You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Titans and The Twelve OlympiansDocument35 pagesThe Titans and The Twelve OlympiansJariejoy Biore67% (3)
- Comparison of Time Domain Flutter Analysis Using A Reduced Order ModelDocument25 pagesComparison of Time Domain Flutter Analysis Using A Reduced Order ModelTheNo ratings yet
- Physicochemical Characterization of Selected Rice Oryza Sativa Lgenotypes Based On Gel Consistency and Alkali Digestion 2161 1009 1000285 PDFDocument5 pagesPhysicochemical Characterization of Selected Rice Oryza Sativa Lgenotypes Based On Gel Consistency and Alkali Digestion 2161 1009 1000285 PDFJawaria IshfaqNo ratings yet
- Articles - English Lesson PlanDocument7 pagesArticles - English Lesson PlanSneha TaliyanNo ratings yet
- Solubility Improvement of Curcumin Through PVP K-30 Solid DispersionsDocument6 pagesSolubility Improvement of Curcumin Through PVP K-30 Solid Dispersionsuday_khandavilliNo ratings yet
- Q4 HEALTH 9 MODULE 3 WEEK 3 and 4.BetaTestedDocument22 pagesQ4 HEALTH 9 MODULE 3 WEEK 3 and 4.BetaTestedCyris Gay AdolfoNo ratings yet
- US20140245523-Helmet Mountuing Systems - Kopia PDFDocument22 pagesUS20140245523-Helmet Mountuing Systems - Kopia PDFja2ja1No ratings yet
- Episode 68 Transcript - Listening TimeDocument5 pagesEpisode 68 Transcript - Listening TimeSDMK Dinkes DKINo ratings yet
- Mcqs On Virology by Misango Da Phd.Document101 pagesMcqs On Virology by Misango Da Phd.Musa yohana100% (2)
- 1964 1obli ChronicleDocument12 pages1964 1obli Chronicleapi-198872914No ratings yet
- High Voltage - 2020 - Su - Electrical Tree Degradation in High Voltage Cable Insulation Progress and ChallengesDocument12 pagesHigh Voltage - 2020 - Su - Electrical Tree Degradation in High Voltage Cable Insulation Progress and ChallengesLuiz KowalskiNo ratings yet
- JósmentaDocument3 pagesJósmentaadorjánvNo ratings yet
- Water Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationDocument2 pagesWater Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationlovlyNo ratings yet
- Cafeteria and Management ReviewerDocument16 pagesCafeteria and Management ReviewerGhibi TrinidadNo ratings yet
- VxRail 7.0.x Release NotesDocument39 pagesVxRail 7.0.x Release NotesphongnkNo ratings yet
- PHP SQL AnywhereDocument7 pagesPHP SQL Anywherecool03No ratings yet
- 03.2 ENSTP - 2019 Aggregates PART1Document24 pages03.2 ENSTP - 2019 Aggregates PART1VEHERNo ratings yet
- APC2100 Device Number Key V2.0Document1 pageAPC2100 Device Number Key V2.0mmbb89No ratings yet
- Hydraulics 11Document11 pagesHydraulics 11Gerald OrtizNo ratings yet
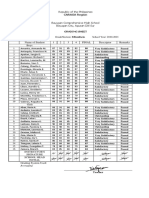
- Ma Angela Kristine Valencia - B. Grading Sheet Fili - 8Document1 pageMa Angela Kristine Valencia - B. Grading Sheet Fili - 8Ma. Angela Kristine ValenciaNo ratings yet
- 2nd Quarter Exam Empowerment - TechnologiesDocument3 pages2nd Quarter Exam Empowerment - Technologieskathryn soriano100% (11)
- Xviii The Roots of CalculusDocument3 pagesXviii The Roots of CalculusDaniel VargasNo ratings yet
- Pidgin - God's Simple PlanDocument3 pagesPidgin - God's Simple PlanAfrica BiblesNo ratings yet
- Famous Writters-WPS OfficeDocument3 pagesFamous Writters-WPS OfficeMelmel TheKnightNo ratings yet
- Soliton WavesDocument42 pagesSoliton WavesAbdalmoedAlaiashyNo ratings yet
- Parliamentary Election Impact W14299-PDF-ENGDocument8 pagesParliamentary Election Impact W14299-PDF-ENGHarshit ShubhankarNo ratings yet
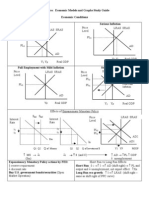
- AP Macroeconomic Models and Graphs Study GuideDocument23 pagesAP Macroeconomic Models and Graphs Study GuideAznAlexT90% (21)
- Asterismos Famosos Observacion Phil HarringtonDocument3 pagesAsterismos Famosos Observacion Phil HarringtonMaria TeresaNo ratings yet
- Types of Forces: Previously in This LessonDocument3 pagesTypes of Forces: Previously in This LessonRayyanNo ratings yet
- LIGHT - MIRROR Practice QuestionsDocument2 pagesLIGHT - MIRROR Practice Questionsshrish000000100% (1)