Professional Documents
Culture Documents
MRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple Sclerosis
Uploaded by
IreneOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
MRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple Sclerosis
Uploaded by
IreneCopyright:
Available Formats
Personal View
MRI monitoring of pathological changes in the spinal cord in
patients with multiple sclerosis
Achim Gass, Maria A Rocca, Federica Agosta, Olga Ciccarelli, Declan Chard, Paola Valsasina, Jonathan C W Brooks, Antje Bischof, Philipp Eisele,
Ludwig Kappos, Frederik Barkhof, Massimo Filippi, for the MAGNIMS Study Group*
The spinal cord is a clinically important site that is affected by pathological changes in most patients with multiple Lancet Neurol 2015; 14: 443–54
sclerosis; however, imaging of the spinal cord with conventional MRI can be difficult. Improvements in MRI provide Published Online
a major advantage for spinal cord imaging, with better signal-to-noise ratio and improved spatial resolution. Through March 4, 2015
http://dx.doi.org/10.1016/
the use of multiplanar MRI, identification of diffuse and focal changes in the whole spinal cord is now routinely
S1474-4422(14)70294-7
possible. Corroborated by related histopathological analyses, several new techniques, such as magnetisation transfer,
See Comment page 348
diffusion tension imaging, functional MRI, and proton magnetic resonance spectroscopy, can detect non-focal, spinal
*Steering Committee members
cord pathological changes in patients with multiple sclerosis. Additionally, functional MRI can reveal changes in the listed at end of paper
response pattern to sensory stimulation in patients with multiple sclerosis. Through use of these techniques, findings Department of Neurology,
of cord atrophy, intrinsic cord damage, and adaptation are shown to occur largely independently of focal spinal cord Universitätsmedizin
lesion load, which emphasises their relevance in depiction of the true burden of disease. Combinations of Mannheim UMM, University of
magnetisation transfer ratio or diffusion tension imaging indices with cord atrophy markers seem to be the most Heidelberg, Germany
(A Gass MD, P Eisele);
robust and meaningful biomarkers to monitor disease evolution in early multiple sclerosis. Neuroimaging Research Unit,
Institute of Experimental
Introduction features of multiple sclerosis in the spinal cord, assess Neurology, Division of
Inflammatory demyelination and neurodegeneration are improvements in conventional MRI techniques, and Neuroscience and Department
of Neurology, San Raffaele
present from the very early stages of multiple sclerosis. discuss the newer MRI approaches that have provided Scientific Institute, Vita-Salute
Brain MRI has helped greatly to understand the insight into pathophysiology of the disease. We also San Raffaele University, Milan,
contribution from these processes to the pathology of address the relevance of developments in imaging and Italy (M A Rocca MD, F Agosta
multiple sclerosis, and both conventional MRI and their potential implications to help understand and MD, P Valsasina PhD, M Filippi
MD); NMR Research Unit,
quantitative approaches to assess neurodegeneration monitor spinal cord involvement in multiple sclerosis. Queen Square Multiple
have become accepted measures in clinical trials. The Sclerosis Centre (D Chard PhD)
spinal cord is also a clinically important site that is Pathological changes in the spinal cord and Department of Brain
Repair and Rehabilitation
affected by pathological changes in most patients with Focal spinal cord lesions are commonly seen in patients
(O Ciccarelli PhD); University
multiple sclerosis. MRI of the spinal cord is a recom- with multiple sclerosis, and tissue abnormalities are College London, Institute of
mended and valuable part of diagnostic investigations in reported in 80–90% of patients on conventional MRI.6–13 Neurology National Institute
patients with suspected multiple sclerosis.1–3 However, Spinal cord lesions usually do not respect the anatomical for Health Research, University
College London Hospitals,
MRI of the spinal cord is more challenging than brain grey–white matter boundaries.14–16 Most lesions are
Biomedical Research Centre,
MRI because the spinal cord is a long and thin structure located in the lateral or dorsal white matter and are only London, UK; University of
that has some mobility; MRI of the spinal cord is further infrequently seen in the anterior columns and central Bristol, Clinical Research and
complicated by artifacts (ie, from breathing, heartbeat, cord area. Most focal lesions are located in the cervical Imaging Centre, Bristol, UK
(J C W Brooks PhD); Department
CSF flow, and aortic flow).4,5 These inherent features cord. However, only 33 (16%) of 202 patients showed
of Neurology, University
make it difficult to image subtle pathological changes and exclusive cervical-cord lesions in a large cohort.9 In Hospital Basel, Basel,
to ensure comparability in follow-up examinations. patients with primary progressive multiple sclerosis, Switzerland (A Bischof MD,
Technical developments in MRI have increased the diffuse areas of mildly increased T2-weighted signal L Kappos MD); Department of
Radiology and Nuclear
signal-to-noise ratio for spinal cord MRI. The use of intensity are the predominant finding in the spinal cord,
Medicine, VU University
parallel imaging techniques, including improved coil whereas patients with secondary progressive multiple Medical Center, Amsterdam,
technology and high field strength, have improved sclerosis show mostly focal lesions at high signal Netherlands (F Barkhof MD)
conventional and quantitative MRI to become more intensity.17 Unlike white matter demyelination in all Correspondence to:
robust and improve the signal-to-noise ratio, image multiple sclerosis patients, which is widespread in the Dr Achim Gass, Department of
Neurology, Universitätsmedizin
resolution, and consequently, the sensitivity and the upper cervical part of the spinal cord, grey matter
Mannheim, University of
specificity of spinal cord MRI. New MRI techniques, demyelination has been shown to extend equally over all Heidelberg, 68135 Mannheim,
such as magnetisation transfer, diffusion tensor imaging spinal levels.18 Axonal loss occurs widely, with reduced Germany
(DTI), functional MRI (fMRI), and ¹H-magnetic axonal density of about 46%, even in normal-appearing achim.gass@medma.uni-
heidelberg.de
resonance spectroscopy (MRS), show an improved white matter. This increases up to about 59% in
picture on the presence and development of lesions, and hyperintense lesions on proton-density weighted
enable imaging of previously difficult to visualise images.19 Lateral columns are most affected, and anterior
pathological changes, enabling the assessment of their columns are least affected by axonal loss.20 In a post-
significance in relation to clinical disability. mortem study14 on 37 patients with multiple sclerosis,
We review the use of spinal cord MRI in multiple most of whom had a progressive disease course, total
sclerosis. We briefly present the main pathological neuronal number at the upper thoracic level was reduced
www.thelancet.com/neurology Vol 14 April 2015 443
Personal View
by 30·3% correlating with the multiple sclerosis disease Some limitations are known to affect the extrapolation
state. In histopathological tests, interneuron and motor of these post-mortem findings to in-vivo MRI of the
neuron numbers were reduced to various degrees, spinal cord. First of all, post-mortem imaging of spinal
notably at the upper spinal cord levels. These changes cord lacks motion and tissue artifacts, and surface coils
seem to occur mainly in demyelinated grey matter and provide a better signal-to-noise ratio. Furthermore, MRI
less so in myelinated grey matter.21 parameters, especially T1-relaxation time and magneti-
By contrast with demyelination, axonal pathological sation transfer ratio, are affected by formalin fixation.
changes do not correlate with findings on T2-weighted Spatial resolution and histopathological specificity is low
images, but seem to occur independently of de- in in-vivo MRI. Therefore, extrapolation of ex-vivo data to
myelination.20 This was corroborated by histopathological in vivo should be done with caution.
findings that axonal loss and diameter did not correlate
with myelin density.19 High signal intensity regions on T2- Conventional spinal cord MRI
weighted images showed nearly normal axonal features Imaging of demyelination
(staining intensity, diameter, regularity) on histopatho- Conventional spinal cord MRI is usually undertaken in
logical examination, suggesting that inflammation does the sagittal plane to cover a large anatomical area. Proton-
not necessarily lead to or precede axonal loss.20 density weighted, T2-weighted, or short tau inversion
Spinal cord atrophy might be due to focal tissue recovery (STIR) sequences are usually used, alone or in
destruction in lesions or to the degeneration of tracts combination, to visualise the outline of the cord, focal
secondary to pathological changes that damage axons. lesions, and diffuse hyperintense signal change. STIR
Two studies22,23 reported more pronounced atrophy in the sequences take longer than proton-density weighted MRI
cervical cord compared with the thoracic and lumbar cord but have a higher sensitivity to detect lesions.26 Frequently,
segments. Cord atrophy was mostly due to white matter two sets of sagittal images with different contrasts (proton-
volume loss, and these cord lesions have little effect on density weighted and T2-weighted, or T2-weighted and
local cord areas. Another study24 showed a clear gradient STIR) are used to increase confidence in lesion detection,
in axonal loss in the cord, with the greatest loss in the particularly because of spinal cord MRI motion artifacts.
cervical region and the least in the lumbar region. The inherent contrast of spinal cord lesions against
However, atrophy seemed to result from white matter healthy cord signal is usually lower than in the brain
loss because the white matter was substantially reduced parenchyma, which is one reason why fluid-attenuated
in in the upper spinal cord levels of patients with multiple inversion recovery (FLAIR) sequences are rarely used for
sclerosis, whereas the grey matter area was not sub- multiple sclerosis lesion detection in the spinal cord.27,28
stantially different between patients with multiple One advantage of the relative insensitivity of T1-weighted
sclerosis and healthy controls.22 By contrast, grey and MRI for the detection of lesions29 is its robustness for
white matter have also been reported to be affected to the spinal cord atrophy assessments. Whole-cord biplanar
same extent.25 Spinal cord atrophy was shown to associate MRI (in the sagittal and axial planes) is time-consuming,
with T1 and, to a lesser extent, with the increase in T2- but parallel imaging techniques with multiarray coils
relaxation time and with a decrease in magnetisation enable a scan of the whole cord to take place quickly.
