You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Abram Hoffer - Prousky - Niacinamide's Potent Role in Alleviating Anxiety With Its Benzodiazepine-Like Properties - TextDocument8 pagesAbram Hoffer - Prousky - Niacinamide's Potent Role in Alleviating Anxiety With Its Benzodiazepine-Like Properties - TextEbook PDF100% (1)
- How To Live With Schizophrenia - Hoffer, Abram, 1917Document200 pagesHow To Live With Schizophrenia - Hoffer, Abram, 1917Ebook PDF100% (1)
- Beyond Antibiotics - Michael A. Schmidt (Orthomolecular Medicine)Document364 pagesBeyond Antibiotics - Michael A. Schmidt (Orthomolecular Medicine)Ebook PDF100% (5)
- Cancer and Vitamin C - Cameron, Ewan and Linus Pauling PDF EbookDocument262 pagesCancer and Vitamin C - Cameron, Ewan and Linus Pauling PDF EbookEbook PDF100% (2)
- Smart Nutrients - Abram Hoffer PDF (Orthomolecular Medicine)Document228 pagesSmart Nutrients - Abram Hoffer PDF (Orthomolecular Medicine)Anonymous gwFqQcnaX100% (4)
- (Abram Hoffer) Hoffer Laws of Natural NutritionDocument144 pages(Abram Hoffer) Hoffer Laws of Natural NutritionEbook PDFNo ratings yet
- 23mb (Abram Hoffer, Andrew W. Saul) Orthomolecular Medicine For EveryoneDocument663 pages23mb (Abram Hoffer, Andrew W. Saul) Orthomolecular Medicine For EveryoneEbook PDF92% (12)
- Ebook Parsons Cholesterol Control Without Diet by William Parsons (Orthomolecular Medicine)Document256 pagesEbook Parsons Cholesterol Control Without Diet by William Parsons (Orthomolecular Medicine)Ebook PDF100% (5)
- VItamin B3 Therapy Niacin BillW Bill Wilson Alcoholics Anonymous AA Abram HofferDocument93 pagesVItamin B3 Therapy Niacin BillW Bill Wilson Alcoholics Anonymous AA Abram HofferEbook PDFNo ratings yet
- AbramHoffer Orthomolecular Psychiatry What Would Abram Hoffer Do 29.2Document13 pagesAbramHoffer Orthomolecular Psychiatry What Would Abram Hoffer Do 29.2Ebook PDF100% (1)
- The Calcium Factor - The Scientific Secret - Robert BarefootDocument225 pagesThe Calcium Factor - The Scientific Secret - Robert BarefootEbook PDF100% (5)
- The Disease Conspiracy - The FDA Suppression of Cures - Robert BarefootDocument227 pagesThe Disease Conspiracy - The FDA Suppression of Cures - Robert BarefootEbook PDF100% (5)
- Eydie Maes Natural Recipes With Ocr Text (Orthomolecular Medicine)Document170 pagesEydie Maes Natural Recipes With Ocr Text (Orthomolecular Medicine)Ebook PDF100% (1)
- Eydie Mae How I Conquered Cancer With Ocr Text (Orthomolecular Medicine)Document227 pagesEydie Mae How I Conquered Cancer With Ocr Text (Orthomolecular Medicine)Ebook PDF100% (1)
- Anthony Demello and OshoDocument4 pagesAnthony Demello and OshoEbook PDF100% (4)
- Ebook Vitamin C and The Common Cold - Linus - PaulingDocument132 pagesEbook Vitamin C and The Common Cold - Linus - PaulingEbook PDF92% (12)
- Ebook: How To Live Longer and Feel Better - Linus Pauling Ebook PDF BookDocument436 pagesEbook: How To Live Longer and Feel Better - Linus Pauling Ebook PDF BookEbook PDF100% (40)
- A New Earth Webinar TranscriptsDocument500 pagesA New Earth Webinar Transcriptslexen100% (1)
- Article - Best Small Towns Picturesque Towns in Europe - Your Favorite - Europe Forum - Fodor's Travel Talk ForumsDocument21 pagesArticle - Best Small Towns Picturesque Towns in Europe - Your Favorite - Europe Forum - Fodor's Travel Talk ForumsEbook PDFNo ratings yet
- Heart Disease, Ascorbate, Lysine and Linus Pauling by Jeffrey Dach MDDocument33 pagesHeart Disease, Ascorbate, Lysine and Linus Pauling by Jeffrey Dach MDEbook PDF100% (1)
- Matthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentDocument40 pagesMatthias Rath Cancer Book - Vitamin C and Lysine For Cancer TreatmentEbook PDF100% (3)
- Linus Pauling - My Love Affair Vitamin CDocument11 pagesLinus Pauling - My Love Affair Vitamin CEbook PDF100% (1)
- A New Earth Webinar TranscriptsDocument500 pagesA New Earth Webinar Transcriptslexen100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DRNB Medical Gastroenterology Paper1Document4 pagesDRNB Medical Gastroenterology Paper1Srinivas PingaliNo ratings yet
- Pathogenic Microorganisms BrochureDocument2 pagesPathogenic Microorganisms Brochureapi-316071223No ratings yet
- A Clinal Primer On Intellectual DisabilityDocument13 pagesA Clinal Primer On Intellectual DisabilityAra AzzahraNo ratings yet
- Childhood ObesityDocument30 pagesChildhood ObesityLeetal KarkayNo ratings yet
- 11 - Precautions For Handling Organic SolventDocument2 pages11 - Precautions For Handling Organic SolventMummy TheNo ratings yet
- Parasitology International: ReviewDocument7 pagesParasitology International: ReviewAhmad PradhanaNo ratings yet
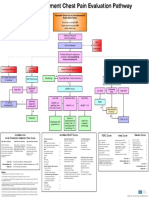
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Utah Medical Cannabis Act OverviewDocument10 pagesUtah Medical Cannabis Act OverviewThe Salt Lake Tribune100% (1)
- Sexually Transmitted DiseasesDocument9 pagesSexually Transmitted DiseasesRodrigo Paolo Marquina EscuadraNo ratings yet
- 4 Stool Culture PDFDocument35 pages4 Stool Culture PDFVenny PatriciaNo ratings yet
- Anxiety DisordersDocument9 pagesAnxiety DisordersGEETA MOHANNo ratings yet
- Adime For DiabetesDocument2 pagesAdime For Diabetesapi-383891195No ratings yet
- Geria ReviewerDocument2 pagesGeria ReviewerbillyktoubattsNo ratings yet
- Graft Versus Host Disease..Document2 pagesGraft Versus Host Disease..Sakawath HosainNo ratings yet
- Drugs For Heart FailureDocument39 pagesDrugs For Heart FailureOngKahYeeNo ratings yet
- Similarities and Differences VocabularyDocument9 pagesSimilarities and Differences VocabularyAliNo ratings yet
- CHRONIC HEPATITIS Prof DR Tarek ShetaDocument38 pagesCHRONIC HEPATITIS Prof DR Tarek ShetaSheren GamaleldenNo ratings yet
- Personality and Social DevelopmentDocument15 pagesPersonality and Social DevelopmentKri de AsisNo ratings yet
- HypertensionDocument1 pageHypertensionshailesh284No ratings yet
- DRUG STUDY Bronchitis CorsigaDocument8 pagesDRUG STUDY Bronchitis CorsigaKasandra Dawn Moquia BerisoNo ratings yet
- C1 Ob-Gyn-2020Document33 pagesC1 Ob-Gyn-2020yabsera mulatuNo ratings yet
- Stress ManagementDocument5 pagesStress Managementapi-314189740No ratings yet
- Family Case Study: BLK 4. Room 7, Phase 5 Brgy. Dela PazDocument9 pagesFamily Case Study: BLK 4. Room 7, Phase 5 Brgy. Dela PazShamz SitiarNo ratings yet
- Common Prescribed DrugsDocument33 pagesCommon Prescribed DrugsGlessica You50% (4)
- A Beautiful Mind ReviewDocument9 pagesA Beautiful Mind ReviewPatriciaChristieNo ratings yet
- Hepatitis BDocument61 pagesHepatitis BMichael AmandyNo ratings yet
- Organic DiseasesDocument3 pagesOrganic DiseasesGlenn Cabance LelinaNo ratings yet
- 35% H2O2 Hydrogen Peroxide Food GradeDocument5 pages35% H2O2 Hydrogen Peroxide Food GradefreeNo ratings yet
- Cerebral Palsy An Overview 2018Document11 pagesCerebral Palsy An Overview 2018Yhuliana AcostaNo ratings yet
- Goddess Isis - 7D InitiationDocument6 pagesGoddess Isis - 7D InitiationEmeraldRayNo ratings yet