You might also like
- Revised Concept Care Map RachelDocument1 pageRevised Concept Care Map Rachelapi-726698459No ratings yet
- Scribe America Final, Emergency DepartmentDocument41 pagesScribe America Final, Emergency DepartmentJulio CastilloNo ratings yet
- Maternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Document2 pagesMaternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Yash atriNo ratings yet
- Pulmonary EmbolismDocument27 pagesPulmonary EmbolismErick Rangga JuniorNo ratings yet
- Pulmonary Embolism - International Emergency Medicine Education ProjectDocument24 pagesPulmonary Embolism - International Emergency Medicine Education ProjectקרוליינהסתםחולםNo ratings yet
- Step Down RN or Progressive Care Skills ChecklistDocument4 pagesStep Down RN or Progressive Care Skills Checklisthealth careNo ratings yet
- Patho 2020Document2 pagesPatho 2020Aziil LiizaNo ratings yet
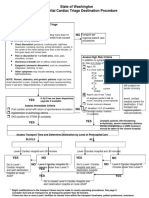
- State of Washington Prehospital Cardiac Triage Destination ProcedureDocument4 pagesState of Washington Prehospital Cardiac Triage Destination ProcedureNanda Dwi Bintoro ZiehenShopNo ratings yet
- Cyanotic Congenital Heart Defects:: Practical Approach For PediatricianDocument25 pagesCyanotic Congenital Heart Defects:: Practical Approach For PediatricianYogiPrimaZulkifliNo ratings yet
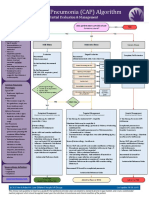
- Pneumonia (CAP) Algorithm: Initial Evaluation & ManagementDocument2 pagesPneumonia (CAP) Algorithm: Initial Evaluation & ManagementAbdi Dwiyanto PutraNo ratings yet
- Primary Care FollowupDocument1 pagePrimary Care Followupe-MedTools100% (6)
- Intrapartum Monitoring: Causes of Fetal Compromise During LaborDocument10 pagesIntrapartum Monitoring: Causes of Fetal Compromise During LaborlicencaNo ratings yet
- IM ReviewDocument4 pagesIM ReviewPäw YusophNo ratings yet
- IM Review 2Document245 pagesIM Review 2Rosela TorralbaNo ratings yet
- Full TextDocument55 pagesFull TextDiyah Ayu Nur SantiNo ratings yet
- Chest Pain Investigation Diagnosis and TreatmentDocument4 pagesChest Pain Investigation Diagnosis and TreatmentHadsabsaNo ratings yet
- OB - Cardiovascular Disorders (LRA)Document6 pagesOB - Cardiovascular Disorders (LRA)Anonymous ANo ratings yet
- Chest Pain - Investigation, Diagnosis and TreatmentDocument5 pagesChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- Taco and Trali: Savita HandayaniDocument12 pagesTaco and Trali: Savita HandayaniAnna Puteri GozaliNo ratings yet
- Qdoc - Tips Nilai Kritis Ekg Dan RadiologiDocument3 pagesQdoc - Tips Nilai Kritis Ekg Dan RadiologiTulus ArisonoNo ratings yet
- Surgery FADocument170 pagesSurgery FArafeekwalid551No ratings yet
- Referral Cheat Sheet: Before You CallDocument2 pagesReferral Cheat Sheet: Before You CallXyz100% (2)
- Case Presentation On CHFDocument13 pagesCase Presentation On CHFCalingalan Hussin CaluangNo ratings yet
- Aflp, Ka, RV, byDocument22 pagesAflp, Ka, RV, byNatasha AnditaNo ratings yet
- ACSDocument56 pagesACSGabriel CalderónNo ratings yet
- Critical Congenital Heart DiseaseDocument55 pagesCritical Congenital Heart DiseaseAntonius SimangunsongNo ratings yet
- AECP - Chest PainDocument7 pagesAECP - Chest PainBenny TrisaktyariNo ratings yet
- Boala Coronariana Cronica Stabila: 16 October 2019 18:27Document131 pagesBoala Coronariana Cronica Stabila: 16 October 2019 18:27Mady MaduNo ratings yet
