You might also like
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- Screenshot 2023-04-23 at 12.23.43 PM PDFDocument5 pagesScreenshot 2023-04-23 at 12.23.43 PM PDFAditya ChakureNo ratings yet
- Sip 6Document13 pagesSip 6indiz emotionNo ratings yet
- 5663 PDFDocument7 pages5663 PDFwaelNo ratings yet
- Oral Allylestrenol A Pregnancy-Supporting ProgestogenDocument7 pagesOral Allylestrenol A Pregnancy-Supporting Progestogenjefri efendiNo ratings yet
- 5663 PDFDocument7 pages5663 PDFwaelNo ratings yet
- HRTDocument62 pagesHRTArpita ArpitaNo ratings yet
- Induction and Maintenance of Amenorrhea in Transmasculine and Nonbinary AdolescentsDocument6 pagesInduction and Maintenance of Amenorrhea in Transmasculine and Nonbinary AdolescentsdespalitaNo ratings yet
- Evidence From Randomised Trials On The Long-Term Effects of Hormone Replacement TherapyDocument3 pagesEvidence From Randomised Trials On The Long-Term Effects of Hormone Replacement TherapyAnurudh SinghNo ratings yet
- Epilepsy and Oral Hormonal Contraception-Indian Perspective: Review ArticleDocument6 pagesEpilepsy and Oral Hormonal Contraception-Indian Perspective: Review ArticleKirubakaranNo ratings yet
- KIMED1Document9 pagesKIMED1Yolita Satya Gitya UtamiNo ratings yet
- Efficacy and Safety of Long Term Treatment in EndometriosisDocument7 pagesEfficacy and Safety of Long Term Treatment in EndometriosisPt.Natasha AriviaNo ratings yet
- Clinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenDocument10 pagesClinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenGiuseppe NuciferoNo ratings yet
- 4 MG Drospirenone Only Pill New Data and A Review of The Literature PDFDocument8 pages4 MG Drospirenone Only Pill New Data and A Review of The Literature PDFJuly López LeitonNo ratings yet
- 03 Legros Verheulpen PDFDocument5 pages03 Legros Verheulpen PDFErsya MuslihNo ratings yet
- EalahhDocument7 pagesEalahhFauzan AprnNo ratings yet
- Update POC Overview 15012020 NotesDocument35 pagesUpdate POC Overview 15012020 NotesLaurențiu LucaNo ratings yet
- Rethinking Postmenopausal Hormone TherapyDocument2 pagesRethinking Postmenopausal Hormone TherapyDanielle Moon100% (1)
- Menopause Hormone Therapy Latest Developments and Clinical PracticeDocument9 pagesMenopause Hormone Therapy Latest Developments and Clinical PracticeJuan FranciscoNo ratings yet
- Anderson 2002Document10 pagesAnderson 2002GemiNo ratings yet
- ADR News Jul2003 Vol5 No2Document4 pagesADR News Jul2003 Vol5 No2William ChandraNo ratings yet
- Oral ContraceptivesDocument24 pagesOral ContraceptivesSaad MotawéaNo ratings yet
- Sem 16 Lectura 1 AnticoncepcionDocument29 pagesSem 16 Lectura 1 AnticoncepcionEnrique Moncada MapelliNo ratings yet
- Hormonal Contraception (Ahp)Document46 pagesHormonal Contraception (Ahp)burhanNo ratings yet
- Comparative Efficacy of Cyproterone/EE Vs Desogestrel/EE On Acne in PCOD: A Hospital Based Study On 40 PatientsDocument4 pagesComparative Efficacy of Cyproterone/EE Vs Desogestrel/EE On Acne in PCOD: A Hospital Based Study On 40 PatientsGayathriNo ratings yet
- Review Article: Medical Treatments For Endometriosis-Associated Pelvic PainDocument12 pagesReview Article: Medical Treatments For Endometriosis-Associated Pelvic PainponekNo ratings yet
- A22 Comparisonof GN RHagonistandantagonistDocument5 pagesA22 Comparisonof GN RHagonistandantagonistSoumya NagarajanNo ratings yet
- Progestin Only ContraceptionDocument4 pagesProgestin Only ContraceptionTareq SawanNo ratings yet
- The Use of Aromatase Inhibitors in Infertility and GynecologyDocument9 pagesThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNo ratings yet
- Oral Contraceptives in Dermatology: ReviewDocument6 pagesOral Contraceptives in Dermatology: Reviewwilmer lopezNo ratings yet
- Topical Testosterone For Breast Cancer Patients With Vaginal AtrophyDocument8 pagesTopical Testosterone For Breast Cancer Patients With Vaginal Atrophyana.tocha.avtNo ratings yet
- Treatment of Menopausal Symptoms With Hormone TherapyDocument34 pagesTreatment of Menopausal Symptoms With Hormone TherapyJennifer estefania sigcha pujotaNo ratings yet
