You might also like
- MindTap - Cengage LearningDocument11 pagesMindTap - Cengage Learningkate jNo ratings yet
- Hospitals in Ilocos SurDocument3 pagesHospitals in Ilocos SurMatt Joseph Cabanting100% (4)
- DR V Krishna Murthy HintsDocument31 pagesDR V Krishna Murthy HintsDrmengani Vamsi Krishna Reddy100% (2)
- Golden - Plaza: Evolution of Health and FitnessDocument11 pagesGolden - Plaza: Evolution of Health and FitnessGodzilla555100% (1)
- Hospital Annual Work Plan Format FinalDocument28 pagesHospital Annual Work Plan Format FinalSila Ontita100% (9)
- Black Book Project 3Document69 pagesBlack Book Project 3Pragya SinghNo ratings yet
- Germanium, A New Approach To Immunity - Betty Kamen, Ph.d.Document25 pagesGermanium, A New Approach To Immunity - Betty Kamen, Ph.d.wxcvbnnbvcxwNo ratings yet
- Multiple Disability Original HandoutDocument42 pagesMultiple Disability Original HandoutHabtamu DebasuNo ratings yet
- Bipolar DisorderDocument8 pagesBipolar DisorderInternational Business Times100% (4)
- Community PsychologyDocument20 pagesCommunity PsychologyMaePornelaGomezNo ratings yet
- Form Pain DetectDocument2 pagesForm Pain Detectalvin100% (4)
- Glutamina 1Document9 pagesGlutamina 1FabianaNo ratings yet
- Cost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationDocument10 pagesCost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationUday PrabhuNo ratings yet
- JurdingDocument9 pagesJurdingsiti hazard aldinaNo ratings yet
- Primary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyDocument7 pagesPrimary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyLuvita Amallia SyadhatinNo ratings yet
- HFNC Vs CpapDocument11 pagesHFNC Vs CpapsilNo ratings yet
- Comparison of Outcomes and Cost-Effectiveness of Laparoscopic and Open Appendectomies in Public Health ServicesDocument12 pagesComparison of Outcomes and Cost-Effectiveness of Laparoscopic and Open Appendectomies in Public Health Servicesviviana benavidesNo ratings yet
- Elliott2017 Article CostEffectivenessOfSupportForP 220711 174907Document19 pagesElliott2017 Article CostEffectivenessOfSupportForP 220711 174907Claudia Andreea StroiaNo ratings yet
- Quality and Safety in AnaesthesiaDocument10 pagesQuality and Safety in Anaesthesiaanna67890No ratings yet
- Pet CT en OncologiaDocument17 pagesPet CT en OncologiaJulissa GamboaNo ratings yet
- Outcome Reporting in Randomized Controlled Trials and Systematic Reviews of Gastroschisis Treatment A Systematic ReviewDocument5 pagesOutcome Reporting in Randomized Controlled Trials and Systematic Reviews of Gastroschisis Treatment A Systematic ReviewEngga CandranataNo ratings yet
- Clinical Nutrition: Narrative ReviewDocument12 pagesClinical Nutrition: Narrative Reviewelivi788No ratings yet
- E039314 FullDocument8 pagesE039314 FullMukesh kumarNo ratings yet
- Introduction To The Postanaesthetic Care Unit: Review Open AccessDocument7 pagesIntroduction To The Postanaesthetic Care Unit: Review Open AccessSamsul BahriNo ratings yet
- Fphar 11 572569Document12 pagesFphar 11 572569hainguyen.htalabNo ratings yet
- Clarithromycin and Endoscopic SinusDocument18 pagesClarithromycin and Endoscopic SinusgekwahyuNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- 2016 Article 109Document7 pages2016 Article 109Nurul SholehahNo ratings yet
- Pmed 1003228Document22 pagesPmed 1003228Ioanna Bianca HNo ratings yet
- Prediction of Future Gastric Cancer Risk Using A Machine Learning Algorithm and Comprehensive Medical Check-Up Data: A Case-Control StudyDocument9 pagesPrediction of Future Gastric Cancer Risk Using A Machine Learning Algorithm and Comprehensive Medical Check-Up Data: A Case-Control StudyAriani ArinNo ratings yet
- PRO10 THE COST ANALYSIS OF EMICIZUMAB VERSUS ACTIVATED PROTHROMB - 2020 - ValueDocument1 pagePRO10 THE COST ANALYSIS OF EMICIZUMAB VERSUS ACTIVATED PROTHROMB - 2020 - ValueMichael John AguilarNo ratings yet
- Cost-Utility Analysis of A Pharmacy-Led Self-Management Programme For Patients With COPDDocument10 pagesCost-Utility Analysis of A Pharmacy-Led Self-Management Programme For Patients With COPDoktarina puspitasariNo ratings yet
