You might also like
- Draw A PersonDocument33 pagesDraw A PersonCarm RiveraNo ratings yet
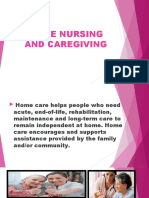
- Home Nursing and CaregivingDocument78 pagesHome Nursing and CaregivingJake Arizapa100% (1)
- Mosbys Textbook For Nursing Assistants 8th Edition Sorrentino Test BankDocument5 pagesMosbys Textbook For Nursing Assistants 8th Edition Sorrentino Test BankCherokee0% (1)
- RMA Skill Practice: Registered Medical Assistant Practice Test QuestionsFrom EverandRMA Skill Practice: Registered Medical Assistant Practice Test QuestionsNo ratings yet
- End of Life CareDocument80 pagesEnd of Life CareRakesh MohanNo ratings yet
- End of Life CareDocument25 pagesEnd of Life CareMeenu DograNo ratings yet
- Amber Sparks, "How To Share Your Home With A Ghost" (Short Story, 2020)Document25 pagesAmber Sparks, "How To Share Your Home With A Ghost" (Short Story, 2020)39 RYAN Ryan Justin UyNo ratings yet
- Nursing Care at The End of Life PDFDocument139 pagesNursing Care at The End of Life PDFPradeep JNANo ratings yet
- Chapter - 010 Home Health CareDocument6 pagesChapter - 010 Home Health CareTrixie AlvarezNo ratings yet
- End of Life CareDocument15 pagesEnd of Life CareAnonymous gEGf1C100% (2)
- Analisis Jurnal End of Life-Tedi&saidDocument5 pagesAnalisis Jurnal End of Life-Tedi&saidYulia JuniartiNo ratings yet
- Clinical Pathway Acute Psych BehavioralDocument3 pagesClinical Pathway Acute Psych Behavioraladadan100% (2)
- Miller, Nursing For Wellness in Older Adult.1Document13 pagesMiller, Nursing For Wellness in Older Adult.1MindiRahayuNo ratings yet
- HIRAC Electrical Work PDFDocument9 pagesHIRAC Electrical Work PDFBasil George100% (5)
- To Whom It May ConcernDocument23 pagesTo Whom It May ConcernAnonymous Km3FXs5vNo ratings yet
- Instructors Guide Canadian Integrating A Palliative Approach - Essentials For Personal Support Workers1Document46 pagesInstructors Guide Canadian Integrating A Palliative Approach - Essentials For Personal Support Workers1KATHY TRUONG67% (6)
- CH 11 Admission, Discharge, Transfers & ReferralsDocument14 pagesCH 11 Admission, Discharge, Transfers & ReferralsNilakshi Barik Mandal100% (1)
- Principles of Palliative Care 2nd PartDocument26 pagesPrinciples of Palliative Care 2nd PartDisala Ranaweera100% (1)
- End of Life Care FDocument84 pagesEnd of Life Care FJhunnie NuquiNo ratings yet
- MPH Entrance Examination With AnswersDocument42 pagesMPH Entrance Examination With Answersahmedhaji_sadik94% (87)
- Nursing Test QuestionsDocument14 pagesNursing Test Questionsconsultant11100% (1)
- E NursingDocument16 pagesE Nursinggopscharan100% (1)
- Home and Palliative Care FinalDocument41 pagesHome and Palliative Care Finalpeca65No ratings yet
- Sample PSW Resume - 3Document2 pagesSample PSW Resume - 3branislava1301No ratings yet
- END OF LIFE CareDocument25 pagesEND OF LIFE Caregireeshsachin100% (1)
- Restraint Use and Patient Care: Nnual CompetencyDocument35 pagesRestraint Use and Patient Care: Nnual CompetencyrustiejadeNo ratings yet
- Palliative Care NursingYESSDocument402 pagesPalliative Care NursingYESSWilliam Will100% (3)
- Futuristic NursingDocument32 pagesFuturistic NursingRabiu Hassan Musa100% (1)
- Psychiatric Nursing Notes: History, AsylumsDocument62 pagesPsychiatric Nursing Notes: History, Asylumssurviving nursing school100% (1)
- Patient Care Technician Textbook PDF ISBN 978-1495107993Document24 pagesPatient Care Technician Textbook PDF ISBN 978-1495107993McGill0% (8)
- Professionalism in NursingDocument28 pagesProfessionalism in NursingIkenna Okpala100% (3)
- Local State of Children Report 2020Document4 pagesLocal State of Children Report 2020QUeen Dai SY Ramirez100% (10)