transfer ratio. Furthermore, atrophy has been shown to Imaging in the axial plane can be very useful to ascertain
correlate well with disability, but is not a direct marker of suspected abnormal changes and can increase the
axonal numbers.19 confidence for the lesion detection in peripheral cord
Studies that correlate MRI findings with histo- locations, where partial-volume effects (limited resolution)
pathological findings suggest that conventional MRI is make lesion detection difficult on sagittal images
mainly sensitive to detect demyelination. From ex-vivo (figure 1).9 Diffuse hyperintense signal change, a patho-
MRI on the spinal cord, Gilmore and colleagues14 reported logical feature that is particularly frequent in patients with
a sensitivity of 87% for the detection of white matter primary progressive multiple sclerosis, is usually seen in
lesions at 4·7 T on proton-density weighted MRI the whole-cord cross-section. Differences in the reported
sequences, 73% for grey matter lesions, and a high frequency of these diffuse changes might be due to the
specificity for grey matter demyelination. In a comparison lower contrast-to-noise ratio of diffuse versus focal lesions
of different sequences, T2-weighted imaging was the and patient selection in different studies.9,13 Acute lesions
strongest to predict demyelination, but also other are often associated with cord swelling and with acute
sequences (proton density, magnetisation transfer ratio, symptoms, whereas overall30 contrast-enhancing lesions
relaxation-time measurement) have been shown to detect are less frequently seen in the spinal cord than in the
areas of demyelination.19 At 4·7 T, the proton-density brain.31,32
weighted high-resolution MRI correlated well in regard to The sensitivity of conventional MRI to detect focal
location and shape of the histopathological findings.17 lesions is particularly valuable in the diagnostic con-
Relaxation times were shown to increase with progressive siderations of the early phases of multiple sclerosis. In
demyelination whereas the magnetisation transfer ratio patients with clinically isolated syndrome (CIS) and
decreased.19 radiologically isolated syndrome (RIS), asymptomatic
444 www.thelancet.com/neurology Vol 14 April 2015
Personal View
spinal cord lesions have been described in 30–40% of A B
patients.33 People with RIS seem to be at a high risk of
progression to CIS.33 Some patients with longer disease
duration also show more focal lesions; in particular,
patients with primary progressive multiple sclerosis
might also show an increase in diffuse signal intensity
on T2-weighted and proton-density weighted images
throughout a large portion of the cord.34,35 In patients
with primary progressive multiple sclerosis, cord abnor-
malities are frequently more pronounced than brain
abnormalities. Clinical correlations with MRI spinal cord
lesion counts have been repeatedly low. Most studies
have focused on the analysis of focal lesions, and
attempts to include both focal lesions and diffuse signal
abnormalities have not been any more revealing.9 Even
in a study with a large group of patients, correlations
were not strong enough to make meaningful assessments
on an individual patient basis.9
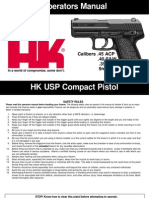
Spinal cord atrophy assessments Figure 1: Biplanar conventional MRI of a 41-year-old female patient with relapsing remitting multiple sclerosis
(A) Sagittal proton-density weighted MRI of the whole spinal cord, with lesions seen as hyperintense areas.
Quantification of the spinal cord cross-sectional area at a (B) The axial images confirm the location of the pathology; lesions are marked with green arrow heads.
high cervical level has been the most reported MRI
measure of cord atrophy.36 Spinal cord atrophy has been
detected in patients at high risk of developing multiple spinal cord lesion load and spinal cord atrophy,
sclerosis (ie, those with cord lesions and additional brain conventional brain MRI lesion burdens were related to
lesions) after a CIS.37 In patients with secondary spinal cord atrophy to various extents, which suggests
progressive multiple sclerosis, the atrophy in the cervical that the reduction in upper cervical cord cross-sectional
cord area is about 16–28%, whereas in patients with area could be a result of T1-hypointense lesions in the
clinically benign disease, spinal cord atrophy was brain rather than lesions of the spinal cord. Furthermore,
considerably less (around 5–8%)36,38. A study on a large the cervical spinal cord cross-sectional area and brain T1-
and diverse cohort (143 healthy controls, 22 CIS, weighted lesion load were the strongest MRI predictors of
101 relapsing remitting multiple sclerosis, 79 secondary disability on the expanded disability status scale (EDSS)
progressive multiple sclerosis, 58 benign multiple score, but atrophy of the spinal cord was more strongly
sclerosis, 75 primary progressive multiple sclerosis) has related to disability (R²=0·564) than spinal cord lesion
substantiated the presence of cervical cord atrophy in load.45 Few studies have assessed to what extent spinal
people with progressive disease, and the relative absence cord atrophy contributes to disability when brain lesion
in patients with benign multiple sclerosis. Spinal cord load and atrophy has been accounted for. Two studies46,47
atrophy was not detected in patients with CIS or with reported spinal cord atrophy to be associated with physical
relapsing remitting multiple sclerosis.39 Klein and disability in regression models, suggesting that it makes
colleagues40 reported increased tissue volumes (when a pronounced independent contribution. A 2 year follow-
normalised for intracranial volumes) in low cervical and up study in 352 patients with multiple sclerosis measured
thoracic cord in patients with relapsing remitting conventional brain and spinal cord MRI parameters in
multiple sclerosis, perhaps attributable to inflammation addition to the annualised percentage brain volume
or oedema associated tissue swelling. Other work has change (aPBVC), and the annualised percentage upper
suggested a rate of cord atrophy in the order of 1–5% per cervical cord cross-sectional area change (aUCCA)
year in people with multiple sclerosis,36,41–43 and cord obtained from the caudal region of the three-dimensional
atrophy seems to be faster in patients with secondary T1-weighted brain MRI acquisition. aUCCA over
progressive multiple sclerosis compared with primary 24 months was highest in patients with secondary
progressive multiple sclerosis.32,44 However, as highlighted progressive multiple sclerosis (–2·2% per year), and was
by the varying results in CIS and relapsing remitting significantly higher in patients with disease progression
multiple sclerosis cohorts, spinal cord atrophy might not (–2·3% per year) than in stable patients (–1·2% per year;
be a linear process. p=0·003). Whereas aPBVC did not differ between
A study on 440 patients with multiple sclerosis subtypes (relapsing remitting multiple sclerosis: –0·42%
(311 relapsing remitting, 92 secondary progressive, and per year; secondary progressive multiple sclerosis: –0·6%
37 primary progressive) confirmed that spinal cord per year; primary progressive multiple sclerosis: –0·46%
atrophy is more pronounced in those with progressive per year), or between progressive and stable patients
disease.45 Although there was no association between (p=0·055).48 Baseline UCCA and aUCCA over 24 months
www.thelancet.com/neurology Vol 14 April 2015 445
Personal View
were reported to contribute to EDSS at month 24, whereas potential to provide a useful and clinically relevant marker
baseline UCCA and number of spinal cord segments of disease progression and offer additional information
with lesions at baseline, but not aUCCA over 24 months, when acquired alongside brain lesion load and brain
were relevant contributors to disease progression.48 This atrophy measures.
study further underlines the feasibility of follow-up
atrophy assessments and their value in provision of New techniques for spinal cord imaging
clinically important information not obtained from brain Magnetisation transfer imaging
MRI analyses. Magnetisation transfer imaging of the spinal cord has
A method for voxel-wise statistical analysis of cord provided substantial insights into focal and diffuse tissue
volume has been developed and validated.49 The abnormalities associated with multiple sclerosis because
investigators showed the regional distribution of cord of its sensitivity to microstructural damage. Magnetisation
atrophy in patients with relapsing remitting multiple transfer imaging is a quantitative MRI technique based
sclerosis versus secondary progressive multiple sclerosis.50 on the interactions between protons in a free environment
Patients with relapsing remitting multiple sclerosis had and motional restricted protons that are bound to
localised clusters of atrophy in the posterior cord, whereas macromolecules. With an off-resonance radiofrequency
patients with secondary progressive multiple sclerosis pulse, the magnetisation of bound protons is saturated
showed a more widespread pattern of cord atrophy, and transferred to the mobile protons, thus reducing the
predominantly in the posterior and lateral cord columns signal intensity of the observable magnetisation.52 Since
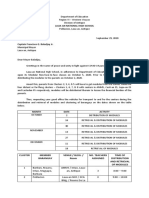
(figure 2). The same approach was used to map the in the CNS the bound protons are mainly associated with
regional distribution of atrophy and T2-hyperintense myelin lipids and proteins, the amount of signal decrease
lesions in the cervical cord of patients with multiple is thought to suggest damage to myelin or to the axonal
sclerosis with different clinical phenotypes.51 Notably, the membranes.19,52,53
spatial distributions of cord atrophy and cord lesions were The magnetisation transfer ratio, calculated from the
not the same for any phenotype,51 suggesting that atrophy magnetisation transfer-on image and magnetisation
is not necessarily the local result of focal demyelination. transfer-off image, is the most common quantitative
Correlations between cord lesion loads and EDSS scores metric used to assess the magnitude of the magnetisation
have been inconsistent and of low strength when transfer effect on a pixel-by-pixel basis (figure 3).
compared with associations of cord atrophy and EDSS Magnetisation transfer maps can subsequently be
(where reported, Spearman correlations range from 0·2 compared between controls and patients with multiple
to 0·7).36,43 Measures of spinal cord atrophy have the sclerosis either by region of interest or by histogram
analysis.54 Several studies55–58 have shown that measure-
ment of the magnetisation transfer ratio in the cervical
A A B C A
C1/C2 C1/C2 cord of patients with multiple sclerosis is feasible and
leads to reliable collection of quantitative MRI data,
L R L R
which is not the case for conventional MRI. These
C3 C3 studies have shown that changes in the magnetisation
L R A L R
transfer ratio of the spinal cord probably occur late in the
C3 course of the disease because no abnormalities were
C4 C4 detected in patients with CIS, relapsing remitting
L R
L R L R multiple sclerosis, or paediatric multiple sclerosis.