- Tight Glycemic Control in Critically Ill PediatricDocument11 pagesTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNo ratings yet
- ArticleDocument6 pagesArticlecarlostororeumatologoNo ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- Ab StewardshipDocument10 pagesAb StewardshipAdkhiatul MuslihatinNo ratings yet
- The Limitations of Observation StudiesDocument5 pagesThe Limitations of Observation StudiesalbgomezNo ratings yet
- Helpa PicoDocument14 pagesHelpa Picoannisa sriwahyuNo ratings yet
- Clinical Science Session-IsTCDocument17 pagesClinical Science Session-IsTCSari HarahapNo ratings yet
- NG9FullGuidanceAppendicesA-J 20150601 PDFDocument713 pagesNG9FullGuidanceAppendicesA-J 20150601 PDFJosué Espino RomeroNo ratings yet
- Health Related Quality of Life Following Open VersDocument8 pagesHealth Related Quality of Life Following Open Versevelynmoreirappgcmh.ufpaNo ratings yet
- Clinical Practice Guidelines For Hepatocellular Carcinoma TheJapan Society of Hepatology 2017 (4th JSH-HCC Guidelines) 2019 UpdateDocument5 pagesClinical Practice Guidelines For Hepatocellular Carcinoma TheJapan Society of Hepatology 2017 (4th JSH-HCC Guidelines) 2019 UpdateTri PutraNo ratings yet
- 7 ArticuloDocument11 pages7 ArticuloKarina AngelNo ratings yet
- Strokeaha 109 576413Document13 pagesStrokeaha 109 576413ichaNo ratings yet
- Diagnostic Efficacy of Cone Beam Computed Tomography in Paediatric Dentistry: A Systematic ReviewDocument20 pagesDiagnostic Efficacy of Cone Beam Computed Tomography in Paediatric Dentistry: A Systematic ReviewJoe TorresNo ratings yet
- Behrendt 2016Document11 pagesBehrendt 2016David MolinaNo ratings yet
- HPV Testing Compared With Routine Cytology in Cervical Screening Long-Term Follow-Up of ARTISTIC RCTDocument66 pagesHPV Testing Compared With Routine Cytology in Cervical Screening Long-Term Follow-Up of ARTISTIC RCTJosé HidalgoNo ratings yet
- A Strategy To Reduce The Carbon Footprint of Clinical TrialsDocument2 pagesA Strategy To Reduce The Carbon Footprint of Clinical TrialsAnastasija LevcenkoNo ratings yet
- E023721 FullDocument9 pagesE023721 Fulljimmy xanzNo ratings yet
- Cost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanDocument9 pagesCost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanRizki MartaNo ratings yet
- CostDocument13 pagesCostClaudia Andreea StroiaNo ratings yet
- 11Document8 pages11mrpaul giovaniNo ratings yet
- COPD RehabilitationDocument12 pagesCOPD RehabilitationharbiNo ratings yet
- Estimating The Cost-Effectiveness of Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes in EnglandDocument13 pagesEstimating The Cost-Effectiveness of Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes in EnglandlivtbuenoNo ratings yet
- 1471 2334 12 83Document10 pages1471 2334 12 83yatedigo958No ratings yet
- Analisis Minimalisasi Biaya (CMA)Document7 pagesAnalisis Minimalisasi Biaya (CMA)diahsaharaNo ratings yet
- Procalcitonin and AB DecisionsDocument10 pagesProcalcitonin and AB DecisionsDennysson CorreiaNo ratings yet
- s13741 021 00214 3Document12 pagess13741 021 00214 3Carlos Daniel Rangel MartinezNo ratings yet
- Internet Interventions: SciencedirectDocument12 pagesInternet Interventions: SciencedirectMuthya GhitaNo ratings yet
- Guia JapomesaDocument11 pagesGuia JapomesaKarem Andrea CamachoNo ratings yet
- Acute Chemotherapy-Induced Nausea and Vomiting in Children With Cancer Still Waiting For A Common Consensus On Treatment PDFDocument8 pagesAcute Chemotherapy-Induced Nausea and Vomiting in Children With Cancer Still Waiting For A Common Consensus On Treatment PDFPaola DiazNo ratings yet
- Routine Chest Physiotherapy For Pneumonia in AdultsDocument3 pagesRoutine Chest Physiotherapy For Pneumonia in AdultsJetindar PuriNo ratings yet
- Andrianasolo2019 PDFDocument22 pagesAndrianasolo2019 PDFkamila rodriguezNo ratings yet
- Clinical Oncology: EditorialDocument3 pagesClinical Oncology: EditorialSyed HossainNo ratings yet
- UntitledDocument15 pagesUntitledMARTIN DANIEL COLMENAREZ RODRIGUEZNo ratings yet