- PBL - CardioDocument5 pagesPBL - Cardiogie sarcedaNo ratings yet
- Pulmonary Edema Concept MapDocument3 pagesPulmonary Edema Concept MapGeraldine MagnanaoNo ratings yet
- Frequently Used Medical AbbreviationsDocument10 pagesFrequently Used Medical AbbreviationsdunareagalatiNo ratings yet
- Em Basic Chest Pain Show NotesDocument2 pagesEm Basic Chest Pain Show NoteshabbouraNo ratings yet
- Management of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineDocument7 pagesManagement of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineSahera Nurhidayah NasutionNo ratings yet
- Diagnostic Tree: DyspneaDocument2 pagesDiagnostic Tree: DyspneaDiana CarolinaNo ratings yet
- F3B Concept Map March 10Document1 pageF3B Concept Map March 10Dinah Rose VitorilloNo ratings yet
- GoitreDocument2 pagesGoitresuggaplumNo ratings yet
- TTS Guidelines R5 2Document5 pagesTTS Guidelines R5 2mikeNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- Acute Care Toolkit 15 Flowcharts Nov19 0Document7 pagesAcute Care Toolkit 15 Flowcharts Nov19 0Ash AmeNo ratings yet
- (Ayuda) Surg2 Le1 RecallsDocument11 pages(Ayuda) Surg2 Le1 RecallsFrances DeiNo ratings yet
- Peripartum Management of Hypertension: A Position Paper of The ESC Council On Hypertension and The European Society of HypertensionDocument10 pagesPeripartum Management of Hypertension: A Position Paper of The ESC Council On Hypertension and The European Society of HypertensionRafael Molina QuirozNo ratings yet
- Acute Coronary SyndromeDocument52 pagesAcute Coronary Syndromeindra muhammadNo ratings yet
- Chest Pain FinalDocument143 pagesChest Pain FinalsaemedNo ratings yet
- Cvs1 - k5 - Cyanotic CHDDocument24 pagesCvs1 - k5 - Cyanotic CHDDumora FatmaNo ratings yet
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- Materi Bapa BagusDocument18 pagesMateri Bapa BagusYadah IkamNo ratings yet
- Pulmonary EmbolismDocument34 pagesPulmonary EmbolismSanjeev Harry BudhooramNo ratings yet
- Deep Vein Thrombosis / Pulmonary EmbolismDocument55 pagesDeep Vein Thrombosis / Pulmonary EmbolismSenti AnnamalaiNo ratings yet
- ACLS ReportDocument58 pagesACLS ReportCamille Honeyleith FernandoNo ratings yet
- Dengue Assessment ChecklistDocument1 pageDengue Assessment ChecklistMitzi BelamideNo ratings yet
- 10 1016@j CCL 2020 04 008Document12 pages10 1016@j CCL 2020 04 008Linda Silvana SariNo ratings yet
- Art Hipertension SecundariaDocument15 pagesArt Hipertension SecundariaLisset FernandezNo ratings yet
- Arritmias en El EmbarazoDocument10 pagesArritmias en El EmbarazoJuan Soto FarfanNo ratings yet
- Table 13-1 Rapid Triage and Transport GuidelinesDocument2 pagesTable 13-1 Rapid Triage and Transport GuidelinesMarios GhobrialNo ratings yet
- Anesthetic Management of Super-Morbidly Obese Parturients For Cesarean Delivery With A Double Neuraxial Catheter Technique: A Case Series (2015)Document5 pagesAnesthetic Management of Super-Morbidly Obese Parturients For Cesarean Delivery With A Double Neuraxial Catheter Technique: A Case Series (2015)Yaneth Tapia MoralesNo ratings yet
- Graded Concept Map 2Document1 pageGraded Concept Map 2api-727701816No ratings yet
- Thoracic Trauma: Keperawatan Gawat Darurat 1 Ns. Siska Natalia, MSN-Palliative CareDocument22 pagesThoracic Trauma: Keperawatan Gawat Darurat 1 Ns. Siska Natalia, MSN-Palliative CareDevi Lamtiur GNo ratings yet
