You might also like
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySri HariNo ratings yet
- New Immunomodulatory Treatment For Infertile Men With AntispermDocument2 pagesNew Immunomodulatory Treatment For Infertile Men With AntispermIvan BubanovicNo ratings yet
- Hard Arson 2008Document7 pagesHard Arson 2008elda zulkarnainNo ratings yet
- Frozen-Thawed Embryo Transfer Cycles Have A Lower Incidence of Ectopic Pregnancy Compared With Fresh Embryo Transfer CyclesDocument5 pagesFrozen-Thawed Embryo Transfer Cycles Have A Lower Incidence of Ectopic Pregnancy Compared With Fresh Embryo Transfer CyclesPetru CernatNo ratings yet
- Live Birth After Transfer of A Single Euploid Vitrified-Warmed Blastocyst According To Standard Timing vs. Timing As Recommended by Endometrial Receptivity AnalysisDocument8 pagesLive Birth After Transfer of A Single Euploid Vitrified-Warmed Blastocyst According To Standard Timing vs. Timing As Recommended by Endometrial Receptivity AnalysisAnh Vũ Hồ NgọcNo ratings yet
- IVF RelatedDocument1 pageIVF RelatedMeera Al AliNo ratings yet
- Review ArticleDocument11 pagesReview ArticlealfiantiNo ratings yet
- 2007.NEJM - in Vitro Fertilization With Preimplantation Genetic ScreeningDocument9 pages2007.NEJM - in Vitro Fertilization With Preimplantation Genetic Screeningrpina.genNo ratings yet
- The Clinical Efficacy of Personalized Embryo Transfer Guided by The Endometrial Receptivity Array: Analysis On IVF:ICSI Outcomes: A Systematic Review and Meta-AnalysisDocument13 pagesThe Clinical Efficacy of Personalized Embryo Transfer Guided by The Endometrial Receptivity Array: Analysis On IVF:ICSI Outcomes: A Systematic Review and Meta-AnalysisAnh Vũ Hồ NgọcNo ratings yet
- Raja EA-2022Document12 pagesRaja EA-2022HAVIZ YUADNo ratings yet
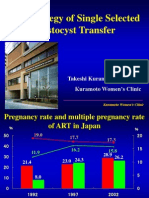
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDocument43 pagesThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiNo ratings yet
- 1 s2.0 S1472648322004291 MainDocument9 pages1 s2.0 S1472648322004291 Main周保亨No ratings yet
- Preimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesDocument5 pagesPreimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesAkmilia VeraNo ratings yet
- The Utility of Embryo Banking in Order To IncreaseDocument6 pagesThe Utility of Embryo Banking in Order To Increaselaura122334No ratings yet
- 5 PGS提高高龄人群的植入率和活产率Document11 pages5 PGS提高高龄人群的植入率和活产率zjuwindNo ratings yet
- Jurnal 8Document4 pagesJurnal 8Yoan YasrilNo ratings yet
- Pi Is 0015028207027598Document2 pagesPi Is 0015028207027598Ferry DimyatiNo ratings yet
- Impact of Paternal Age On EmbryologyDocument7 pagesImpact of Paternal Age On EmbryologyMạc Đình Cẩm TúNo ratings yet
- 2018 Article 432Document8 pages2018 Article 432Hartanto LieNo ratings yet
- 2020 HawkeDocument16 pages2020 Hawke99ornelaNo ratings yet
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- Biologia de La Reproduccion 1Document5 pagesBiologia de La Reproduccion 1Annette ChavezNo ratings yet
- The Preterm Labor Index and Fetal Fibronectin For.24Document6 pagesThe Preterm Labor Index and Fetal Fibronectin For.24bombonlrNo ratings yet
- Zhang 2019Document9 pagesZhang 2019Maria José MendiolaNo ratings yet
- 1 META分析 改善IVF临床结局Document21 pages1 META分析 改善IVF临床结局zjuwindNo ratings yet
- Hal 97Document8 pagesHal 97William OmarNo ratings yet
- Día Transfer. Labarta 1Document6 pagesDía Transfer. Labarta 1AnaNo ratings yet
- Infant Outcome After Complete Uterine RuptureDocument8 pagesInfant Outcome After Complete Uterine RuptureHeiddy Ch SumampouwNo ratings yet