- BR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialDocument7 pagesBR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialMarcellia AngelinaNo ratings yet
- A New Treatment Method of Advanced Metastic TumorsDocument7 pagesA New Treatment Method of Advanced Metastic TumorsDiana DíazNo ratings yet
- Jay Raja: Mr. Ashish KyadaDocument36 pagesJay Raja: Mr. Ashish Kyadajvraja80100% (2)
- Analysis of Deprescription Strategies of Proton Pump Inhibitors in Primary CareDocument7 pagesAnalysis of Deprescription Strategies of Proton Pump Inhibitors in Primary CareVíctor Pérez RiveroNo ratings yet
- Economic Evaluation Strategies in Telehealth: Obtaining A More Holistic Valuation of Telehealth InterventionsDocument5 pagesEconomic Evaluation Strategies in Telehealth: Obtaining A More Holistic Valuation of Telehealth InterventionsAlejandro CardonaNo ratings yet
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondFrom EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattNo ratings yet
- Reinforcing Kangaroo Mother Care Uptake in Resource Limited SettingsDocument5 pagesReinforcing Kangaroo Mother Care Uptake in Resource Limited SettingsNadia AyuningtiasNo ratings yet
- Diagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentDocument3 pagesDiagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentNadia AyuningtiasNo ratings yet
- Jurnal 11980Document12 pagesJurnal 11980hafid wabulaNo ratings yet
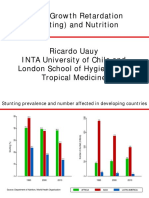
- Uauy PDFDocument52 pagesUauy PDFNadia AyuningtiasNo ratings yet
- Efek Zinc Pada Anak Dengan Gagal TumbuhDocument5 pagesEfek Zinc Pada Anak Dengan Gagal TumbuhirfhanahusaNo ratings yet
- Chapter 1Document6 pagesChapter 1Nadia AyuningtiasNo ratings yet
- Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateDocument6 pagesEstimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateNadia AyuningtiasNo ratings yet
- Brigada ZumbaDocument2 pagesBrigada ZumbaRommel DaysonNo ratings yet
- Household 1Document2 pagesHousehold 1ainun rapikaNo ratings yet
- BSC English Notes NewDocument54 pagesBSC English Notes NewFahad HabibNo ratings yet
- 6 Best Homeopathic Medicines For Swollen Ankles - Homeopathy at DrHomeoDocument9 pages6 Best Homeopathic Medicines For Swollen Ankles - Homeopathy at DrHomeovivek khannaNo ratings yet
- Evaluation For PediaDocument4 pagesEvaluation For PediaEva BellaNo ratings yet
- Nursing and Midwifery Board - Questionnaire - Re Entry To Practice Self Assessment Questionnaire - Enrolled NurseDocument10 pagesNursing and Midwifery Board - Questionnaire - Re Entry To Practice Self Assessment Questionnaire - Enrolled NurseZafarsodikNo ratings yet
- Final Research Paper Group 4Document64 pagesFinal Research Paper Group 4Airey Alasan EconarNo ratings yet
- After ProhibitionDocument16 pagesAfter ProhibitionChris JosephNo ratings yet
- Symptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportDocument14 pagesSymptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportThaísa NogueiraNo ratings yet
- The Health Insurance WorkbookDocument12 pagesThe Health Insurance WorkbookLarry ThomasNo ratings yet
- Lecture 1Document38 pagesLecture 1Yong Hao Jordan JinNo ratings yet
- 375 Vitolize Womens ENG Rev1-9-13 PDFDocument1 page375 Vitolize Womens ENG Rev1-9-13 PDFMaria Angela OtelNo ratings yet
- Bachelor of Science Degree in Food - Nutrition and Dietetics PDFDocument42 pagesBachelor of Science Degree in Food - Nutrition and Dietetics PDFDon Baraka DanielNo ratings yet
- Report of Mr. AUDARYA MANEDocument1 pageReport of Mr. AUDARYA MANENeutral GodNo ratings yet
- Dialog 2 WWDocument4 pagesDialog 2 WWILHAM FERDIANSAHNo ratings yet
- Validation of Attention Deficit Hyperactivity DisoDocument5 pagesValidation of Attention Deficit Hyperactivity DisoNarmada DevkotaNo ratings yet
- What Is Medical DeontologyDocument11 pagesWhat Is Medical DeontologyExorticNo ratings yet
- Drug Study and LaboratoryDocument13 pagesDrug Study and LaboratoryGEOMHAI CATBAGANNo ratings yet
- Daftar Pustaka: Komang Trisna AriestiniDocument7 pagesDaftar Pustaka: Komang Trisna AriestiniRamayanaNo ratings yet