdiamondNo ratings yet
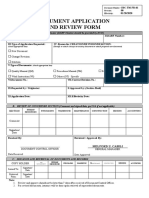
- Document Application and Review FormDocument1 pageDocument Application and Review FormJonnel CatadmanNo ratings yet
- Tax 1Document351 pagesTax 1AbbyNo ratings yet
- Spreadsheet and Presentation Skills SyllabusDocument4 pagesSpreadsheet and Presentation Skills SyllabusGbox CTCNo ratings yet
- 6 Fsiqiatria-1524041346Document48 pages6 Fsiqiatria-1524041346მირანდა გიორგაშვილიNo ratings yet
- Forms of WillsDocument24 pagesForms of WillsJasNo ratings yet
- Make Money OnlineDocument9 pagesMake Money OnlineTimiNo ratings yet
- UITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioDocument9 pagesUITM Faculty of Business Entrepreneurship Rubric Social Media PortfolioShamsyul AriffinNo ratings yet
- PT JayatamaDocument67 pagesPT JayatamaAminadap. SIL.TNo ratings yet
- 41 Programmer Isp RT809F PDFDocument3 pages41 Programmer Isp RT809F PDFArunasalam ShanmugamNo ratings yet
- Smith Bell v. Sotello MattiDocument3 pagesSmith Bell v. Sotello MattijrvyeeNo ratings yet
- Geraldez Vs Ca 230 Scra 329Document12 pagesGeraldez Vs Ca 230 Scra 329Cyrus Pural EboñaNo ratings yet
- g6 Sws ArgDocument5 pagesg6 Sws Argapi-202727113No ratings yet
- Perlman Janice, The Myth of Marginality RevisitDocument36 pagesPerlman Janice, The Myth of Marginality RevisitLuisa F. RodriguezNo ratings yet
- Ume Mri GuideDocument1 pageUme Mri GuideHiba AhmedNo ratings yet
- Kim Hoff PAR 117 JDF 1115 Separation AgreementDocument9 pagesKim Hoff PAR 117 JDF 1115 Separation AgreementlegalparaeagleNo ratings yet
- DepEd Memorandum on SHS Curriculum MappingDocument8 pagesDepEd Memorandum on SHS Curriculum MappingMichevelli RiveraNo ratings yet