- Epilepsyinpregnancy: Cynthia Harden,, Christine LuDocument10 pagesEpilepsyinpregnancy: Cynthia Harden,, Christine LuWindy MuldianiNo ratings yet
- (1479683X - European Journal of Endocrinology) A Comparison Between Spironolactone and Spironolactone Plus Finasteride in The Treatment of HirsutismDocument4 pages(1479683X - European Journal of Endocrinology) A Comparison Between Spironolactone and Spironolactone Plus Finasteride in The Treatment of HirsutismSoheil SssNo ratings yet
- Efficacy of Progestogens in The Maintenance of Early Pregnancy in Women With Threatened Miscarriage or Recurrent MiscarriageDocument20 pagesEfficacy of Progestogens in The Maintenance of Early Pregnancy in Women With Threatened Miscarriage or Recurrent MiscarriagesilviuNo ratings yet
- ContraceptivesDocument8 pagesContraceptivesRadowan AhmadNo ratings yet
- Bazedoxifane Dan IbuprofenDocument7 pagesBazedoxifane Dan Ibuprofendita novia maharaniNo ratings yet
- Male and Female HormonesDocument26 pagesMale and Female HormonesZuha HundalNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument12 pagesBest Practice & Research Clinical Obstetrics and GynaecologyMariana HernandezNo ratings yet
- Endometriosis: Long-Term Treatment With Gonadotropin-Releasing Hormone Agonists - UpToDateDocument27 pagesEndometriosis: Long-Term Treatment With Gonadotropin-Releasing Hormone Agonists - UpToDatekodeNo ratings yet
- Management of Premenstrual SyndromeDocument8 pagesManagement of Premenstrual SyndromeNandha D'seRrafindhNo ratings yet
- Ovulation Induction: Embryo Clinic, Krasnodar, RussiaDocument2 pagesOvulation Induction: Embryo Clinic, Krasnodar, RussiaAsh AmeNo ratings yet
- Pharmacology of The Reproductive SystemDocument5 pagesPharmacology of The Reproductive SystemMark Russel Sean LealNo ratings yet
- PIIS0015028207002786 Phytoestrogens in Clinical PracticeDocument7 pagesPIIS0015028207002786 Phytoestrogens in Clinical PracticeGeorge CarpNo ratings yet
- Drugs 2 (Gyneac)Document103 pagesDrugs 2 (Gyneac)Aman Shaikh100% (2)
- Reproductive Pharmacology Lecturio ReflectionDocument7 pagesReproductive Pharmacology Lecturio ReflectionNathaniel SolisNo ratings yet
- s00404 019 05340 4Document8 pagess00404 019 05340 4Tanaporn ThongpolNo ratings yet
- Improvement of Sperm Quality After Micronutrient SupplementationDocument4 pagesImprovement of Sperm Quality After Micronutrient SupplementationalNo ratings yet
- 1 s2.0 S0002937809002713 MainDocument8 pages1 s2.0 S0002937809002713 MaingeraldersNo ratings yet
- Contraception Lec 1Document38 pagesContraception Lec 1fh2785519No ratings yet
- Testosterone and Growth Hormone in Older Men For Better or For WorseDocument4 pagesTestosterone and Growth Hormone in Older Men For Better or For WorseGayathriMaranNo ratings yet
- Estradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)Document12 pagesEstradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)ddandan_2No ratings yet
- Treatment of Endometriosis-Associated Pain With Elagolix - NEJM 2017Document13 pagesTreatment of Endometriosis-Associated Pain With Elagolix - NEJM 2017Lenar AnthonyNo ratings yet
- v18n2 91 DienogestDocument7 pagesv18n2 91 DienogestAnna ReznorNo ratings yet
- Estradiol 10mcg (Vagifen)Document13 pagesEstradiol 10mcg (Vagifen)asdwasdNo ratings yet
- Rind 62 - E62 - 0 PDFDocument6 pagesRind 62 - E62 - 0 PDFFransiska Dina MarseliaNo ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author ManuscriptDivika ShilvanaNo ratings yet
- Testosterone Supplementation in Men: A Practical Guide For The Gynecologist and ObstetricianDocument7 pagesTestosterone Supplementation in Men: A Practical Guide For The Gynecologist and ObstetricianAnca CucuNo ratings yet
- Written Assignment Unit 3Document5 pagesWritten Assignment Unit 3Benses AlvaradoNo ratings yet
- Ocp in Pcos PDFDocument38 pagesOcp in Pcos PDFKeeranmayeeishra0% (1)
- Drug Tariff December 2023Document1,229 pagesDrug Tariff December 2023piNo ratings yet
- Emergency Inhalers in SchoolsDocument22 pagesEmergency Inhalers in SchoolspiNo ratings yet
- Patient Information Leaflet Testosterone Therapy in Women v3Document1 pagePatient Information Leaflet Testosterone Therapy in Women v3piNo ratings yet
