You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- First Day of School Pics 2020-21Document18 pagesFirst Day of School Pics 2020-21Evangelin MelvinNo ratings yet
- Printable Indoor Scavenger Hunts For KidsDocument5 pagesPrintable Indoor Scavenger Hunts For KidsEvangelin MelvinNo ratings yet
- Printable Family Quarantine Bucket ListDocument2 pagesPrintable Family Quarantine Bucket ListEvangelin MelvinNo ratings yet
- See-Trace-Write Christmas Preschool Writing PackDocument22 pagesSee-Trace-Write Christmas Preschool Writing PackEvangelin MelvinNo ratings yet
- Simple Preschool RoutineDocument10 pagesSimple Preschool RoutineEvangelin MelvinNo ratings yet
- Rest in Christ: Memory Verse - Hand Out Scriptures To ReadDocument2 pagesRest in Christ: Memory Verse - Hand Out Scriptures To ReadEvangelin MelvinNo ratings yet
- Rest in Christ: Memory Verse - Hand Out Scriptures To ReadDocument2 pagesRest in Christ: Memory Verse - Hand Out Scriptures To ReadEvangelin MelvinNo ratings yet
- Home Care Assessment EditedDocument3 pagesHome Care Assessment EditedEvangelin Melvin100% (1)
- Crops in Tamil - Google SearchDocument1 pageCrops in Tamil - Google SearchEvangelin MelvinNo ratings yet
- Parenting Is Hard, Especially Trying To Be Patient... Scattered QuotesDocument1 pageParenting Is Hard, Especially Trying To Be Patient... Scattered QuotesEvangelin MelvinNo ratings yet
- Parenting Is Hard, Especially Trying To Be Patient... Scattered QuotesDocument1 pageParenting Is Hard, Especially Trying To Be Patient... Scattered QuotesEvangelin MelvinNo ratings yet
- StewardshipDocument74 pagesStewardshipEvangelin MelvinNo ratings yet
- Crops in Tamil - Google SearchDocument1 pageCrops in Tamil - Google SearchEvangelin MelvinNo ratings yet
- 8 Wound Care ANTT Assessment - Form 6Document1 page8 Wound Care ANTT Assessment - Form 6Evangelin MelvinNo ratings yet
- IPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyDocument27 pagesIPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyEvangelin MelvinNo ratings yet
- Management of Patients With Musculoskeletal Trauma and ProblemsDocument122 pagesManagement of Patients With Musculoskeletal Trauma and ProblemsEvangelin MelvinNo ratings yet
- IPC15AsepticNonTouchTechnique (ANTT) May13Document11 pagesIPC15AsepticNonTouchTechnique (ANTT) May13Evangelin MelvinNo ratings yet
- Topics02 01Document326 pagesTopics02 01Evangelin MelvinNo ratings yet
- Aseptic Non Touch Techniques Policy V4nov 2018Document21 pagesAseptic Non Touch Techniques Policy V4nov 2018Evangelin MelvinNo ratings yet
- 4ps Self Assessment Tool IndividualDocument9 pages4ps Self Assessment Tool IndividualMuhammad Faraz HasanNo ratings yet
- IPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyDocument27 pagesIPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyEvangelin MelvinNo ratings yet
- Agonda BeachDocument1 pageAgonda BeachEvangelin MelvinNo ratings yet
- YouthCentral Resume VCE WorkExpDocument6 pagesYouthCentral Resume VCE WorkExpRick MercadoNo ratings yet
- Musculoskeletalnursing 171106105453Document122 pagesMusculoskeletalnursing 171106105453Evangelin MelvinNo ratings yet
- Musculoskeletalnursing 171106105453Document122 pagesMusculoskeletalnursing 171106105453Evangelin MelvinNo ratings yet
- Nursing CareDocument8 pagesNursing CareEvangelin MelvinNo ratings yet
- Early Warning Score (EWS) Procedure 239155Document16 pagesEarly Warning Score (EWS) Procedure 239155Evangelin MelvinNo ratings yet
- Early Warning Score (EWS) Procedure 239155Document16 pagesEarly Warning Score (EWS) Procedure 239155Evangelin MelvinNo ratings yet
- Arterial Blood Gas SamplingDocument56 pagesArterial Blood Gas SamplingThai CheNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Peace Through Literature: A Thematic Study of Ernest Hemingway's A Farewell To ArmsDocument4 pagesPeace Through Literature: A Thematic Study of Ernest Hemingway's A Farewell To ArmsEnglish JournalNo ratings yet