Conversely, substantial reductions in histogram-derived
C5 C5
C7 magnetisation transfer ratio were recorded in the spinal
L R L R cord of patients with primary progressive multiple
L R
C6 C6
sclerosis and patients with secondary progressive
P
multiple sclerosis. These cord magnetisation transfer
L R L R
ratios were much lower than those noted in patients
C7 C7 with relapsing remitting multiple sclerosis.59 In patients
L R
with primary progressive multiple sclerosis, disability
L R
A P A P A P was statistically significant according to the EDSS scores,
P P albeit weakly, associated with a composite MR model,
t value 0 6 t value 0 4 t value 0 8
including measures of axonal loss and intrinsic damage
Figure 2: Voxel-wise assessment of the regional distribution of spinal cord atrophy of cervical cord tissue, indicated by a reduced
Sagittal and axial MRI at different cervical cord levels on 45 patients with relapsing remitting multiple sclerosis, magnetisation transfer ratio and signs of cord atrophy.59
26 patients with secondary progression multiple scelerosis and 67 age-matched healthy control subjects. Colour The magnetisation transfer ratio was significantly
coded for t values; p=0·001, data uncorrected only for display reasons. (A) Patients with all subtypes of multiple
sclerosis compared with healthy control subjects. (B) Patients with relapsing remitting multiple sclerosis compared altered in patients with locomotor disability compared
with healthy control subjects. (C) Patients with secondary progressive multiple sclerosis compared with those with with those without (p=0.001).60 Moreover, in patients
relapsing-remitting multiple. A=anterior. C=cervical region. L=left. R=right. P=posterior. with relapsing remitting multiple sclerosis, a moderate
446 www.thelancet.com/neurology Vol 14 April 2015
Personal View
association was identified between baseline spinal cord
A B
magnetisation transfer ratio and disability changes and
relapse rate over 18 months of follow-up.61 MT off
Some technical developments have been introduced to
improve both magnetisation transfer acquisition and
analysis. To overcome the restrictions due to the small size
of the spinal cord and its sensitivity to motion, the use of
three-dimensional gradient-echo sequences, which obtain MT on
high-resolution images with a high signal-to-noise ratio
and a strong magnetisation transfer saturation effect,62 has
been proposed. This approach was applied in a preliminary
study,62 in which magnetisation transfer on and
magnetisation off images were acquired within a single MTR
sequence together to obtain inherently coregistered
magnetisation transfer saturated and unsaturated images. MD FA Diffusion directions
Despite the small patient cohort included in the study, this Figure 3: Magnetisation transfer ratio and diffusion tensor MRI maps of the cervical cord
method was sufficiently sensitive to reveal differences in (A) Magnetisation transfer MRI: axial gradient-echo images of the cervical cord from a patient with relapsing
the average magnetisation transfer ratio and peak location remitting multiple sclerosis. (B) Diffusion tensor MRI obtained from a patient with relapsing remitting multiple
sclerosis showing sagittal MD, left; FA, middle; and diffusion directions (right panel, blue shows diffusion along the
of seven patients with multiple sclerosis compared with caudo-rostral and rostro-caudal direction). Diffusion maps were obtained from a patient with relapsing remitting
healthy control participants. Magnetisation transfer multiple sclerosis. MT=magnetisation transfer. MTR=magnetisation transfer ratio. MD=mean diffusivity.
analysis improved the regional assessment of cord FA=fractional anisotropy.
damage, by measuring the cord grey matter in isolation
from white matter. With this approach, a substantial Diffusion tensor imaging
reduction of average grey matter magnetisation transfer Diffusion MRI has been widely used to study multiple
ratio was recorded in 18 patients with relapsing remitting sclerosis because it can detect and quantify CNS disease-
multiple sclerosis without T2-visible cord lesions,63 which related pathological changes.68 The characteristics of
was also associated with patients’ disability. A further novel diffusion, which can be defined as the random
approach that has been developed to overcome cord translational motion of molecules in a fluid system, are
motion-related problems, which might cause an imperfect changed by several CNS tissue components, including
subtraction between magnetisation-saturated and cell membranes and organelles. The MRI-measured
magnetisation-unsaturated images leading to an unreliable diffusion coefficient of healthy CNS tissues—the
magnetisation transfer ratio, is a new metric to measure apparent diffusion coefficient (ADC)—is lower than the
the magnetisation transfer effect in the cord tissue by ADC of free water.68 Pathological processes that lead to a
using the CSF as an internal magnetisation transfer signal- decrease of barriers that restrict diffusion can lead to an
intensity reference for the spine. This technique needs the increase in ADC values.68 Because the magnitude of
acquisition of only one magnetisation-saturated image, diffusion is also dependent on the direction in which it is
and measures the strength of the signal at each voxel by measured, a more complete characterisation can be
dividing voxel-signal intensity by CSF-signal intensity. obtained from a diffusion tensor (DT),69 a matrix that
This new metric (MTCSF64) was successfully used to accounts for the correlation between molecular displace-
measure tissue damage in the spinal cord of 42 patients ments along orthogonal directions. From the DT,
with multiple sclerosis.65 With a region-of-interest-based parameters that are quantitative and invariant to the
approach, this study showed a substantial MTCSF change choice of reference frame can be derived, including the
in the dorsal and in the lateral columns of these patients, mean diffusivity, which measures the average molecular
which were both associated with sensorimotor impairment motion independent of any tissue directionality, and the
and disability scores. fractional anisotropy (FA), which shows the diffusivity
In a further study, magnetisation transfer ratio abnor- along one spatial direction (figure 3).69 Post-mortem
malities were reported in an area corresponding to the studies in multiple sclerosis have shown that the main
expected location of the pia mater and subpial region in pathological correlates of diffusivity changes are
the outer-cervical spinal cord.66 These outer spinal cord demyelination and axonal loss,53,70 with the correlation
abnormalities were also seen early in the course of with pathological features being stronger for FA than for
multiple sclerosis before cord atrophy was pronounced, diffusivity indices.53,70 One study showed that the DT
and a greater reduction in magnetisation transfer ratio indices in longitudinal diffusivity and radial diffusivity
values was noted in progressive multiple sclerosis. A show a pathological increase, and FA shows a pathological
composite measure, which took into account the cervical decrease in T2-hyperintense lesions. These effects were
cord magnetisation transfer ratio and cross-sectional mainly caused by demyelination, which was corroborated
area, improved the strength of the correlation between by an immunofluorescent assay in which axons were still
cervical cord MRI findings and the EDSS score.67 relatively preserved.71
www.thelancet.com/neurology Vol 14 April 2015 447
Personal View
Using a region-of-interest approach72 in three patients were substantially different, indicating pathological
with multiple sclerosis, increased mean diffusivity and a tissue changes, in patients with multiple sclerosis versus
tendency towards decreased FA in cord lesions of healthy controls, and between the progressive multiple
patients, in comparison with the cord of healthy controls, sclerosis subtypes versus relapsing multiple sclerosis
was reported. By applying sensitivity encoding echo- subtypes, with the exception of parallel diffusivity. In
planar imaging to DT MRI of the cervical cord,73 the multivariable regression models adjusted for age, sex,
extent of cervical cord damage was estimated in patients brain parenchymal fraction, and spinal cord cross-
with multiple sclerosis with different clinical phenotypes. sectional area, the MRI indices independently explained
With a histogram-based approach, 44 patients with variability in hip flexion strength (p<0·01
relapsing remitting multiple sclerosis and secondary for mean diffusivity, perpendicular diffusivity, and
progressive multiple sclerosis had increased mean parallel diffusivity, p=0·07 for FA), vibration sensation
diffusivity and decreased FA of the cervical cord threshold (p=0·04 for FA, p=0·05 for magnetisation
compared with healthy controls. However, no substantial transfer ratio, and p=0·06 for perpendicular diffusivity),
differences in cord DT MRI measures were seen between and EDSS scores (p=0·003 for FA, p=0·03 for mean
the two patient cohorts.74 In the same study, using a diffusivity, p=0·005 for perpendicular diffusivity, and
multivariate linear regression model, cervical cord p=0·02 for magnetisation transfer ratio). The same
average FA and brain average mean diffusivity were method was used on 124 patients with multiple sclerosis82
independent determinants of clinical disability. who were dichotomised into a low-lesion or high-lesion
Patients with primary progressive multiple sclerosis group. Of the patients with low lesion counts, the
also had abnormal mean diffusivity and FA of the cervical microstructural abnormalities (such as small amounts of
cord.40 When compared with secondary progressive demyelination, gliosis and neuronal loss) assessed by
multiple sclerosis,75 patients with benign multiple magnetisation transfer ratio, cross-sectional area, and
sclerosis had milder cervical cord damage. Moreover, in diffusion imaging, were more pronounced than in
patients with benign multiple sclerosis, both cord cross- patients with a high EDSS (≥6) compared with those with
sectional area and FA were independently associated a lower EDSS (<6). In this context, the information on
with the extent of clinical disability,75 thus suggesting that microstructural abnormalities were helpful to understand
DT MRI could contribute to a comprehensive assessment the clinical differences that was not accounted for with
of spinal cord damage. the conventional MRI approach.82
Several reports76–78 used a region-of-interest-based At present, only one 2-year follow-up study has assessed
approach to quantify damage within the different cervical longitudinal changes by use of cord DT MRI in a large
spinal cord compartments (ie, white matter of the different sample of patients with multiple sclerosis.83 The authors
cord columns and central grey matter). These studies showed that cervical cord cross-sectional area and FA
showed substantial DT MRI changes in diffusion in both decreased, and cervical cord mean diffusivity increased
the normal-appearing white matter and grey matter in the during follow-up. Cord FA decrease, but not cord cross-
spinal cord of patients with multiple sclerosis compared sectional area and mean diffusivity, was substantially
with healthy controls. These changes were more severe in higher in patients with primary progressive multiple
cord macroscopic lesions seen on the MRI than in the sclerosis than in those with either relapsing remitting or
normal-appearing white matter. secondary progressive disease. In this study, multiple
Cervical spinal cord DT tractography has been combined sclerosis cord pathological changes were also proved
with proton MR spectroscopy to estimate cord damage independent of concomitant brain changes and were
occurring in 14 patients with spinal relapses.79 Compared associated with medium-term disability accrual.
with controls, these patients had reductions in
N-acetylaspartate concentrations, which is a specific fMRI of the spinal cord
marker in vivo for neuronal health and integrity, con- Despite being technically challenging, a spinal cord spin-
nectivity, and FA of the lateral corticospinal tracts and echo based fMRI with signal enhancement by
posterior tracts. These measurements were shown to extravascular proton contrast has been shown to provide
correlate with acute disability. The 6 month longitudinal reliable data in human beings.84–86 Cord signal changes
assessment of these patients showed that low (more can be detected during different motor and sensory
healthy) radial diffusivity of the corticospinal tract at paradigms85 (figure 4). Spinal cord fMRI in patients with
baseline was associated with improved clinical outcome.80 relapse-onset multiple sclerosis showed an altered
Another study compared different quantitative cervical pattern of functional activations in the cervical cord
spinal cord metrics with system specific measurements during both tactile and proprioceptive stimuli of the right
and general clinical measures in 129 patients with upper limb.84,85 Functional changes in the cervical cord
multiple sclerosis.81 The authors calculated spinal cord associated with tactile stimulation of the right hand were
cross-sectional area, FA, mean diffusivity, perpendicular assessed in a cohort 49 of patients with relapsing
diffusivity (λ⊥), parallel diffusivity (λ||), and magnetisation remitting or secondary progressive multiple sclerosis.86
transfer ratio on axial slices at C3–C4. All MRI indices Greater cervical cord activation was present in patients
448 www.thelancet.com/neurology Vol 14 April 2015
Personal View
with relapsing remitting or secondary progressive
A C5 C5/6 C6 C6/7 C7 C7/T1 T1
multiple sclerosis compared with controls.86 Moreover,
severely disabled patients showed an enhancement of L R
cord activity not only compared with controls, but also
compared with patients with less clinical disability (ie,
EDSS ≤3·5).86 Tactile-associated cervical cord over- B
activation was also recorded in patients with primary
L R
progressive multiple sclerosis.87
Compared with healthy controls, both relapse-onset
and patients with primary progressive multiple sclerosis 1·68 4
showed altered distribution of tactile-associated cervical t value
cord activity.84,87 In the expected regions of neuronal Figure 4: Activation maps of an fMRI on the spinal cord
involvement for a tactile stimulation of the palm of the Activation maps (colour-coded for t values) of the cervical cord projected onto
right hand, patients showed a functional lateralisation of axial proton-density-weighted spin-echo images from C5 to T1 from a healthy
control (A) and a patient with multiple sclerosis (B) during a tactile stimulation
cord activity, which was predominant in the cord side
of the palm of the right hand. fMRI=functional MRI. C=cervical region.