- Concepts of Palliative CareDocument53 pagesConcepts of Palliative CareBlessed Abigael100% (2)
- Community Mental HealthDocument11 pagesCommunity Mental HealthManoj GargNo ratings yet
- Nursing Case ManagementDocument11 pagesNursing Case ManagementLohith Sunshine100% (1)
- Hospice & Palliative CareDocument21 pagesHospice & Palliative CareAmy100% (1)
- Palliative Care - End of Life Care - Northern HealthDocument8 pagesPalliative Care - End of Life Care - Northern HealthDiklatpimempat AngkatanlimabelasNo ratings yet
- End-Of-Life Decision Making Across CulturesDocument15 pagesEnd-Of-Life Decision Making Across CulturesPamNo ratings yet
- Nursing and End-of-Life CareDocument26 pagesNursing and End-of-Life CareShafiq Ur RahmanNo ratings yet
- End of Life CareDocument11 pagesEnd of Life CareBelindaNo ratings yet
- Palliative Care NursingDocument64 pagesPalliative Care NursingPrince Jhessie L. Abella100% (1)
- Quality of Life S U Comments: Procedure ChecklistsDocument3 pagesQuality of Life S U Comments: Procedure ChecklistsMariam100% (1)
- Palliative CareDocument23 pagesPalliative CareCharles Frank100% (1)
- Oncology NursingDocument158 pagesOncology NursingHebsiba PonnayyanNo ratings yet
- WCU APRN Student HandbookDocument17 pagesWCU APRN Student HandbookEllie MehrNo ratings yet
- Health and Wellness Industry OverviewDocument20 pagesHealth and Wellness Industry OverviewdeepcancerNo ratings yet
- MPH Entrance Exam For 2007Document3 pagesMPH Entrance Exam For 2007ahmedhaji_sadik100% (7)
- (DR Joyce Zerwekh) Nursing Care at The End of LifeDocument472 pages(DR Joyce Zerwekh) Nursing Care at The End of LifeSubbie Outlier83% (6)
- CHRC SWMS Mobilisation and DeMobilisationDocument8 pagesCHRC SWMS Mobilisation and DeMobilisationStansilous Tatenda NyagomoNo ratings yet
- Standards, Challenges & Scope of Psychiatric Nursing Multi-Disciplinary Team & Role of NurseDocument66 pagesStandards, Challenges & Scope of Psychiatric Nursing Multi-Disciplinary Team & Role of NurseJoric MagusaraNo ratings yet
- People V PaycanaDocument1 pagePeople V PaycanaPrincess Trisha Joy UyNo ratings yet
- The Nursing Health HistoryDocument25 pagesThe Nursing Health HistoryJonah R. MeranoNo ratings yet
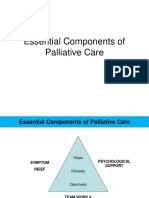
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano60% (5)
- Emotional IntellegenceDocument7 pagesEmotional IntellegenceGirish SubramanianNo ratings yet
- Hospice Care in The Nursing HomeDocument73 pagesHospice Care in The Nursing Homeraul nino Moran100% (1)
- Masticatory EfficiencyDocument19 pagesMasticatory EfficiencyVikas AggarwalNo ratings yet
- Hospice Care PlanDocument9 pagesHospice Care PlanAmanda SimpsonNo ratings yet
- Hospice and PallativeDocument38 pagesHospice and PallativeVhe Pacatang100% (1)
- The Nurses Role in Palliative Care A QualitativeDocument18 pagesThe Nurses Role in Palliative Care A Qualitativesukarni84sgdNo ratings yet
- Care of Dying and DeadDocument10 pagesCare of Dying and Deadd1choosenNo ratings yet
- Singson vs. SingsonDocument2 pagesSingson vs. SingsonBay NazarenoNo ratings yet
- The Palliative Approach: A Resource for Healthcare WorkersFrom EverandThe Palliative Approach: A Resource for Healthcare WorkersRating: 4.5 out of 5 stars4.5/5 (3)
- MCQ Sick NewbornDocument21 pagesMCQ Sick NewbornprabhatNo ratings yet
- Week 4 # 3 Delirium-1Document25 pagesWeek 4 # 3 Delirium-1charissa100% (1)
- Preceptor Handbook For Nursing EducationDocument41 pagesPreceptor Handbook For Nursing EducationBryan Mae H. Degorio0% (1)
- Murray Nadels Textbook of Respiratory Medicine 7Th Edition Various Authors Download 2024 Full ChapterDocument47 pagesMurray Nadels Textbook of Respiratory Medicine 7Th Edition Various Authors Download 2024 Full Chaptergary.wesley812100% (11)