- Name: Noor-Ul-Dhuha Assignment: First Registration: Sp19-Baf-018 Date: 20-04-2020 Subject: MarketingDocument9 pagesName: Noor-Ul-Dhuha Assignment: First Registration: Sp19-Baf-018 Date: 20-04-2020 Subject: MarketingTiny HumanNo ratings yet
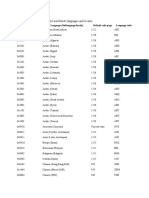
- The Following Table Shows The Worldwide Languages and LocalesDocument12 pagesThe Following Table Shows The Worldwide Languages and LocalesOscar Mauricio Vargas UribeNo ratings yet
- Applied English Phonology 3rd EditionDocument1 pageApplied English Phonology 3rd Editionapi-2413357310% (7)
- Figures of Speech: Figure of Speech-Word or Phrase That Makes A Comparison BetweenDocument2 pagesFigures of Speech: Figure of Speech-Word or Phrase That Makes A Comparison BetweenPRAMODRAUT85No ratings yet
- Pruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Document2 pagesPruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Jeru SierraNo ratings yet
- Phonetastic PhrasesDocument6 pagesPhonetastic PhrasesAlma NazarioNo ratings yet
- English Vocabulary Exercises LIFE STAGES 2022Document3 pagesEnglish Vocabulary Exercises LIFE STAGES 2022daniela BroccardoNo ratings yet
- Sinhala AlphabetDocument7 pagesSinhala AlphabetSivapalasundaram Raghuram0% (1)
- The Analects of Confucius SummaryDocument3 pagesThe Analects of Confucius SummaryJoshua Paul Ersando100% (1)
- Alina Anasie-BUSINESS ENVIRONMENTDocument14 pagesAlina Anasie-BUSINESS ENVIRONMENTalina mateiNo ratings yet
- Jurisprudential Analysis of Nirbhaya Rape CaseDocument25 pagesJurisprudential Analysis of Nirbhaya Rape CaseAishwarya Ravikhumar67% (3)
- Old Torrance Unified Report CardDocument2 pagesOld Torrance Unified Report CardSouthern California Public RadioNo ratings yet
- Chaoter 1 AssignmentDocument44 pagesChaoter 1 AssignmentBatool AbbasNo ratings yet
- Rizal As A TeacherDocument12 pagesRizal As A TeacherKristine AgustinNo ratings yet
- Commendation For Excellence in Support of The Student ExperienceDocument2 pagesCommendation For Excellence in Support of The Student ExperienceRayna Dianne DosanoNo ratings yet
- (2014) Designing Hypermuscular Neoaristocracy - Tereza KuldovaDocument8 pages(2014) Designing Hypermuscular Neoaristocracy - Tereza KuldovaTereza KuldovaNo ratings yet
- Grade 11 Arts and Design Prospectus Version 2Document1 pageGrade 11 Arts and Design Prospectus Version 2kaiaceegees0% (1)
- International Relations VocabularyDocument1 pageInternational Relations Vocabularyjeanneidys GNo ratings yet
- The Malta & Gozo History & Culture Brochure 2010Document16 pagesThe Malta & Gozo History & Culture Brochure 2010VisitMalta67% (3)
- Sid ResumeDocument2 pagesSid ResumeBikash Ranjan SahuNo ratings yet
- 9 Ahmad Rasul Ashap SalehDocument8 pages9 Ahmad Rasul Ashap SalehRionaldiNo ratings yet
- Stephen Krashen's Theory of Second Language Acquisition (Assimilação Natural - o Construtivismo No Ensino de Línguas)Document5 pagesStephen Krashen's Theory of Second Language Acquisition (Assimilação Natural - o Construtivismo No Ensino de Línguas)Danilo de OliveiraNo ratings yet
- Asian Contemporary Art in JapanDocument7 pagesAsian Contemporary Art in Japanvekjeet ChampNo ratings yet
- Uni Registration Form PDFDocument3 pagesUni Registration Form PDFNueron TreeNo ratings yet
- How I Became A PirateDocument3 pagesHow I Became A PirateJalina McClainNo ratings yet
- Lacan and His Influence: Kevin JonesDocument2 pagesLacan and His Influence: Kevin JonesannaNo ratings yet
- Resume SampleDocument3 pagesResume SampleAlibasher H. Azis EsmailNo ratings yet
- CV Kashif AliDocument2 pagesCV Kashif AliRao KashifNo ratings yet
- Understanding and Writing Pourquoi StoriesDocument5 pagesUnderstanding and Writing Pourquoi StoriesDiannaGregoryNarotskiNo ratings yet