- Am J Perinatol. 2007 Jun24 (6) 373-6Document4 pagesAm J Perinatol. 2007 Jun24 (6) 373-6Ivan Osorio RuizNo ratings yet
- Vaginal Delivery of TwinsDocument63 pagesVaginal Delivery of Twinsrake sardevaNo ratings yet
- Jorgensen 2007Document17 pagesJorgensen 2007Vanessa TavaresNo ratings yet
- To Determine The Pregnancy Outcomes in Patients With Previous Spontaneous AbortionsDocument13 pagesTo Determine The Pregnancy Outcomes in Patients With Previous Spontaneous AbortionsIJAR JOURNALNo ratings yet
- Austin Journal of Invitro FertilizationDocument5 pagesAustin Journal of Invitro FertilizationAustin Publishing GroupNo ratings yet
- Vaginal Delivery After Placental Abruption With IntrauterineDocument6 pagesVaginal Delivery After Placental Abruption With Intrauterinesamsara vrindaNo ratings yet
- Pi Is 0015028212014069Document1 pagePi Is 0015028212014069Vasantham HospitalNo ratings yet
- Sperma Analisis PaperDocument6 pagesSperma Analisis PaperFedrik Monte Kristo LimbongNo ratings yet
- GeneticaDocument5 pagesGeneticayessyNo ratings yet
- (Zafar Iqba) An Islamic Perspect On GovernanceDocument28 pages(Zafar Iqba) An Islamic Perspect On GovernancenazeerahmadNo ratings yet
- 6 PGS缩短受孕时间Document8 pages6 PGS缩短受孕时间zjuwindNo ratings yet
- Cerclage For Women With Twin Pregnancies: A Systematic Review and MetaanalysisDocument16 pagesCerclage For Women With Twin Pregnancies: A Systematic Review and MetaanalysisSaira MendozaNo ratings yet
- Bosdou-2019-Higher Probability of Live-Birth IDocument15 pagesBosdou-2019-Higher Probability of Live-Birth Inathalieleclef125No ratings yet
- Intrapartum Fetal Monitoring PDFDocument4 pagesIntrapartum Fetal Monitoring PDFelda zulkarnainNo ratings yet
- Short Stature As An Independent Risk Factor For Cephalopelvic Disproportion in A Country of Relatively Small-Sized MothersDocument4 pagesShort Stature As An Independent Risk Factor For Cephalopelvic Disproportion in A Country of Relatively Small-Sized MothersLeni AnggrainiNo ratings yet
- Journal ClubDocument9 pagesJournal ClubnoorNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- A B C A A A: Fertility & SterilityDocument2 pagesA B C A A A: Fertility & SterilityAisyahNo ratings yet
- Procedures and Techniques-Clinical: ArtDocument2 pagesProcedures and Techniques-Clinical: ArtGeos KarNo ratings yet
- Atosiban 2Document7 pagesAtosiban 2Meliana JayasaputraNo ratings yet
- 1 s2.0 S1472648318305911 MainDocument3 pages1 s2.0 S1472648318305911 MainManal Mozalbat HaddadNo ratings yet
- SARTscoring SETpaperDocument6 pagesSARTscoring SETpaperFedrik Monte Kristo LimbongNo ratings yet
- Ofir 2003Document5 pagesOfir 2003Jim HawkinsNo ratings yet
- Pi Is 0015028209011005Document6 pagesPi Is 0015028209011005Meli AnaNo ratings yet
- Reproductive Biology and EndocrinologyDocument5 pagesReproductive Biology and EndocrinologyАнатолий КомогорцевNo ratings yet
- Aneuploidy ConcordanceDocument12 pagesAneuploidy ConcordancejuanNo ratings yet
- Cervical EncerclageDocument25 pagesCervical EncerclageKartheek VarmaNo ratings yet
- Benchaib 2007Document8 pagesBenchaib 2007Tiffany LamNo ratings yet
- Fetomaternal BleedingDocument4 pagesFetomaternal BleedingHartanto LieNo ratings yet
- Pi Is 1028455916300389Document5 pagesPi Is 1028455916300389Ana AdamNo ratings yet
- Arabin Pessary To Prevent Adverse Perinatal Outcomes in Twin Pregnancies With A Short Cervix, PESSARONE. Marion GroussollesDocument13 pagesArabin Pessary To Prevent Adverse Perinatal Outcomes in Twin Pregnancies With A Short Cervix, PESSARONE. Marion GroussollesqmfddnhdjmNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Low Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665Document5 pagesLow Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665GayathriMaranNo ratings yet