- Obstetric Disorders and Critical Illness - 2022 - Clinics in Chest MedicineDocument18 pagesObstetric Disorders and Critical Illness - 2022 - Clinics in Chest MedicineGustavo ParedesNo ratings yet
- Research Article Microrna-146A Serves As A Biomarker For Adverse Prognosis of St-Segment Elevation Myocardial InfarctionDocument13 pagesResearch Article Microrna-146A Serves As A Biomarker For Adverse Prognosis of St-Segment Elevation Myocardial Infarctionmuhammad sajidNo ratings yet
- Faizal 2021Document11 pagesFaizal 2021muhammad sajidNo ratings yet
- DocuDocument13 pagesDocumuhammad sajidNo ratings yet
- Review Article Meta-Analysis of The Potential Role of Mirna-21 in Cardiovascular System Function MonitoringDocument6 pagesReview Article Meta-Analysis of The Potential Role of Mirna-21 in Cardiovascular System Function Monitoringmuhammad sajidNo ratings yet
- Nazir 2019Document18 pagesNazir 2019muhammad sajidNo ratings yet
- Cardiologist-Level Arrhythmia Detection and Classification in Ambulatory Electrocardiograms Using A Deep Neural NetworkDocument11 pagesCardiologist-Level Arrhythmia Detection and Classification in Ambulatory Electrocardiograms Using A Deep Neural NetworkSuparshva JainNo ratings yet
- Supplementary - Data-2021-Applications of Artificial Intelligencemachine Learning Approaches in Cardiovascular Medicine Systematic Review With RecommendationsDocument52 pagesSupplementary - Data-2021-Applications of Artificial Intelligencemachine Learning Approaches in Cardiovascular Medicine Systematic Review With Recommendationsmuhammad sajidNo ratings yet
- Review Cardiac Hybrid ImagingDocument11 pagesReview Cardiac Hybrid Imagingmuhammad sajidNo ratings yet
- Cardiologist-Level Arrhythmia Detection and Classification in Ambulatory Electrocardiograms Using A Deep Neural NetworkDocument11 pagesCardiologist-Level Arrhythmia Detection and Classification in Ambulatory Electrocardiograms Using A Deep Neural NetworkSuparshva JainNo ratings yet
- Review Image Fusion For CAD DetectionDocument5 pagesReview Image Fusion For CAD Detectionmuhammad sajidNo ratings yet
- Accepted Manuscript: Computers in Biology and MedicineDocument21 pagesAccepted Manuscript: Computers in Biology and Medicinemuhammad sajidNo ratings yet
- Expert Systems With Applications: Jesmin Nahar, Tasadduq Imam, Kevin S. Tickle, Yi-Ping Phoebe ChenDocument9 pagesExpert Systems With Applications: Jesmin Nahar, Tasadduq Imam, Kevin S. Tickle, Yi-Ping Phoebe ChenRohan SahuNo ratings yet
- 10.1007@s10489 019 01461 0Document9 pages10.1007@s10489 019 01461 0muhammad sajidNo ratings yet
- Hardware Matrix InversionDocument4 pagesHardware Matrix Inversionmuhammad sajidNo ratings yet
- Pattern ClassificationDocument41 pagesPattern ClassificationShashaank Mattur AswathaNo ratings yet
- Direct Computation 2. Radix-2 FFT 3. Decimation-In-Time FFT 4. Flowgraphs 5. Bit Reversal Permutation 6. Complexity 7. Decimation-In-Frequency FFTDocument26 pagesDirect Computation 2. Radix-2 FFT 3. Decimation-In-Time FFT 4. Flowgraphs 5. Bit Reversal Permutation 6. Complexity 7. Decimation-In-Frequency FFTveeramaniks408No ratings yet
- 146 PDFDocument6 pages146 PDFmuhammad sajidNo ratings yet
- Pneumonics For AclsDocument2 pagesPneumonics For Aclskrishnaprasadm7100% (2)
- Laporan Kasus Kardio CHF Ec CADDocument35 pagesLaporan Kasus Kardio CHF Ec CADpun212No ratings yet