ipsilateral to the stimulus, and a more frequent activation T=thoracic region. L=left. R=right.
of the posterior quadrants than the anterior cord
quadrants.84,87 Activity of the anterior cord seemed to be
more prevalent in patients with multiple sclerosis than in ¹H-magnetic resonance spectroscopy
healthy controls, on both the ipsilateral and contralateral ¹H-MRS of the spinal cord is technically challenging90–92
sides.84,87 Additionally, unlike healthy controls, patients and patients with multiple sclerosis have rarely been
with multiple sclerosis did not show differential activation analysed with brain ¹H-MRS studies.79,93–97 Until now, the
between the right and the left hemicords.84,87 The increased metabolite that has been most studied in the spinal cord
activation of the cervical cord in patients with relapsing is N-acetylaspartate (total N-acetylaspartate [tNAA], equal
remitting or primary progressive multiple sclerosis was to NAA + NAA-glutamate).98 One study has detected a
associated with cord structural damage, measured with linear decrease in tNAA concentrations in the upper
DT MRI, whereas no association was identified with cord cervical cord with ageing in healthy participants,
atrophy and cord-T2 focal-lesions.86,87 suggesting that this tNAA decline shows age-related
In a comparison of 17 healthy controls and patients neuroaxonal degeneration.92
with progressive multiple sclerosis (18 secondary Despite technical differences in the methods applied to
progressive, 16 primary progressive), both progressive acquire spectra from the spinal cord, which include the
multiple sclerosis forms had an over-recruitment of the use of MR scanners with different magnetic field
cervical cord, which was more pronounced in secondary strengths, and differences in the clinical characteristics
progressive than primary progressive multiple sclerosis, of the patient groups studied (table), reports so far have
despite similar levels of cord structural damage. However, consistently shown a reduction in the tNAA concentration
patients with secondary progressive multiple sclerosis in patients with multiple sclerosis compared with healthy
had more pronounced focal and diffuse brain damage, controls, which varied between 21% and 39%79,94,96,97 (table,
which would advocate for an effect of supraspinal brain figure 5). This reduction in tNAA concentration could be
abnormalities on the recorded cord activation changes.88 clinically relevant, as it has been shown to correlate with
Rocca and coworkers89 investigated the association the cerebellar function score94 and performance on the
between fatigue and cervical cord abnormalities by nine-hole peg test.79
obtaining spinal cord fMRI in 20 controls, 15 patients When the temporal concentration of tNAA after an
with multiple sclerosis without fatigue, and 20 patients acute cervical cord lesion was investigated, as the acute
with multiple sclerosis with fatigue. In response to tactile lesion resolved the tNAA concentration partly recovered,91
stimulation, the patients with multiple sclerosis showed mirroring the temporal behaviour of NAA described in
more widespread cord activation than controls, but this brain studies.100,101 These findings suggest that reduced
increase was less pronounced in patients with fatigue tNAA indicates not only reduced neuronal integrity but
and was related to the severity of fatigue. The authors also metabolic dysfunction.102 Additional evidence for this
suggest that the differences in cord fMRI activation are metabolic component of tNAA comes from the reported
caused by changes in cortical inhibition and changes in absence of correlation between spinal cord tNAA
spinal interneuron activation, which are likely to serve as concentration and spinal cord atrophy.79,93 Thus, these
compensatory mechanisms for the loss of resources to results suggest that differences in tNAA concentrations
maintain normal function. In patients with fatigue, such are seen in pathological processes that are different from
compensatory mechanisms might be compromised, but neuroaxonal degeneration, which is known to be well
local structural cord damage did not seem to be a relevant captured by in-vivo measurements of spinal cord atrophy.
factor to explain the different activation patterns in The partial recovery of tNAA concentrations after an
patients with and without fatigue.89 acute spinal cord relapse was associated with the extent
www.thelancet.com/neurology Vol 14 April 2015 449
Personal View
Scanner Spinal cord Type of MS EDSS Tissue included in the Reduced NAA in patients versus
level spectroscopic voxel controls
Kendi et al (2004)93 1·5 T C3–C7 Not reported Not reported NAWM Yes, but reduction not reported
Blamire et al (2007)94 2·0 T C3 4 RR, 7 SP 4·5 Not reported 32%
Ciccarelli et al (2007)79 1·5 T C1–C3 13 RR, 1 SP 4·0 Acute lesions 39%
Marliani et al (2010)96 3·0 T C2–C3 15 RR Not reported Chronic lesions 21% (NAA:Cho)
Ciccarelli et al (2013)99 3·0 T C1–C3 10 RR, 5 NMO Not reported Chronic lesions 29%
MS=multiple sclerosis. EDSS=expanded disability status scale. NAA=N-acetylaspartate. NAWM=normal appearing white matter. RR=relapsing remitting. SP=secondary
progressive. Cho=choline-containing compounds. NMO=neuromyelitis optica.
Table: Magnetic resonance imaging studies of the spinal cord in patients with multiple sclerosis
Cho NAA
A C
Cr
Cho
D mIns
NAA
Cr
lipids
4·0 3·8 3·6 3·4 3·2 3·0 2·8 2·6 2·4 2·2 2·0 1·8 1·6 1·4 1·2 1·0 0·8 0·6 0·4
Chemical shift (ppm)
Figure 5: Cervical cord ¹H-spectroscopy with a 3 T MR system
Spectroscopic voxel located on an axial (A) and sagittal (B) plane T2-weighted images between C2 and C3. Spectra obtained with LCModel analysis of a healthy control
(C) and a patient with relapsing remitting multiple sclerosis (D). The patient spectrum showed reduced NAA/Cr and NAA/Cho ratios, and increased mIns/Cr and Cho/Cr
ratios; lipids are also visible in the spectrum of the patient with multiple sclerosis. MR=magnetisation transfer. Cho=choline. Cr=creatine plus phosphocreatine.
NAA=N-acetylasparate. mIns= myo-inositol. Red line demonstrates the identified peaks from the MRS data, the grey line defines the baseline. Reproduced with
permission from Anna Federica Marliani (Neuroradiology Department, Bellaria Hospital, Bologna, Italy).
of clinical recovery, suggesting that improved neuronal be measured with ¹H-MRS, such as choline-containing
metabolism could be a mechanism of tissue repair that compounds, creatine plus phosphocreatine and myo-
leads to clinical improvement.95 inositol, has been noted to be consistently different in
These findings support the use of spinal cord ¹H-MRS patients with multiple sclerosis when compared with
to obtain insights into the mechanisms of damage and healthy controls (figure 5).79,93,96,99 However, some
repair of the CNS. None of the other metabolites that can associations between acute disability and these metabolite
450 www.thelancet.com/neurology Vol 14 April 2015
Personal View
concentrations have been described and should be studied
further.96 Additionally, reduced myo-inositol normalised to Search strategy and selection criteria
creatine plus phosphocreatine was recorded in References for this Personal View were identified through
neuromyelitis optica lesions of the spinal cord compared searches of PubMed with the search terms (and synonyms)
with multiple sclerosis lesions and healthy cord, possibly “spinal cord MRI”, and “spinal cord pathology”, “T2-weighted
suggesting astrocytic damage in neuromyelitis optica.99 MRI”, “spinal cord atrophy”, “magnetisation transfer”, and the
These findings are in agreement with pathological key terms “multiple sclerosis”, “diffusion weighted MRI”,
evidence that neuromyelitis optica is an autoimmune “functional MRI” and/or “¹H-spectroscopy” from 1990 to July,
astrocytopathy, in which the damage to astrocytes is 2014. We also searched the abstract databases of the
substantial and widespread.103 European Committee for Treatment and Research in Multiple
Sclerosis congress 2012 and 2013, American Academy of
Conclusions and future directions Neurology congress 2012 and 2013, and International
The progress of MRI instrumentation provides a major Society for Magnetic Resonance in Medicine congress 2013
advantage for conventional spinal cord imaging with a and 2014 for relevant studies. The abstracts of retrieved
better signal-to-noise ratio and improved spatial citations were reviewed and prioritised by relevant content,
resolution, which has already helped modern quantitative and by the quality of evidence reported. From the large
MRI techniques further our understanding of multiple number of manuscripts, we included mainly studies with a
sclerosis. It is now possible to identify diffuse and focal prospective design. Only reports in English were reviewed.
changes in an examination of the whole spinal cord with
conventional MRI. MRI in both axial and sagittal planes
might be best suited to detect focal lesions in the cord as longitudinal studies in large patient cohorts would be
diagnostic information or indicators of disease activity. It useful to characterise the disease dynamics and support
would be of great value to conventional and advanced and extend the results from cross-sectional studies.
techniques if there was further technical progress to Present findings suggest that different pathological
reduce motion artifacts for spinal cord MRI. processes that contribute to clinical disability could be
Histopathological studies have shown that conventional better shown, including quantitative measures like
MRI is highly sensitive to focal demyelination and less magnetisation transfer ratio or DTI indices with cord
sensitive to visualise axonal loss or more subtle degrees of atrophy markers, in addition to conventional spinal cord
demyelination. Cord atrophy, intrinsic microstructural MRI. One report showed high-resolution cervical cord
cord damage, and adaptation occur largely independent MRI at 7 T with an increase of nearly 4·2-times on T2-
of focal spinal cord lesion load, underlining their weighted spinal cord MRI at 7 T relative to 3 T, which
relevance in depicting the true burden of disease. Cross- should not only be useful to provide more anatomical
sectional and longitudinal studies on cervical cord atrophy detail, but will surely help quantitative MRI approaches
have shown that large cohorts of patients with multiple in the future.104
sclerosis can be useful to appreciate the information Future technical developments, which will be associated
provided by spinal cord atrophy, potentially independent with the use of higher-magnetic fields, might make it
from that of brain MRI findings. The more advanced possible to cover not only a larger area of the spine,105 but
techniques have so far focused on the technically most also to obtain spectra from the lower cervical spine and
accessible area—the cervical spinal cord. Although thoracic levels,92 and to quantify new metabolites, such as
¹H-MRS is technically challenging and has been mainly glutamate and glutamine, in a method that could be
used in small studies, it offers high specificity particularly applied in the clinic.106 One study with specially designed
on axonal integrity. Magnetisation transfer and DTI motion and instability correction methods for applications
metrics are well known quantitative techniques for brain to the spinal cord and a custom-made, neck coil array,
imaging. In the spinal cord, both techniques are sensitive showed a reliable quantification of glutathione in all, and
to demyelination and axonal loss that is not visible on aspartate, lactate, and GABA in some of the volunteers.107
conventional spinal cord MRI; however, their specificity The combination of NAA concentration with other
to differentiate demyelination and axonal loss is limited. imaging measures sensitive to structural damage might
Microscopic changes and spinal cord atrophy tend to allow exploration of the clinical significance of the
become apparent after longer disease durations, and metabolic component of tNAA.108 These factors, together
could be very small or not detectable in the early stages of with possible increases in ¹H-MRS sensitivity and spatial
multiple sclerosis. However, changes of magnetisation resolution, might make spinal cord ¹H-MRS an invaluable
transfer and DTI metrics seem to be clinically meaningful, technique not only for diagnostic and prognostic reasons,
as they contribute to reported clinical differences in but also for understanding in vivo the neurobiological
patients with a similar lesion burden on conventional mechanisms of injury and repair.