- Alteration of Final Maturation and Laboratory Techniques in Low RespondersDocument7 pagesAlteration of Final Maturation and Laboratory Techniques in Low RespondersGayathriMaranNo ratings yet
- Controversies in ART: Can The IVF Laboratory Influence Preimplantation Embryo Aneuploidy?Document9 pagesControversies in ART: Can The IVF Laboratory Influence Preimplantation Embryo Aneuploidy?GayathriMaranNo ratings yet
- ISAR 2023 Brochure v1Document8 pagesISAR 2023 Brochure v1GayathriMaranNo ratings yet
- PIIS0015028220316599Document1 pagePIIS0015028220316599GayathriMaranNo ratings yet
- PIIS0015028222000164Document1 pagePIIS0015028222000164GayathriMaranNo ratings yet
- Testosterone and Growth Hormone in Older Men For Better or For WorseDocument4 pagesTestosterone and Growth Hormone in Older Men For Better or For WorseGayathriMaranNo ratings yet
- Luteinizing Hormone - Independent Rise of Progesterone As The Physiological Trigger of The Ovulatory Gonadotropins Surge in The HumanDocument9 pagesLuteinizing Hormone - Independent Rise of Progesterone As The Physiological Trigger of The Ovulatory Gonadotropins Surge in The Humansiti indah hardiyantiNo ratings yet
- PIIS1472648310619980Document7 pagesPIIS1472648310619980GayathriMaranNo ratings yet
- IMO Class 3Document15 pagesIMO Class 3Jagadeesh Kumar100% (3)
- English Literature: Prose 1Document13 pagesEnglish Literature: Prose 1GayathriMaranNo ratings yet
- Media Bulletin 19 05 20 COVID 19 6 PM PDFDocument25 pagesMedia Bulletin 19 05 20 COVID 19 6 PM PDFGayathriMaranNo ratings yet
- Abstracts Vol. 90, Suppl 1, September 2008Document2 pagesAbstracts Vol. 90, Suppl 1, September 2008GayathriMaranNo ratings yet
- Sample Paper Syllabus 2019-20: ClassDocument18 pagesSample Paper Syllabus 2019-20: ClassGayathriMaranNo ratings yet
- Father of InventionsDocument9 pagesFather of InventionsGayathriMaranNo ratings yet
- EVS Slip Test 3 II STDDocument2 pagesEVS Slip Test 3 II STDGayathriMaranNo ratings yet
- Media Bulletin 21 05 20 COVID 19 6 PM PDFDocument28 pagesMedia Bulletin 21 05 20 COVID 19 6 PM PDFGayathriMaranNo ratings yet
- What Can The Clinician Do To Improve Implantation?: OutlookDocument11 pagesWhat Can The Clinician Do To Improve Implantation?: OutlookGayathriMaranNo ratings yet
- Star BeginnersDocument3 pagesStar BeginnersGayathriMaranNo ratings yet
- Media Bulletin 19 05 20 COVID 19 6 PM PDFDocument25 pagesMedia Bulletin 19 05 20 COVID 19 6 PM PDFGayathriMaranNo ratings yet
- Cuddalore Classwork - 2 Grade 3 Evs 1 (Science) - Chapter 2 - Parts of Our BodyDocument2 pagesCuddalore Classwork - 2 Grade 3 Evs 1 (Science) - Chapter 2 - Parts of Our BodyGayathriMaranNo ratings yet
- From The Principal's Desk: CuddaloreDocument16 pagesFrom The Principal's Desk: CuddaloreGayathriMaranNo ratings yet
- Media Bulletin 20 05 20 COVID 19 6 PM PDFDocument25 pagesMedia Bulletin 20 05 20 COVID 19 6 PM PDFGayathriMaranNo ratings yet
- 29 82 PDFDocument6 pages29 82 PDFGayathriMaranNo ratings yet
- Piis0015028211013112 PDFDocument2 pagesPiis0015028211013112 PDFGayathriMaranNo ratings yet
- Pi Is 0015028214023498Document2 pagesPi Is 0015028214023498GayathriMaranNo ratings yet
- Pi Is 0015028216532257Document4 pagesPi Is 0015028216532257GayathriMaranNo ratings yet
- Pi Is 1472648310611716Document4 pagesPi Is 1472648310611716GayathriMaranNo ratings yet
- MPDF PDFDocument4 pagesMPDF PDFGayathriMaranNo ratings yet
- Pi Is 0015028211013112Document1 pagePi Is 0015028211013112GayathriMaranNo ratings yet