- Edwards Lifescience Vigileo CatalogoDocument40 pagesEdwards Lifescience Vigileo CatalogoDeni Leonardo TorresNo ratings yet
- 382-Article Text-2683-5-10-20191027Document14 pages382-Article Text-2683-5-10-20191027Nanda NovitaNo ratings yet
- 2017 Hypertension Webinar PDFDocument81 pages2017 Hypertension Webinar PDFMira Mariana UlfahNo ratings yet
- Anatomy and Physiology of Lymphatic SystemDocument24 pagesAnatomy and Physiology of Lymphatic Systemamber tariqNo ratings yet
- Intraosseous Arteriovenous Malformations Mimicking Malignant DiseaseDocument7 pagesIntraosseous Arteriovenous Malformations Mimicking Malignant DiseaseNm SNo ratings yet
- HPNDocument4 pagesHPNFlorianne AdlawanNo ratings yet
- Cardiovascular Drugs: Dr. April Dawn R. LuceroDocument122 pagesCardiovascular Drugs: Dr. April Dawn R. LuceroRjDNo ratings yet
- Therapy ModuleDocument39 pagesTherapy ModuleSuruchi Jagdish SharmaNo ratings yet
- Daftar Diagnosis Dan Kode BPJSDocument18 pagesDaftar Diagnosis Dan Kode BPJSeginagirsangNo ratings yet
- Human Tractus RespiratoriusDocument5 pagesHuman Tractus RespiratoriusDading Satrio SetiawanNo ratings yet
- The Swiss Approach For A Heartbeat-Driven Lead-And Batteryless PacemakerDocument7 pagesThe Swiss Approach For A Heartbeat-Driven Lead-And Batteryless PacemakerIrvansyahNo ratings yet
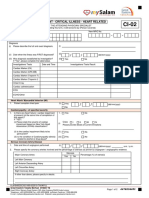
- CI 02 Heart RelatedDocument2 pagesCI 02 Heart RelatedSiti Rohani AhmadNo ratings yet
- #Dr. Lora Ecg PDFDocument53 pages#Dr. Lora Ecg PDFمحمد زينNo ratings yet
- Diastolic Stress Echocardiography PDFDocument23 pagesDiastolic Stress Echocardiography PDFSofia KusumadewiNo ratings yet
- 2019 BLS 1 - Revisi Akhir - PPT - Final DR - APRILDocument34 pages2019 BLS 1 - Revisi Akhir - PPT - Final DR - APRILarga setyo adjiNo ratings yet
- Diferential Diagnosis in Internal Medicine 20879 PDFDocument448 pagesDiferential Diagnosis in Internal Medicine 20879 PDFMarcel Cegodar100% (2)
- Natriuretic Peptide Measurement in NonDocument2 pagesNatriuretic Peptide Measurement in NonAde YonataNo ratings yet
- ACS Management in JKN EraDocument36 pagesACS Management in JKN EraErwin Freddy HutabaratNo ratings yet
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- 47-Article Text-305-1-10-20220731Document10 pages47-Article Text-305-1-10-20220731alyn30274No ratings yet
- Presentor: DR - Kumar Moderator: DR - VamsidharDocument71 pagesPresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyNo ratings yet
- Calcium For Resuscitation?: E. Erdmann and E. Reuschel-JanetschekDocument7 pagesCalcium For Resuscitation?: E. Erdmann and E. Reuschel-JanetschekMislav HilcNo ratings yet
- The Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)Document284 pagesThe Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)AndreaAlexandraNo ratings yet
- Hypoplastic Left Heart SyndromeDocument26 pagesHypoplastic Left Heart SyndromeKhaled S. HarbNo ratings yet
- Neonatal Echo Course 2019Document1 pageNeonatal Echo Course 2019ajes coolNo ratings yet
- DysrhythmiaDocument30 pagesDysrhythmiaJJ JirapathNo ratings yet
- Omcmle Physiology Workbook Part 5 PDFDocument63 pagesOmcmle Physiology Workbook Part 5 PDFloiuse shepiralNo ratings yet
- International Journal of Scientific Research: General MedicineDocument4 pagesInternational Journal of Scientific Research: General MedicineTriple ANo ratings yet