spinal cord MRI. In this regard, quantitative MRI Contributors
measures show the ability to provide clinically relevant AG, MF, LK, and FB decided on the structure of the Personal View. All
information beyond MRI lesion load. Multicentre and authors participated in the preparation of a first draft of the manuscript,
www.thelancet.com/neurology Vol 14 April 2015 451
Personal View
tables and figures. AG and MF prepared a first version of the 4 McGowan JC. Technical issues for MRI examination of the spinal
manuscript, contributed to writing of subsequent versions, helped to cord. J Neurol Sci 2000; 172 (suppl 1): S27–31.
select references, and reviewed the final version of the manuscript. 5 Taber KH, Herrick RC, Weathers SW, Kumar AJ, Schomer DF,
Hayman LA. Pitfalls and artifacts encountered in clinical MR
MAGNIMS Study Group Steering Committee imaging of the spine. Radiographics 1998; 18: 1499–521.
A Rovira, N de Stefano, X Montalban, F Barkhof, C Enzinger, M Filippi,
6 Kidd D, Thorpe JW, Thompson AJ, et al. Spinal cord MRI using
J Frederiksen, L Kappos, O Ciccarelli, J Palace, H Vrenken, M A Rocca, multi-array coils and fast spin echo. II. Findings in multiple
T Yousry. sclerosis. Neurology 1993; 43: 2632–37.
Declaration of interests 7 Tartaglino LM, Friedman DP, Flanders AE, Lublin FD, Knobler RL,
AG has received honoraria for lecturing, travel expenses for attending Liem M. Multiple sclerosis in the spinal cord: MR appearance and
meetings, and financial support for research from Bayer Schering, correlation with clinical parameters. Radiology 1995; 195: 725–32.
Biogen Idec, Merck Serono, Novartis, and TEVA Neurosciences. FA has 8 Thorpe JW, Kidd D, Moseley IF, et al. Spinal MRI in patients with
received research supports from the Italian Ministry of Health and suspected multiple sclerosis and negative brain MRI. Brain 1996;
119: 709–14.
AriSLA—Fondazione Italiana di Ricerca per la Sclerosi Laterale
Amiotrofica, and speaker honoraria from Biogen Idec and Serono 9 Weier K, Mazraeh J, Naegelin Y, et al. Biplanar MRI for the assessment
of the spinal cord in multiple sclerosis. Mult Scler 2012; 18: 1560–69.
Symposia International Foundation. DC has received honoraria from
Bayer, Teva and the Serono Symposia International Foundation for 10 Lycklama à Nijeholt GJ, Barkhof F, Castelijns JA, et al.
Comparison of two MR sequences for the detection of multiple
faculty-led education work, Teva for advisory board work, and holds stock
sclerosis lesions in the spinal cord. AJNR Am J Neuroradiol. 1996;
in GlaxoSmithKline. MAR has received speaker honoraria from Biogen 17: 1533–38.
Idec, Serono Symposia International Foundation, Genzyme, and
11 Lycklama à Nijeholt GJ, Castelijns JA, Weerts J, et al. Sagittal MR of
Novartis and receives research support from Italian Ministry of Health multiple sclerosis in the spinal cord: fast versus conventional spin-
and Fondazione Italiana Sclerosi Multipla. MF serves on scientific echo imaging. AJNR Am J Neuroradiol. 1998; 19: 355–60.
advisory boards for Teva Pharmaceutical Industries; has received 12 Bot JC, Barkhof F, Lycklama à Nijeholt G, et al. Differentiation of
compensation for consulting services and/or speaking activities from multiple sclerosis from other inflammatory disorders and
Bayer Schering Pharma, Biogen Idec, Merck Serono, and Teva cerebrovascular disease: value of spinal MR imaging. Radiology
Pharmaceutical Industries; and receives research support from Bayer 2002; 223: 46–56.
Schering Pharma, Biogen Idec, Merck Serono, Teva Pharmaceutical 13 Bot JC, Barkhof F, Polman CH, et al. Spinal cord abnormalities in
Industries, Italian Ministry of Health, Fondazione Italiana Sclerosi recently diagnosed MS patients: added value of spinal MRI
Multipla, Cure PSP, Alzheimer’s and Drug Discovery Foundation, and examination. Neurology 2004; 62: 226–33.
the Jacques and Gloria Gossweiler Foundation (Switzerland). OC has 14 Gilmore CP, DeLuca GC, Bö L, et al. Spinal cord neuronal
received research funding from the Wellcome Trust, MS Society of Great pathology in multiple sclerosis. Brain Pathol 2009; 19: 642–49.
Britain and Northern Ireland, UCL Biomedical Research Centre, and 15 Adams RD, Kubik CS. The morbid anatomy of the demyelinative
Engineering and Physical Sciences Research Council. She has also disease. Am J Med 1952; 12: 510–46.
received speaker honoraria from Bayer. AB received travel support from 16 Ikuta F, Zimmerman HM. Distribution of plaques in seventy
Biogen Idec. PE has received travel expenses from Bayer Health Care. autopsy cases of multiple sclerosis in the United States. Neurology
FB serves as a consultant for Bayer Shering Pharma, Sanofi-Aventis, 1976; 26: 26–28.
Biogen-Idec, UCB, Merck-Serono, Novartis, and Roche. LK has 17 Nijeholt GJ, Bergers E, Kamphorst W, et al. Post-mortem high-
participated in the past 36 months as member or chair of planning and resolution MRI of the spinal cord in multiple sclerosis: a correlative
steering committees or advisory boards in corporate-sponsored clinical study with conventional MRI, histopathology and clinical
trials in multiple sclerosis and other neurological diseases. The phenotype. Brain 2001; 124: 154–66.
sponsoring pharmaceutical companies for these trials include: Actelion, 18 Gilmore CP, Bö L, Owens T, Lowe J, Esiri MM, Evangelou N. Spinal
Addex, Advancell, Allozyne, BaroFold, Bayer Health Care cord gray matter demyelination in multiple sclerosis-a novel pattern
Pharmaceuticals, Bayer Schering Pharma, Bayhill, Biogen Idec, Biotica, of residual plaque morphology. Brain Pathol 2006; 16: 202–08.
CLC Behring, Elan, Genentech, GeNeuro SA, Genmab, Genmark, 19 Bot JC, Blezer EL, Kamphorst W, et al. The spinal cord in multiple
Genzyme, GlaxoSmithKline, Johnson & Johnson, Lilly, Merck Serono, sclerosis: relationship of high-spatial-resolution quantitative MR
imaging findings to histopathologic results. Radiology 2004;
Mitsubishi Pharma, Novartis, Novo Nordisk, Octapharma, Peptimmune,
233: 531–40.
Praxicon, Roche, Sanofi-Aventis, Santhera, Siemens, Teva, UCB,
20 Bergers E, Bot JC, De Groot CJ, et al. Axonal damage in the spinal
Xenoport and Wyeth. He is principal investigator for the following drug
cord of MS patients occurs largely independent of T2 MRI lesions.
studies: BOLD, BOLD EXT., EXPAND (BAF312, Novartis), DECIDE, Neurology 2002; 59: 1766–71.
DECIDE EXT. (Daclizumab, Biogen Idec), ENDORSE (BG00012, Biogen
21 Gilmore CP, Geurts JJ, Evangelou N, et al. Spinal cord grey matter
Idec), FINGORETT, FTY-UMBRELLA, INFORMS, INFORMS EXT lesions in multiple sclerosis detected by post-mortem high field MR
LONGTERM. (Fingolimod, Novartis), OCRELIZUMAB PHASE II EXT., imaging. Mult Scler 2009; 15: 180–88.
OPERA, ORATORIO (Ocrelizumab, Roche), STRATA EXT. 22 Gilmore CP, DeLuca GC, Bö L, et al. Spinal cord atrophy in
(Natalizumab, Biogen Idec), and TERIFLUNOMIDE EXT. multiple sclerosis caused by white matter volume loss. Arch Neurol
(Teriflunomide, Sanofi-Aventis). He has also lectured at medical 2005; 62: 1859–62.
conferences or in public on various aspects of the diagnosis and 23 Evangelou N, DeLuca GC, Owens T, Esiri MM. Pathological study of
management of multiple sclerosis. In many cases these talks have been spinal cord atrophy in multiple sclerosis suggests limited role of
sponsored by unrestricted educational grants to his institution from one local lesions. Brain 2005; 128: 29–34.
or another of the above listed companies. Honoraria and other payments 24 DeLuca GC, Williams K, Evangelou N, Ebers GC, Esiri MM. The
for all these activities have been exclusively used for funding of research contribution of demyelination to axonal loss in multiple sclerosis.
of his department. JCWB and PV declare no competing interests. Brain 2006; 129: 1507–16.
25 Bjartmar C, Kidd G, Mörk S, Rudick R, Trapp BD. Neurological
References
disability correlates with spinal cord axonal loss and reduced
1 Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for
N-acetyl aspartate in chronic multiple sclerosis patients. Ann Neurol
multiple sclerosis: 2010 revisions to the McDonald criteria.
2000; 48: 893–901.
Ann Neurol 2011; 69: 292–302.
26 Philpott C, Brotchie P. Comparison of MRI sequences for
2 Simon JH, Li D, Traboulsee A, et al. Standardized MR imaging
evaluation of multiple sclerosis of the cervical spinal cord at 3 T.
protocol for multiple sclerosis: consortium of MS Centers
Eur J Radiol 2011; 80: 780–85.
consensus guidelines. Am J Neuroradiol 2006; 27: 455–61.