- HRT MimsDocument1 pageHRT MimspiNo ratings yet
- Drug Tariff March 2024Document1,245 pagesDrug Tariff March 2024piNo ratings yet
- Drug Tariff December 2023Document1,229 pagesDrug Tariff December 2023piNo ratings yet
- Drug Tariff March 2024Document1,245 pagesDrug Tariff March 2024piNo ratings yet
- Drug Tariff March 2024Document1,245 pagesDrug Tariff March 2024piNo ratings yet
- Berkshire HRTDocument7 pagesBerkshire HRTpiNo ratings yet
- KAPS Paper 1 Sample 1Document34 pagesKAPS Paper 1 Sample 1pi100% (2)
- CAOPexam PDFDocument9 pagesCAOPexam PDFpiNo ratings yet
- KAPS Paper 2 Sample 2Document39 pagesKAPS Paper 2 Sample 2piNo ratings yet
- Specialist Pharmacist JD - RSCH - MAY531!14!1Document9 pagesSpecialist Pharmacist JD - RSCH - MAY531!14!1piNo ratings yet
- KAPS Paper 2 Sample 2Document39 pagesKAPS Paper 2 Sample 2piNo ratings yet
- KAPS Exam Paper For Australian Pharmaceutical Council ExamDocument40 pagesKAPS Exam Paper For Australian Pharmaceutical Council ExampiNo ratings yet
- KAPS Paper 1 Sample 1Document34 pagesKAPS Paper 1 Sample 1pi100% (2)
- Melatonin-Children - Final Updated Amended Sep 2008 Due To Circadin and MHRADocument8 pagesMelatonin-Children - Final Updated Amended Sep 2008 Due To Circadin and MHRApiNo ratings yet
- Melatonin Verdict Update Oct 2013Document2 pagesMelatonin Verdict Update Oct 2013piNo ratings yet
- De Bruyne EUrw 17Document6 pagesDe Bruyne EUrw 17piNo ratings yet
- Neuroleptic Malignat Sy AlimemazinDocument3 pagesNeuroleptic Malignat Sy AlimemazinpiNo ratings yet
- KAPS Paper 2 Sample 1Document33 pagesKAPS Paper 2 Sample 1Syed ArifuddinNo ratings yet
- Melatonin-Children - Final Updated Amended Sep 2008 Due To Circadin and MHRADocument8 pagesMelatonin-Children - Final Updated Amended Sep 2008 Due To Circadin and MHRApiNo ratings yet
- Controlled Trimeprazine Night Waking: Trial of ForDocument6 pagesControlled Trimeprazine Night Waking: Trial of ForpiNo ratings yet
- BMJ Systematic Review InsomniaDocument5 pagesBMJ Systematic Review InsomniapiNo ratings yet
- Bazedoxifenplus Conjugated OestrogensDocument1 pageBazedoxifenplus Conjugated OestrogenspiNo ratings yet
- BazedoxifeneDocument2 pagesBazedoxifenepiNo ratings yet
- France 91Document7 pagesFrance 91piNo ratings yet
- Melatonin ESUOMDocument25 pagesMelatonin ESUOMpiNo ratings yet
- NHS Tayside Flowchart For Systemic HRT Prescribing: AbbreviationsDocument2 pagesNHS Tayside Flowchart For Systemic HRT Prescribing: AbbreviationspiNo ratings yet
- Bazedoxifenplus Conjugated OestrogensDocument1 pageBazedoxifenplus Conjugated OestrogenspiNo ratings yet
- Lectra Fashion e Guide Nurturing EP Quality Logistics Production Crucial To Optimize enDocument8 pagesLectra Fashion e Guide Nurturing EP Quality Logistics Production Crucial To Optimize eniuliaNo ratings yet
- Beyond SyncretismDocument27 pagesBeyond Syncretismz miriamNo ratings yet
- Carbon Trading-The Future Money Venture For IndiaDocument11 pagesCarbon Trading-The Future Money Venture For IndiaijsretNo ratings yet
- Intern CV Pheaktra TiengDocument3 pagesIntern CV Pheaktra TiengTieng PheaktraNo ratings yet
- Animation I Syllabus 2Document3 pagesAnimation I Syllabus 2api-207924970100% (1)
- 26th Sunday in Ordinary Time HNSDocument232 pages26th Sunday in Ordinary Time HNSJeanette FormenteraNo ratings yet
- Psscoc For Design Build 2020Document78 pagesPsscoc For Design Build 2020王佳乐No ratings yet
- My Day: Reading Materials I CourseDocument7 pagesMy Day: Reading Materials I CourseZeynab BagirovaNo ratings yet
- Ele Unit5 Revision PDFDocument2 pagesEle Unit5 Revision PDFNatalia ZapataNo ratings yet
- Reflection of The Movie Informant - RevisedDocument3 pagesReflection of The Movie Informant - RevisedBhavika BhatiaNo ratings yet
- The Global Workforce Crisis BCG PDFDocument28 pagesThe Global Workforce Crisis BCG PDFdakintaurNo ratings yet
- Subjective and Objective DataDocument43 pagesSubjective and Objective DataMingNo ratings yet
- Fault Report MF HFDocument2 pagesFault Report MF HFBrian BennettNo ratings yet
- Roman Empire Revived TheoryDocument173 pagesRoman Empire Revived TheoryBrenoliNo ratings yet
