You might also like
- Mini Warfarin GuidelinesDocument2 pagesMini Warfarin GuidelinesPeunn NattaphatNo ratings yet
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- IV Push MedicationsDocument67 pagesIV Push Medicationsbtalera100% (1)
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Heparin Drip ProtocolDocument16 pagesHeparin Drip Protocolapi-277534147100% (1)
- 1st Line Medication of An e CartDocument5 pages1st Line Medication of An e CartColette Marie PerezNo ratings yet
- Anatomy Mnemonics 2Document50 pagesAnatomy Mnemonics 2Nourhan JamalNo ratings yet
- Science 10 Module 1 3qDocument5 pagesScience 10 Module 1 3qDionil CabilanNo ratings yet
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Chick 72 HR DDocument35 pagesChick 72 HR Daa628No ratings yet
- List of Geometric CardsDocument102 pagesList of Geometric CardsamazingdivinegraceNo ratings yet
- Medication Administration PolicyDocument188 pagesMedication Administration Policyليراث ليNo ratings yet
- Pre-Board Exam For July 2011 NLEDocument37 pagesPre-Board Exam For July 2011 NLEdammenoel100% (2)
- 19 30s ExerciseDocument10 pages19 30s Exercisegirard_boweNo ratings yet
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioNo ratings yet
- Pharmacology Viva Manual Prefinal PDFDocument112 pagesPharmacology Viva Manual Prefinal PDF9821699080100% (1)
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookAnonymous FSUnLYr4yNo ratings yet
- Zhan ZhuangDocument13 pagesZhan ZhuangBrian ColborneNo ratings yet
- RFDS Western Operations HEA16 - V3.0 Clinical ManualDocument28 pagesRFDS Western Operations HEA16 - V3.0 Clinical ManualJoed BiasonNo ratings yet
- Pediatric Dosage CalculationsDocument5 pagesPediatric Dosage CalculationsLovely Anjenell MacalingaNo ratings yet
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- HeparinDocument4 pagesHeparinapi-3797941100% (2)
- Living Longer and Healthier LifeDocument233 pagesLiving Longer and Healthier Lifeweisberger100% (1)
- Aplikasi - 3S - Sdki - Slki.siki (Pak Adam) 02Document16 pagesAplikasi - 3S - Sdki - Slki.siki (Pak Adam) 02Anis Nur AfifahNo ratings yet
- Oet Reading - DVTDocument11 pagesOet Reading - DVTOlive GroupNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Amended Intravenous Unfractionated Heparin Recommended StandardDocument4 pagesAmended Intravenous Unfractionated Heparin Recommended StandardTOJO JOSEPH TOMNo ratings yet
- UFH LMWH Fonda - 06september2020Document7 pagesUFH LMWH Fonda - 06september2020gabrimarteNo ratings yet
- Drug Guideline Title: Remifentanil: SummaryDocument11 pagesDrug Guideline Title: Remifentanil: SummaryyafetNo ratings yet
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xNo ratings yet
- Anticoagulations in Surgery: Sharifah Naiemah BT Syed MansorDocument20 pagesAnticoagulations in Surgery: Sharifah Naiemah BT Syed MansorSharifah NaiemahNo ratings yet
- ICU 2 - Management For DICDocument20 pagesICU 2 - Management For DICNur Aziemah Mohd ZamriNo ratings yet
- Enoxaparin MAGDocument2 pagesEnoxaparin MAGmlbrown8No ratings yet
- Nclex 3 With RationaleDocument13 pagesNclex 3 With RationaleMsPocketbook HoarderNo ratings yet
- Surviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016Document36 pagesSurviving Sepsis Campaign: International Guidelines For Management of Severe Sepsis and Septic Shock: 2016IvanRaykaNo ratings yet
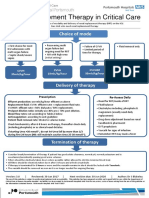
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Con 1420782810247Document7 pagesCon 1420782810247AsetonitrileNo ratings yet
- Anticoag GuidelinesDocument22 pagesAnticoag Guidelinesyusuf100% (1)
- RocuroniumbromideinjDocument14 pagesRocuroniumbromideinjagnes hutabaratNo ratings yet
- Low Molecular Weight Heparins (LMWH) : I. Mechanism of ActionDocument7 pagesLow Molecular Weight Heparins (LMWH) : I. Mechanism of ActionIniya RajendranNo ratings yet
- Unfractionate Heparin Low Molecular Weight HeparinDocument3 pagesUnfractionate Heparin Low Molecular Weight HeparinArun KumarNo ratings yet
- Deep Vein ThrombosisDocument22 pagesDeep Vein ThrombosisEznal MahidinNo ratings yet
- Pediatric Hematology Oncology Ward Officer HandbookDocument40 pagesPediatric Hematology Oncology Ward Officer HandbookLetchumana KrishnanNo ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- S 011 LBLDocument22 pagesS 011 LBLalexandr zinchenkoNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Enoxaparin Sodium Injection I.PDocument15 pagesEnoxaparin Sodium Injection I.PSuhailansariNo ratings yet