27 Hittmair K, Mallek R, Prayer D, Schindler EG, Kollegger H. Spinal
3 Bot JC, Barkhof F. Spinal-cord MRI in multiple sclerosis:
cord lesions in patients with multiple sclerosis: comparison of MR
conventional and nonconventional MR techniques.
pulse sequences. AJNR Am J Neuroradiol 1996; 17: 1555–65.
Neuroimaging Clin N Am 2009; 19: 81–99.
452 www.thelancet.com/neurology Vol 14 April 2015
Personal View
28 Lycklama G, Thompson A, Filippi M, et al. Spinal-cord MRI in 51 Rocca MA, Valsasina P, Damjanovic D, et al. Voxel-wise mapping of
multiple sclerosis. Lancet Neurol 2003; 2: 555–62. cervical cord damage in multiple sclerosis patients with different
29 Gass A, Filippi M, Rodegher ME, Schwartz A, Comi G, clinical phenotypes. J Neurol Neurosurg Psychiatry 2013; 84: 35–41.
Hennerici MG. Characteristics of chronic MS lesions in the 52 Ropele S, Fazekas F. Magnetization transfer MR imaging in
cerebrum, brainstem, spinal cord, and optic nerve on T1-weighted multiple sclerosis. Neuroimaging Clin N Am 2009; 19: 27–36.
MRI. Neurology 1998; 50: 548–50. 53 Mottershead JP, Schmierer K, Clemence M, et al. High field MRI
30 Silver NC, Good CD, Sormani MP, et al. A modified protocol to correlates of myelin content and axonal density in multiple
improve the detection of enhancing brain and spinal cord lesions in sclerosis—a post-mortem study of the spinal cord. J Neurol 2003;
multiple sclerosis. J Neurol 2001; 248: 215–24. 250: 1293–301.
31 Thorpe JW, Kidd D, Moseley IF, et al. Serial gadolinium-enhanced 54 Filippi M, Rocca MA. Magnetization transfer magnetic resonance
MRI of the brain and spinal cord in early relapsing-remitting imaging of the brain, spinal cord, and optic nerve. Neurotherapeutics
multiple sclerosis. Neurology 1996; 46: 373–78. 2007; 4: 401–13.
32 Kidd D, Thorpe JW, Kendall BE, et al. MRI dynamics of brain and 55 Rovaris M, Gallo A, Riva R, et al. An MT MRI study of the cervical
spinal cord in progressive multiple sclerosis. cord in clinically isolated syndromes suggestive of MS. Neurology
J Neurol Neurosurg Psychiatry 1996; 60: 15–19. 2004; 63: 584–85.
33 Okuda DT, Mowry EM, Cree BA, et al. Asymptomatic spinal cord 56 Filippi M, Bozzali M, Horsfield MA, et al. A conventional and
lesions predict disease progression in radiologically isolated magnetization transfer MRI study of the cervical cord in patients
syndrome. Neurology 2011; 76: 686–92. with MS. Neurology 2000; 54: 207–13.
34 Lycklama à Nijeholt GJ, Barkhof F, Scheltens P, et al. MR of the 57 Rovaris M, Judica E, Ceccarelli A, et al. Absence of diffuse cervical
spinal cord in multiplesclerosis: relation to clinical subtype and cord tissue damage in early, non-disabling relapsing-remitting MS:
disability. AJNR Am J Neuroradiol. 1997; 18: 1041–48. a preliminary study. Mult Scler 2008; 14: 853–56.
35 Nijeholt GJ, van Walderveen MA, Castelijns JA, et al. Brain and 58 Mezzapesa DM, Rocca MA, Falini A, et al. A preliminary diffusion
spinal cord abnormalities in multiple sclerosis. Correlation between tensor and magnetization transfer magnetic resonance imaging
MRI parameters, clinical subtypes and symptoms. Brain 1998; study of early-onset multiple sclerosis. Arch Neurol 2004; 61: 366–68.
121: 687–97. 59 Rovaris M, Bozzali M, Santuccio G, et al. In vivo assessment of the
36 Losseff NA, Webb SL, O’Riordan JI, et al. Spinal cord atrophy and brain and cervical cord pathology of patients with primary
disability in multiple sclerosis. A new reproducible and sensitive progressive multiple sclerosis. Brain 2001; 124: 2540–49.
MRI method with potential to monitor disease progression. Brain 60 Bozzali M, Rocca MA, Iannucci G, Pereira C, Comi G, Filippi M.
1996; 119: 701–08. Magnetization-transfer histogram analysis of the cervical cord in
37 Brex PA, Leary SM, O’Riordan JI, et al. Measurement of spinal cord patients with multiple sclerosis. AJNR Am J Neuroradiol 1999;
area in clinically isolated syndromes suggestive of multiple 20: 1803–08.
sclerosis. J Neurol Neurosurg Psychiatry 2001; 70: 544–47. 61 Charil A, Caputo D, Cavarretta R, Sormani MP, Ferrante P,
38 Filippi M, Campi A, Colombo B, et al. A spinal cord MRI study of Filippi M. Cervical cord magnetization transfer ratio and clinical
benign and secondary progressive multiple sclerosis. J Neurol 1996; changes over 18 months in patients with relapsing-remitting
243: 502–05. multiple sclerosis: a preliminary study. Mult Scler 2006;
39 Rocca MA, Horsfield MA, Sala S, et al. A multicenter assessment of 12: 662–65.
cervical cord atrophy among MS clinical phenotypes. Neurology 62 Hickman SJ, Hadjiprocopis A, Coulon O, Miller DH, Barker GJ.
2011; 76: 2096–102. Cervical spinal cord MTR histogram analysis in multiple sclerosis
40 Klein JP, Arora A, Neema M, et al. A 3T MR imaging investigation using a 3D acquisition and a B-spline active surface segmentation
of the topography of whole spinal cord atrophy in multiple sclerosis. technique. Magn Reson Imaging 2004; 22: 891–95.
AJNR Am J Neuroradiol 2011; 32: 1138–42. 63 Agosta F, Pagani E, Caputo D, Filippi M. Associations between
41 Furby J, Hayton T, Altmann D, et al. A longitudinal study of MRI- cervical cord gray matter damage and disability in patients with
detected atrophy in secondary progressive multiple sclerosis. multiple sclerosis. Arch Neurol 2007; 64: 1302–05.
J Neurol 2010; 257: 1508–16. 64 Smith SA, Golay X, Fatemi A, et al. Magnetization transfer
42 Rashid W, Davies GR, Chard DT, et al. Upper cervical cord area in weighted imaging in the upper cervical spinal cord using
early relapsing-remitting multiple sclerosis: cross-sectional study of cerebrospinal fluid as intersubject normalization reference
factors influencing cord size. J Magn Reson Imaging 2006; 23: 473–76. (MTCSF imaging). Magn Reson Med 2005; 54: 201–06.
43 Rashid W, Davies GR, Chard DT, et al. Increasing cord atrophy in 65 Zackowski KM, Smith SA, Reich DS, et al. Sensorimotor
early relapsing-remitting multiple sclerosis: a 3 year study. dysfunction in multiple sclerosis and column-specific
J Neurol Neurosurg Psychiatry 2006; 77: 51–55. magnetization transfer-imaging abnormalities in the spinal cord.
44 Stevenson VL, Leary SM, Losseff NA, et al. Spinal cord atrophy and Brain 2009; 132: 1200–09.
disability in MS: a longitudinal study. Neurology 1998; 51: 234–38. 66 Kearney H, Yiannakas MC, Samson RS, Wheeler-Kingshott CA,
45 Lukas C, Sombekke MH, Bellenberg B, et al. Relevance of spinal Ciccarelli O, Miller DH. Investigation of magnetization transfer
cord abnormalities to clinical disability in multiple sclerosis: MR ratio-derived pial and subpial abnormalities in the multiple
imaging findings in a large cohort of patients . Radiology 2013; sclerosis spinal cord. Brain 2014; 137: 2456–68.
269: 542–52. 67 Lycklama à Nijeholt GJ, Castelijns JA, Lazeron RH, et al.
46 Bonati U, Fisniku LK, Altmann DR, et al. Cervical cord and brain Magnetization transfer ratio of the spinal cord in multiple sclerosis:
grey matter atrophy independently associate with long-term MS relationship to atrophy and neurologic disability. J Neuroimaging
disability. J Neurol Neurosurg Psychiatry 2011; 82: 471–72. 2000; 10: 67–72.
47 Cohen AB, Neema M, Arora A, et al. The relationships among MRI- 68 Rovaris M, Agosta F, Pagani E, Filippi M. Diffusion tensor MR
defined spinal cord involvement, brain involvement, and disability imaging. Neuroimaging Clin N Am 2009; 19: 37–43.
in multiple sclerosis. J Neuroimaging 2012; 22: 122–28. 69 Pierpaoli C, Basser PJ. Toward a quantitative assessment of
48 Lukas C, Knol DL, Sombekke MH,et al. Cervical spinal cord volume diffusion anisotropy. Magn Reson Med 1996; 36: 893–906.
loss is related to clinical disability progression in multiple sclerosis. 70 Schmierer K, Wheeler-Kingshott CA, Boulby PA, et al. Diffusion
J Neurol Neurosurg Psychiatry 2014; published online Jun 27. tensor imaging of post mortem multiple sclerosis brain.
DOI: 10.1136/jnnp-2014-308021. Neuroimage 2007; 35: 467–77.
49 Valsasina P, Horsfield MA, Rocca MA, Absinta M, Comi G, 71 Zollinger LV, Kim TH, Hill K, Jeong EK, Rose JW. Using diffusion
Filippi M. Spatial normalization and regional assessment of cord tensor imaging and immunofluorescent assay to evaluate the
atrophy: voxel-based analysis of cervical cord 3D T1-weighted pathology of multiple sclerosis. J Magn Reson Imaging 2011;
images. AJNR Am J Neuroradiol 2012; 33: 2195–200. 33: 557–64.
50 Valsasina P, Rocca MA, Horsfield MA, et al. Regional cervical cord 72 Clark CA, Werring DJ, Miller DH. Diffusion imaging of the spinal
atrophy and disability in multiple sclerosis: a voxel-based analysis. cord in vivo: estimation of the principal diffusivities and application
Radiology 2013; 266: 853–61. to multiple sclerosis. Magn Reson Med 2000; 43: 133–38.
www.thelancet.com/neurology Vol 14 April 2015 453
Personal View
73 Cercignani M, Horsfield MA, Agosta F, Filippi M. Sensitivity- 92 Abdel-Aziz K, Solanky BS, Yiannakas MC, et al. Age-related changes
encoded diffusion tensor MR imaging of the cervical cord. in metabolite concentrations in the normal spinal cord. PLoS ONE
AJNR Am J Neuroradiol 2003; 24: 1254–56. 2014; published online Oct 13. DOI:10.1371/journal.pone.0105774.