- Green ConcreteDocument19 pagesGreen ConcreteAnubhav KalNo ratings yet
- Supplementary Cause List - 16.10.2023Document7 pagesSupplementary Cause List - 16.10.2023Aamir BhatNo ratings yet
- Inventory Management (Pertemuan V)Document85 pagesInventory Management (Pertemuan V)Asep RahmatullahNo ratings yet
- Civil TutorialDocument638 pagesCivil TutorialEmmanuel Mends FynnNo ratings yet
- House Bill 4208Document1 pageHouse Bill 4208Sinclair Broadcast Group - EugeneNo ratings yet
- Ingles TripticoDocument2 pagesIngles Triptico'YanetCruzRamosNo ratings yet
- Atty. SungaDocument22 pagesAtty. SungaKris MercadoNo ratings yet
- Dental EthicsDocument50 pagesDental EthicsMukhtar Andrabi100% (1)
- Potot Vs People DigestDocument1 pagePotot Vs People DigestMary Grace SevillaNo ratings yet
- Willis, D. - Visualizing Political StruggleDocument11 pagesWillis, D. - Visualizing Political StruggleAndreea Mitreanu100% (3)
- GE1451 NotesDocument18 pagesGE1451 NotessathishNo ratings yet
- A Conceptualization of Vehicle Platoons and Platoon OperationsDocument19 pagesA Conceptualization of Vehicle Platoons and Platoon OperationsWatthanasak JeamwatthanachaiNo ratings yet
- English IODocument6 pagesEnglish IOAarav MathurNo ratings yet
- Nephrotic Syndrome Children PDFDocument11 pagesNephrotic Syndrome Children PDFesdl86No ratings yet
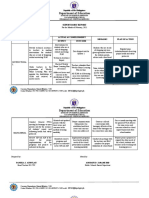
- Department of Education: Supervisory Report School/District: Cacawan High SchoolDocument17 pagesDepartment of Education: Supervisory Report School/District: Cacawan High SchoolMaze JasminNo ratings yet
- Funal ReportDocument2 pagesFunal ReportApril Jay EgagamaoNo ratings yet
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissFrom EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissRating: 4.5 out of 5 stars4.5/5 (81)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutFrom EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutRating: 4 out of 5 stars4/5 (131)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1457)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndFrom EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Peaceful Sleep Hypnosis: Meditate & RelaxFrom EverandPeaceful Sleep Hypnosis: Meditate & RelaxRating: 4.5 out of 5 stars4.5/5 (142)
- Neville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!From EverandNeville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Rating: 5 out of 5 stars5/5 (284)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Summary of The Art of Seduction by Robert GreeneFrom EverandSummary of The Art of Seduction by Robert GreeneRating: 4 out of 5 stars4/5 (46)
- How to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayFrom EverandHow to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayRating: 4.5 out of 5 stars4.5/5 (5)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldFrom EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldRating: 4.5 out of 5 stars4.5/5 (1145)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisFrom EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (2)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo ratings yet
- The Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidFrom EverandThe Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidRating: 4 out of 5 stars4/5 (65)
- The Three Waves of Volunteers & The New EarthFrom EverandThe Three Waves of Volunteers & The New EarthRating: 5 out of 5 stars5/5 (179)
- Queen Bee: A brand new addictive psychological thriller from the author of The BridesmaidFrom EverandQueen Bee: A brand new addictive psychological thriller from the author of The BridesmaidRating: 4 out of 5 stars4/5 (132)
- The Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingFrom EverandThe Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingRating: 4 out of 5 stars4/5 (71)
- The Secret Teachings Of All Ages: AN ENCYCLOPEDIC OUTLINE OF MASONIC, HERMETIC, QABBALISTIC AND ROSICRUCIAN SYMBOLICAL PHILOSOPHYFrom EverandThe Secret Teachings Of All Ages: AN ENCYCLOPEDIC OUTLINE OF MASONIC, HERMETIC, QABBALISTIC AND ROSICRUCIAN SYMBOLICAL PHILOSOPHYRating: 4.5 out of 5 stars4.5/5 (4)