- Drug - Guide - Scavenger - Hunt - Docx 16th EditionDocument5 pagesDrug - Guide - Scavenger - Hunt - Docx 16th EditionYousaf FarookNo ratings yet
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocument5 pagesHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNo ratings yet
- Clinical Diagnosis ofDocument14 pagesClinical Diagnosis ofNor Shuhada HaronNo ratings yet
- LMWH QML 06Document7 pagesLMWH QML 06pd7qmlNo ratings yet
- Anx 135796 enDocument108 pagesAnx 135796 enMohamed RawyNo ratings yet
- Orig 1 S 187 LBLDocument20 pagesOrig 1 S 187 LBLfarezpharmaNo ratings yet
- EPIRUBICIN Ferron PharmaceuticalsDocument7 pagesEPIRUBICIN Ferron PharmaceuticalsHep PutNo ratings yet
- Print 18Document4 pagesPrint 18Mahmoud SelimNo ratings yet
- Nuwiq Epar Product Information enDocument54 pagesNuwiq Epar Product Information enSutirtha MukhopadhyayNo ratings yet
- ClexaneinjDocument25 pagesClexaneinjBobeico TatianaNo ratings yet
- SURGERY PROTOCOL Pacientes Con AddisonDocument3 pagesSURGERY PROTOCOL Pacientes Con AddisonLuis GarciaNo ratings yet
- VF PediDocument6 pagesVF PedixiphoideusNo ratings yet
- OB Hem Uterotonic Medications For Prevention and Treatment of PPHDocument7 pagesOB Hem Uterotonic Medications For Prevention and Treatment of PPHpwytymbm56No ratings yet
- Annex I Summary of Product CharacteristicsDocument42 pagesAnnex I Summary of Product CharacteristicsDonald RangerNo ratings yet
- Acute Management Hipercianotic SpellsDocument2 pagesAcute Management Hipercianotic SpellsSigit SutantoNo ratings yet
- TPE Protocol 2018Document5 pagesTPE Protocol 2018AnaNo ratings yet
- Envarsus Epar Product Information enDocument51 pagesEnvarsus Epar Product Information enEnam HaqNo ratings yet
- Drug On ElaximDocument6 pagesDrug On ElaximBabesNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?From EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?No ratings yet
- Spoken Production.Document4 pagesSpoken Production.brettymel.nuiqueNo ratings yet
- Prices For UgandaDocument9 pagesPrices For UgandaSyed Arshad HussainNo ratings yet
- Previouspaper BSSC Graduate Level Main Exam 2010 GKDocument48 pagesPreviouspaper BSSC Graduate Level Main Exam 2010 GKJay Prakash PatelNo ratings yet
- Paper de JB FRBDocument1 pagePaper de JB FRBjbenitesvilchezNo ratings yet
- BC Biomedical DA-2006 Defibrillator Analyzer - Service ManualDocument171 pagesBC Biomedical DA-2006 Defibrillator Analyzer - Service ManualSerginho Henrique100% (2)
- Anatomy Helpers Blood Supply To Abdominal OrgansDocument5 pagesAnatomy Helpers Blood Supply To Abdominal OrgansSam TagardaNo ratings yet
- Oral Report - Experiment 4Document52 pagesOral Report - Experiment 4Kristella DraheimNo ratings yet
- Plant Cell WallDocument2 pagesPlant Cell WallShiela BelandresNo ratings yet
- Sub 1.5 Body Defence MechanismDocument17 pagesSub 1.5 Body Defence Mechanismliefeng81No ratings yet
- Jared MendezDocument5 pagesJared MendezJared StudyNo ratings yet
- March 2016 (v2) QP - Paper 4 CIE Biology A-LevelDocument28 pagesMarch 2016 (v2) QP - Paper 4 CIE Biology A-LevelDivine-joyNo ratings yet
- Ecology of The Microbiome of The Infected Root Canal System A Comparison Between Apical and Coronal Root SegmentsDocument15 pagesEcology of The Microbiome of The Infected Root Canal System A Comparison Between Apical and Coronal Root Segmentsabcder1234No ratings yet
- Reuss, Kiesel, Kundev & Hommel 2011 Unconscious Activation of Task SetsDocument12 pagesReuss, Kiesel, Kundev & Hommel 2011 Unconscious Activation of Task SetshoorieNo ratings yet
- Nutrition in OrthodonticsDocument51 pagesNutrition in OrthodonticsShweta DU80% (5)
- Bloque 2.1. Sleisenger and Fordtran'S - Section X - Chapter 122Document23 pagesBloque 2.1. Sleisenger and Fordtran'S - Section X - Chapter 122Danisi ObregonNo ratings yet
- Opioids AutacoidsDocument22 pagesOpioids AutacoidsSiddharth Anand80% (5)
- Genetics Solution Manual - Chapter 3Document22 pagesGenetics Solution Manual - Chapter 3amarka01No ratings yet
- Vasopressors and Inotropes 120465803991568 4Document31 pagesVasopressors and Inotropes 120465803991568 4Guillermo Gp Equus Ferus CaballusNo ratings yet
- Allreports AspxDocument4 pagesAllreports AspxRoyal XeroxNo ratings yet