74 Valsasina P, Rocca MA, Agosta F, et al. Mean diffusivity and 93 Kendi AT, Tan FU, Kendi M, Yilmaz S, Huvaj S, Tellioğlu S. MR
fractional anisotropy histogram analysis of the cervical cord in MS spectroscopy of cervical spinal cord in patients with multiple
patients. Neuroimage 2005; 26: 822–28. sclerosis. Neuroradiology 2004; 46: 764–69.
75 Benedetti B, Rocca MA, Rovaris M, et al. A diffusion tensor MRI 94 Blamire AM, Cader S, Lee M, Palace J, Matthews PM. Axonal
study of cervical cord damage in benign and secondary progressive damage in the spinal cord of multiple sclerosis patients detected by
multiple sclerosis patients. J Neurol Neurosurg Psychiatry 2010; magnetic resonance spectroscopy. Magn Reson Med 2007;
81: 26–30. 58: 880–85.
76 Ohgiya Y, Oka M, Hiwatashi A, et al. Diffusion tensor MR imaging 95 Ciccarelli O, Altmann DR, McLean MA, et al. Spinal cord repair in
of the cervical spinal cord in patients with multiple sclerosis. MS: does mitochondrial metabolism play a role? Neurology 2010;
Eur Radiol 2007; 17: 2499–504. 74: 721–27.
77 Ohgiya Y, Oka M, Hiwatashi A, et al. Diffusion tensor MR imaging 96 Marliani AF, Clementi V, Albini Riccioli L, et al. Quantitative
of the cervical spinal cord in patients with multiple sclerosis. cervical spinal cord 3T proton MR spectroscopy in multiple
Eur Radiol 2007; 17: 2499–504. sclerosis. AJNR Am J Neuroradiol 2010; 31: 180–84.
78 Cruz LC Jr, Domingues RC, Gasparetto EL. Diffusion tensor 97 Henning A, Schär M, Kollias SS, Boesiger P, Dydak U. Quantitative
imaging of the cervical spinal cord of patients with relapsing- magnetic resonance spectroscopy in the entire human cervical
remising multiple sclerosis: a study of 41 cases. Arq Neuropsiquiatr spinal cord and beyond at 3T. Magn Reson Med 2008; 59: 1250–58.
2009; 67: 391–95 98 Moffett JR, Ross B, Arun P, Madhavarao CN, Namboodiri AM.
79 Ciccarelli O, Wheeler-Kingshott CA, McLean MA, et al. Spinal cord N-Acetylaspartate in the CNS: from neurodiagnostics to
spectroscopy and diffusion-based tractography to assess acute neurobiology. Prog Neurobiol 2007; 81: 89–131.
disability in multiple sclerosis. Brain 2007; 130: 2220–31. 99 Ciccarelli O, Thomas DL, De Vita E, et al. Low myo-inositol
80 Freund P, Wheeler-Kingshott C, Jackson J, Miller D, Thompson A, indicating astrocytic damage in a case series of neuromyelitis
Ciccarelli O. Recovery after spinal cord relapse in multiple sclerosis optica. Ann Neurol 2013; 74: 301–05.
is predicted by radial diffusivity. Mult Scler 2010; 16: 1193–202. 100 De Stefano N, Matthews PM, Arnold DL. Reversible decreases in
81 Oh J, Zackowski K, Chen M, et al. Multiparametric MRI correlates N-acetylaspartate after acute brain injury. Magn Reson Med 1995;
of sensorimotor function in the spinal cord in multiple sclerosis. 34: 721–27.
Mult Scler 2013; 19: 427–35. 101 Mader I, Roser W, Kappos L, et al. Serial proton MR spectroscopy of
82 Oh J, Saidha S, Chen M, et al. Spinal cord quantitative MRI contrast-enhancing multiple sclerosis plaques: absolute metabolic
discriminates between disability levels in multiple sclerosis. values over 2 years during a clinical pharmacological study.
Neurology 2013; 80: 540–47. AJNR Am J Neuroradiol 2000; 21: 1220–7.
83 Agosta F, Absinta M, Sormani MP, et al. In vivo assessment of 102 Bates TE, Strangward M, Keelan J, Davey GP, Munro PM, Clark JB.
cervical cord damage in MS patients: a longitudinal diffusion tensor Inhibition of N-acetylaspartate production: implications for
MRI study. Brain 2007; 130: 2211–19. 1H-MRS studies in vivo. Neuroreport 1996; 7: 1397–400.
84 Agosta F, Valsasina P, Caputo D, Stroman PW, Filippi M. Tactile- 103 Lucchinetti CF, Guo Y, Popescu BF, Fujihara K, Itoyama Y, Misu T.
associated recruitment of the cervical cord is altered in patients with The pathology of an autoimmune astrocytopathy: lessons learned
multiple sclerosis. Neuroimage 2008; 39: 1542–48. from neuromyelitis optica. Brain Pathol 2014; 24: 83–97.
85 Agosta F, Valsasina P, Rocca MA, et al. Evidence for enhanced 104 Zhao W, Cohen-Adad J, Polimeni JR, et al. Nineteen-channel receive
functional activity of cervical cord in relapsing multiple sclerosis. array and four-channel transmit array coil for cervical spinal cord
Magn Reson Med 2008; 59: 1035–42. imaging at 7 T. Magn Reson Med 2014; 72: 291–300.
86 Valsasina P, Agosta F, Absinta M, Sala S, Caputo D, Filippi M. 105 Edden RA, Bonekamp D, Smith MA, Dubey P, Barker PB. Proton
Cervical cord functional MRI changes in relapse-onset MS patients. MR spectroscopic imaging of the medulla and cervical spinal cord.
J Neurol Neurosurg Psychiatry 2010; 81: 405–08. J Magn Reson Imaging 2007; 26: 1101–05.
87 Agosta F, Valsasina P, Absinta M, Sala S, Caputo D, Filippi M. 106 Solanky BS, Abdel-Aziz K, Yiannakas MC, Berry AM, Ciccarelli O,
Primary progressive multiple sclerosis: tactile-associated functional Wheeler-Kingshott CA. In vivo magnetic resonance spectroscopy
MR activity in the cervical spinal cord. Radiology 2009; 253: 209–15. detection of combined glutamate-glutamine in healthy upper
88 Valsasina P, Rocca MA, Absinta M, et al. Cervical cord fMRI cervical cord at 3 T. NMR Biomed 2013; 26: 357–66.
abnormalities differ between the progressive forms of multiple 107 Hock A, Wilm B, Zandomeneghi G, et al. Detection of GABA,
sclerosis. Hum Brain Mapp 2012; 33: 2072–80. aspartate and glutathione in the human spinal cord.
89 Rocca MA, Absinta M, Valsasina P, et al. Abnormal cervical cord Joint annual meeting ISMRM, Milan, Italy; May 10–16 Poster
function contributes to fatigue in multiple sclerosis. Mult Scler 2012; number 1712.
18: 1552–59. 108 Ciccarelli O, Toosy AT, De Stefano N, Wheeler-Kingshott CA,
90 Hock A, Henning A, Boesiger P, Kollias SS. 1H-MR spectroscopy in Miller DH, Thompson AJ. Assessing neuronal metabolism in vivo
the human spinal cord. AJNR Am J Neuroradiol 2013; 34: 1682–89. by modeling imaging measures. J Neurosci 2010; 30: 15030–33.
91 Marliani AF, Clementi V, Albini-Riccioli L, Agati R, Leonardi M.
Quantitative proton magnetic resonance spectroscopy of the human
cervical spinal cord at 3 Tesla. Magn Reson Med 2007; 57: 160–63.
454 www.thelancet.com/neurology Vol 14 April 2015
Reproduced with permission of the copyright owner. Further reproduction prohibited without
permission.