- Palliative Care in Bangladesh: Group: IDocument38 pagesPalliative Care in Bangladesh: Group: IShipra TalukderNo ratings yet
- Community Case: Faith-Based CommunityDocument1 pageCommunity Case: Faith-Based CommunityFatima G ReyesNo ratings yet
- Nursing Prioritization of The Patient Ne PDFDocument13 pagesNursing Prioritization of The Patient Ne PDFBambim TexonNo ratings yet
- Palliative NursingDocument31 pagesPalliative NursingNyein MohNo ratings yet
- Govt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeDocument17 pagesGovt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeMamta YadavNo ratings yet
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Document6 pagesRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERINo ratings yet
- Admission, Discharge, Transfer & ReferralsDocument31 pagesAdmission, Discharge, Transfer & ReferralsYousef JafarNo ratings yet
- Haji 100Document40 pagesHaji 100ahmedhaji_sadikNo ratings yet
- MPH TestDocument47 pagesMPH Testahmedhaji_sadik50% (2)
- Enterance ExamDocument2 pagesEnterance Examahmedhaji_sadikNo ratings yet
- Enterance ExamDocument2 pagesEnterance Examahmedhaji_sadikNo ratings yet
- Final Exam1Document2 pagesFinal Exam1ahmedhaji_sadikNo ratings yet
- 008 Vaccancy Health and Nutrition Project OfficerDocument3 pages008 Vaccancy Health and Nutrition Project Officerahmedhaji_sadikNo ratings yet
- ANC Ahmedhaji DocumentsDocument34 pagesANC Ahmedhaji Documentsahmedhaji_sadik100% (1)
- Manji Yamada V/s Union of India (UOI) and Anr.Document6 pagesManji Yamada V/s Union of India (UOI) and Anr.DimpleChainaniNo ratings yet
- Level 2 Award in Health and Safety in The Workplace: Instructions To CandidatesDocument4 pagesLevel 2 Award in Health and Safety in The Workplace: Instructions To CandidatesCLIFFORD DAKYAHASNo ratings yet
- Tofen TabDocument2 pagesTofen TabTasif AmirNo ratings yet
- Surat Trip Ke Bank Negara MalaysiaDocument2 pagesSurat Trip Ke Bank Negara MalaysiaZaid IbrahimNo ratings yet
- Katzung, B Farmakologi Dasar Dan Klinik Edisi 10. Jakarta - EGC, 2010.Document5 pagesKatzung, B Farmakologi Dasar Dan Klinik Edisi 10. Jakarta - EGC, 2010.M. Yusuf DaliNo ratings yet
- MATERIAL SAFETY Ava - Bridgepak - C-MDocument4 pagesMATERIAL SAFETY Ava - Bridgepak - C-Mfs1640No ratings yet
- Ortho CurriculumDocument53 pagesOrtho CurriculumlanghalilafaNo ratings yet
- Claire Musgrove ResumeDocument1 pageClaire Musgrove Resumeapi-453824286No ratings yet
- Laporan Praktikum HematologiDocument12 pagesLaporan Praktikum HematologiAnang Yanuar RamadhanNo ratings yet
- FORTRON® 1120L4 - PPS - Specialty: DescriptionDocument2 pagesFORTRON® 1120L4 - PPS - Specialty: DescriptionAdam GordonNo ratings yet
- Day 24 Population Aging Ielts NguyenhuyenDocument1 pageDay 24 Population Aging Ielts NguyenhuyenAn QuanNo ratings yet
- Early-Onset Neonatal Sepsis 2014Document27 pagesEarly-Onset Neonatal Sepsis 2014Ninde Rivera GonzalezNo ratings yet
- 5 6088992044825444514Document16 pages5 6088992044825444514Prakash Aradhya RNo ratings yet
- Ebook Respiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition PDF Full Chapter PDFDocument68 pagesEbook Respiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition PDF Full Chapter PDFkyle.heffner607100% (32)
- Prerequisite Skills For Language: E C S C D SDocument3 pagesPrerequisite Skills For Language: E C S C D SBernard CarpioNo ratings yet
- Dangerous Drugs Board: Methamphetamine Hydrochloride (Shabu)Document5 pagesDangerous Drugs Board: Methamphetamine Hydrochloride (Shabu)Kelly AlairNo ratings yet
- Laparoscopic CholecystectomyDocument10 pagesLaparoscopic CholecystectomyCharm TanyaNo ratings yet