- Sindroma MetabolikDocument24 pagesSindroma MetabolikAnissa Aulia AdjaniNo ratings yet
- TMC Dosing ChartDocument6 pagesTMC Dosing ChartScott100% (1)
- Micro Blading Training BibleDocument98 pagesMicro Blading Training Biblezaina28No ratings yet
- Genetic Algorithm VS Memetic Algorithm For Automated Music CompositionDocument5 pagesGenetic Algorithm VS Memetic Algorithm For Automated Music CompositionMondheera PituxcoosuvarnNo ratings yet
- UrochordatevolutionDocument15 pagesUrochordatevolutionRodrigo CarralNo ratings yet
- The Windmill Technique Avoids Manual Removal of The RetainedDocument6 pagesThe Windmill Technique Avoids Manual Removal of The RetainedEndrianus Jaya PutraNo ratings yet
- Name:-Zain Abbas Rollno: - 9837 Program: - DPT (6Th) Submitted To Ma'M Iqra NawazDocument19 pagesName:-Zain Abbas Rollno: - 9837 Program: - DPT (6Th) Submitted To Ma'M Iqra NawazAbdul MuqeetNo ratings yet
- 01 Lecture Animation PPTDocument47 pages01 Lecture Animation PPTMary JewelNo ratings yet
- Problems With The Management of The Golden Apple Snail Pomacea Canaliculata: An Important Exotic Pest of Rice in AsiaDocument2 pagesProblems With The Management of The Golden Apple Snail Pomacea Canaliculata: An Important Exotic Pest of Rice in AsiaGerryanna MagbitangNo ratings yet
- Whole Face Approach With Hyaluronic Acid FillersDocument11 pagesWhole Face Approach With Hyaluronic Acid Fillersalh basharNo ratings yet
- Fee - 19th Century Craniology - The Study of The Female SkullDocument19 pagesFee - 19th Century Craniology - The Study of The Female SkullMaivyTranNo ratings yet
- Clone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Document3 pagesClone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Jaimier CajandabNo ratings yet
- Non Spatial FieldsDocument19 pagesNon Spatial FieldsMariano SerranoNo ratings yet
- Sage Genetics Lecture 2017 ExpoDocument55 pagesSage Genetics Lecture 2017 ExpoJosé Nigadera de la SotaNo ratings yet
- Filipino ScientistDocument13 pagesFilipino ScientistFiona Ramirez RomeroNo ratings yet
- Adv Sci G7Document22 pagesAdv Sci G7Ezequiel ManluluNo ratings yet
- PUB - NEWater - Quality 1Document1 pagePUB - NEWater - Quality 1Weijin LeowNo ratings yet
- Cactus Explorer 09 - Complete PDFDocument56 pagesCactus Explorer 09 - Complete PDFkhun sakNo ratings yet
- DNA ReplicationDocument3 pagesDNA ReplicationApril Marie100% (3)
- Cleavage, Blastula, Gastrula, NeurulaDocument41 pagesCleavage, Blastula, Gastrula, NeurulaHyenaNo ratings yet
- Nurul Berliana Aini - 081911433043 - D1 - Laporan Praktikum Sampling BentosDocument17 pagesNurul Berliana Aini - 081911433043 - D1 - Laporan Praktikum Sampling Bentosprisca wibawaNo ratings yet
- JEI Manuscript Template v.2.2023Document8 pagesJEI Manuscript Template v.2.2023Alp Arda ÇimenNo ratings yet
- Anatomy and Physiology ResourcesDocument4 pagesAnatomy and Physiology Resourcesmasmakkin6170No ratings yet
- Endokrinologi - Kanker ProstatDocument11 pagesEndokrinologi - Kanker ProstatPutri Mustika SariNo ratings yet
- S5LT-IIc-3.3.1-THE MENSTRUAL CYCLE PDFDocument5 pagesS5LT-IIc-3.3.1-THE MENSTRUAL CYCLE PDFMelyn BustamanteNo ratings yet
- 1 s2.0 S1367048418310452 MainDocument6 pages1 s2.0 S1367048418310452 MainskocabzzNo ratings yet
- Biology 9th Specs 1 PDFDocument1 pageBiology 9th Specs 1 PDFAamir HabibNo ratings yet
- Chapter 1 Nutrition and MetabolismDocument19 pagesChapter 1 Nutrition and Metabolismbayan.grNo ratings yet
- 56 4 Article01Document14 pages56 4 Article01Thiago GomezNo ratings yet
- Bamboo Research in The Philippines - Cristina A. RoxasDocument14 pagesBamboo Research in The Philippines - Cristina A. RoxashazelNo ratings yet