You might also like
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Utility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDocument9 pagesUtility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDenis AlexandruNo ratings yet
- Sca IiDocument8 pagesSca IiAlfredo Enrique Marin AliagaNo ratings yet
- cVEMP y oVEMP en ESCLEROSIS MULTIPLEDocument8 pagescVEMP y oVEMP en ESCLEROSIS MULTIPLEJaneth GuzmanNo ratings yet
- bjr-83-493 TirDocument35 pagesbjr-83-493 Tirdoni AfrianNo ratings yet
- Spinal Cord Anatomy and LocalizationDocument18 pagesSpinal Cord Anatomy and LocalizationJuanCarlosRiveraAristizabalNo ratings yet
- Seguridad Social en AlemaniaDocument8 pagesSeguridad Social en AlemaniaMichael RojasNo ratings yet
- Neuroimaging in Investigation of Patients With.11Document20 pagesNeuroimaging in Investigation of Patients With.11mhd.mamdohNo ratings yet
- Spine GAN Semantic Segmentation of MultiDocument40 pagesSpine GAN Semantic Segmentation of MultiDr. Md. Salah Uddin YusufNo ratings yet
- Jpurnal of RadiologyDocument65 pagesJpurnal of RadiologydavinsetiamanahNo ratings yet
- Poljradiol 79 461Document4 pagesPoljradiol 79 461Ale ParraNo ratings yet
- Spec MRI Distinguish Acue TM of NMOSD N Infarction. Kister Et Al 2015Document21 pagesSpec MRI Distinguish Acue TM of NMOSD N Infarction. Kister Et Al 2015Ido BramantyaNo ratings yet
- MielografiaDocument15 pagesMielografiaRafaelNo ratings yet
- WJR 6 716Document11 pagesWJR 6 716laraviNo ratings yet
- Imaging The Spine: Orthopaedics E Ii: Spine and PelvisDocument13 pagesImaging The Spine: Orthopaedics E Ii: Spine and Pelvisraul ramboyongNo ratings yet
- Chapter 2Document11 pagesChapter 2fiskiyeyikimkirdi06No ratings yet
- Epi Zone Articles 1Document8 pagesEpi Zone Articles 1kai xinNo ratings yet
- Samir 2005 OCT in Diagnosis of Neurologic DiseaseDocument11 pagesSamir 2005 OCT in Diagnosis of Neurologic DiseaseAlfredo Enrique Marin AliagaNo ratings yet
- Contents NCLDocument3 pagesContents NCLdewi najiraNo ratings yet
- Newdiagnosiccriteria PDFDocument13 pagesNewdiagnosiccriteria PDFDoaa MokhtarNo ratings yet
- Diagnostics 12 00258 v2Document20 pagesDiagnostics 12 00258 v2Sara GaoNo ratings yet
- Infogrfico5 ArtigoderefernciaDocument21 pagesInfogrfico5 Artigoderefernciagiovannacollins404No ratings yet
- Abnormalities of Cortical Morphology and Structural Covariance Network in Patients With Subacute Basal Ganglia StrokeDocument9 pagesAbnormalities of Cortical Morphology and Structural Covariance Network in Patients With Subacute Basal Ganglia StrokeDiane MxNo ratings yet
- Degeneative Disc DiseaseDocument38 pagesDegeneative Disc Diseaserulitoss_41739No ratings yet
- Wilson 2017Document13 pagesWilson 2017DaniNo ratings yet
- 1891 FullDocument5 pages1891 FullArgtim RexhepiNo ratings yet
- Filippi Assessment Lesions MRI in MSDocument18 pagesFilippi Assessment Lesions MRI in MSAlfonso LemaNo ratings yet
- Tripathy 2015Document19 pagesTripathy 2015Someshwar GuptNo ratings yet
- Krabbe DiseaseDocument6 pagesKrabbe DiseaseUrko GoroquietaNo ratings yet
- Brain SPECT Imaging in Complex Psychiatric Cases: An Evidence-Based, Underutilized ToolDocument9 pagesBrain SPECT Imaging in Complex Psychiatric Cases: An Evidence-Based, Underutilized ToolMariaNo ratings yet
- Neuroimagen en La Esclerosis Lateral Amiotrófica Usos Actuales y EmergentesDocument34 pagesNeuroimagen en La Esclerosis Lateral Amiotrófica Usos Actuales y EmergentesNatalia VelezNo ratings yet
- Chapter 1 by Onwa FavourDocument7 pagesChapter 1 by Onwa Favourdarocha ucheNo ratings yet
- Wardlaw - 2013 Neuroimaging Standards For Research Into Small Vessel Disease SVDDocument17 pagesWardlaw - 2013 Neuroimaging Standards For Research Into Small Vessel Disease SVDDavid JuanNo ratings yet
- NIH Public Access: Author ManuscriptDocument26 pagesNIH Public Access: Author ManuscriptPaul RodrigoNo ratings yet
- Comparison ofDocument10 pagesComparison ofTecnologos 4º turnoNo ratings yet
- Dr. Prudhvinathreddy. A: S/O A.M.Kondareddy 7/350-1A Bhaygya Nagar Colony Kadapa, Ysr Kadapa (DIST) Andhra PradeshDocument13 pagesDr. Prudhvinathreddy. A: S/O A.M.Kondareddy 7/350-1A Bhaygya Nagar Colony Kadapa, Ysr Kadapa (DIST) Andhra PradeshRachnaNo ratings yet
- Ijss Nov Oa28Document5 pagesIjss Nov Oa28Irsanti sasmitaNo ratings yet
- Neuroimaging of Spinal Canal StenosisDocument17 pagesNeuroimaging of Spinal Canal Stenosisrulitoss_41739No ratings yet
- Magnetic Resonance Imaging - 2013 - Ignjatovi - Brain Iron MRI A Biomarker For Amyotrophic Lateral SclerosisDocument8 pagesMagnetic Resonance Imaging - 2013 - Ignjatovi - Brain Iron MRI A Biomarker For Amyotrophic Lateral SclerosisMahima vermaNo ratings yet
- Frohman 2006Document11 pagesFrohman 2006Alfredo Enrique Marin AliagaNo ratings yet
- MRI SeizuresDocument7 pagesMRI SeizuresMarco MalagaNo ratings yet
- Current Clinical Brain Tumor Imaging: Neuroradiology Review SeriesDocument19 pagesCurrent Clinical Brain Tumor Imaging: Neuroradiology Review Seriesalih jenjang2021No ratings yet
- RG 2021200079Document16 pagesRG 2021200079Rahul KashyapNo ratings yet
- Brain Perfusi Dengan Metode Arterial Spin Labeling (Asl) : Prosedur Pemeriksaan Magnetic Resonance Imaging (Mri)Document11 pagesBrain Perfusi Dengan Metode Arterial Spin Labeling (Asl) : Prosedur Pemeriksaan Magnetic Resonance Imaging (Mri)Titi bastiahNo ratings yet
- 5 THDocument17 pages5 THMohamed MohammedNo ratings yet
- Acta 91 84Document2 pagesActa 91 84Mendoza Vázquez MarcoNo ratings yet
- MR Imaging in White Matter Diseases of The Brain and Spinal # GliosisDocument487 pagesMR Imaging in White Matter Diseases of The Brain and Spinal # GliosisRyan Kadavil100% (1)
- Multiple Sclerosis and Related DisordersDocument7 pagesMultiple Sclerosis and Related DisordersScerbatiuc CristinaNo ratings yet
- Clinical Electromyography - The Clinics PDFDocument380 pagesClinical Electromyography - The Clinics PDFSusanaBravoDueñas100% (2)
- Osteoradionecrosis of The Upper Cervical Spine - MR Imaging Following Radiotherapy For Nasopharyngeal CarcinomaDocument7 pagesOsteoradionecrosis of The Upper Cervical Spine - MR Imaging Following Radiotherapy For Nasopharyngeal CarcinomaakreditasiNo ratings yet
- Two Decades of Advances in Muscle Imaging in Children From P - 2021 - NeuromuscDocument13 pagesTwo Decades of Advances in Muscle Imaging in Children From P - 2021 - NeuromuscSuzie Simone Mardones SilvaNo ratings yet
- Uso de Ultrasonografia para Medial EpycondilitisDocument5 pagesUso de Ultrasonografia para Medial EpycondilitisSantiago BianchiNo ratings yet
- Hytec Brain Tolerance Srs MultifractionsDocument19 pagesHytec Brain Tolerance Srs MultifractionsFNo ratings yet
- Optical Coherence Tomography A Window Into The Mechanisms of Multiple SclerosisDocument12 pagesOptical Coherence Tomography A Window Into The Mechanisms of Multiple SclerosisSara BkrNo ratings yet
- European Journal of Radiology: R. Siemund, M. Thurnher, P.C. SundgrenDocument8 pagesEuropean Journal of Radiology: R. Siemund, M. Thurnher, P.C. SundgrenMasithaNo ratings yet
- Endplate DefectsDocument10 pagesEndplate DefectsStancu Oana RuxandraNo ratings yet
- Imaging Techniques For The Lumbar Spine: Conventional Radiology, Computed Tomography Magnetic Resonance ImagingDocument23 pagesImaging Techniques For The Lumbar Spine: Conventional Radiology, Computed Tomography Magnetic Resonance ImagingfilibusterosNo ratings yet
- Metástasis Leptomeningea en Tumores SólidosDocument16 pagesMetástasis Leptomeningea en Tumores SólidosElis EscobarNo ratings yet
- Mri H20Document17 pagesMri H20Khan A RehNo ratings yet
- MRI TB SpineDocument5 pagesMRI TB SpineAyubwarroNo ratings yet
- Fagor CNC 8025 - 8030Document255 pagesFagor CNC 8025 - 8030alvhann_1No ratings yet
- GenesDocument33 pagesGenesJerick RoxasNo ratings yet
- Theory-Set & Relations PDFDocument4 pagesTheory-Set & Relations PDFmp SinghNo ratings yet
- 03 Soil Classification Numerical PDFDocument5 pages03 Soil Classification Numerical PDFabishrantNo ratings yet
- Maxon - Gas Electro-Mechanical ValvesDocument4 pagesMaxon - Gas Electro-Mechanical ValvesThiagoNo ratings yet
- Anritsu Metal Detection GuideDocument32 pagesAnritsu Metal Detection GuideJesus Roberto De La Vega GermanNo ratings yet
- Natural Topography of PakistanDocument25 pagesNatural Topography of Pakistansatayish100% (1)
- HK USP CompactDocument56 pagesHK USP CompactJonathan CrenshawNo ratings yet
- Material Control Procedure - TemplateDocument5 pagesMaterial Control Procedure - TemplateHernandito Rahmat KusumaNo ratings yet
- Drypix 6000 12eDocument501 pagesDrypix 6000 12eraj_meditech100% (1)
- Compound Wall Toilet Revised (4) - ModelDocument1 pageCompound Wall Toilet Revised (4) - ModelInfra SupportNo ratings yet
- 01 Overview of The F & B IndustryDocument8 pages01 Overview of The F & B Industrynikki abalosNo ratings yet
- BS en 6100-3-2 Electromagnetic Compatibility (EMC)Document12 pagesBS en 6100-3-2 Electromagnetic Compatibility (EMC)Arun Jacob CherianNo ratings yet
- 1 s2.0 S0092867422011734 MainDocument29 pages1 s2.0 S0092867422011734 MainIoanna NikdimaNo ratings yet
- A Lightweight True Random Number Generator For Root of Trust ApplicationsDocument11 pagesA Lightweight True Random Number Generator For Root of Trust ApplicationsMADDULURI JAYASRINo ratings yet
- Questions and Answers About Lead in Ceramic Tableware: Contra Costa Health Services / Lead Poisoning Prevention ProjectDocument4 pagesQuestions and Answers About Lead in Ceramic Tableware: Contra Costa Health Services / Lead Poisoning Prevention Projectzorro21072107No ratings yet
- Helminths: NematodesDocument17 pagesHelminths: NematodesNicolle PanchoNo ratings yet
- Zelio Control Relays - RM22TR33Document7 pagesZelio Control Relays - RM22TR33SIVARAMANJAGANATHANNo ratings yet
- Gen Math DianaDocument5 pagesGen Math DianaDon Marlon BuquisNo ratings yet
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- Module Letter 1Document2 pagesModule Letter 1eeroleNo ratings yet
- Psychological Factors Influencing Technology Adoption A Case S - 2021 - TechnovDocument17 pagesPsychological Factors Influencing Technology Adoption A Case S - 2021 - Technov6helmi6nauval6No ratings yet
- 12V-100Ah FTA DatasheetDocument1 page12V-100Ah FTA Datasheetchandrashekar_ganesanNo ratings yet
- Wolfi Landstreicher - Willful Disobedience - Number 3Document32 pagesWolfi Landstreicher - Willful Disobedience - Number 3populaererNo ratings yet
- Multical® 402: Data SheetDocument20 pagesMultical® 402: Data SheetSundar RamasamyNo ratings yet
- MCQ Rewriting 1Document10 pagesMCQ Rewriting 1Quỳnh Anh NguyễnNo ratings yet
- The Heart: Dr. Silvia BoyajianDocument44 pagesThe Heart: Dr. Silvia BoyajianAsem YousefNo ratings yet
- 11 Physical Fitness Assessment 1Document40 pages11 Physical Fitness Assessment 1Danilo Sare IIINo ratings yet
- Chapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Document9 pagesChapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Adeyoju RebeccaNo ratings yet
- Seismic Retrofitting2.0 BY PRIYANSHUDocument30 pagesSeismic Retrofitting2.0 BY PRIYANSHUPriyanshu VarshneyNo ratings yet