You might also like
- Introduction To CounselingDocument27 pagesIntroduction To CounselingajazNo ratings yet
- BSC 09092017Document72 pagesBSC 09092017ajazNo ratings yet
- The Nursing Assessment Cheat Sheet (ADPIE)Document3 pagesThe Nursing Assessment Cheat Sheet (ADPIE)ajaz100% (1)
- Understanding Disabilitypdf PDFDocument17 pagesUnderstanding Disabilitypdf PDFArnold ArubaNo ratings yet
- NHS Employers Bullying Measures Final ReportDocument58 pagesNHS Employers Bullying Measures Final ReportajazNo ratings yet
- Least Two Negative Acts, Weekly or More Often, For Six or More Months in Situations WhereDocument1 pageLeast Two Negative Acts, Weekly or More Often, For Six or More Months in Situations WhereajazNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Fce Speaking Test ChecklistDocument2 pagesFce Speaking Test Checklist冰泉100% (1)
- Negligence - Breach of Duty: The Reasonable Man TestDocument4 pagesNegligence - Breach of Duty: The Reasonable Man Testnamram1414No ratings yet
- English For ComunicationDocument15 pagesEnglish For ComunicationWardah WardielaNo ratings yet
- Vpa ReflDocument2 pagesVpa Reflapi-298564847No ratings yet
- Pragmatic ResearcherDocument14 pagesPragmatic ResearcherAbderrahim ChalfaouatNo ratings yet
- Stuvia 521677 Summary Strategy An International Perspective Bob de Wit 6th Edition PDFDocument86 pagesStuvia 521677 Summary Strategy An International Perspective Bob de Wit 6th Edition PDFRoman BurbakhNo ratings yet
- Thesis Format With SD (BSCS)Document4 pagesThesis Format With SD (BSCS)kathleencate0% (1)
- Air Properties Lesson PlanDocument2 pagesAir Properties Lesson Planapi-489169715No ratings yet
- (Akira Takayama) Analytical Methods in EconomicsDocument693 pages(Akira Takayama) Analytical Methods in EconomicsCarla Valverde España100% (4)
- Be Unconventional Planner 2022Document92 pagesBe Unconventional Planner 2022GayeGabriel100% (1)
- Anticipating Strategy DecayDocument14 pagesAnticipating Strategy DecayRoshela KhanNo ratings yet
- Documented Essay About EmojisDocument8 pagesDocumented Essay About EmojisSweet MulanNo ratings yet
- Toyota Forklift 02 5fg28!02!5fg30 Parts CatalogDocument22 pagesToyota Forklift 02 5fg28!02!5fg30 Parts Catalognathanielsmith070288xgd100% (115)
- Simple Past TenseDocument10 pagesSimple Past TenseEka FitriNo ratings yet
- Ethics From The MarginDocument20 pagesEthics From The MarginOvia HerbertNo ratings yet
- Manipulatives in Maths TechingDocument4 pagesManipulatives in Maths TechingerivickNo ratings yet
- What Is The Self by Michael D. Moga, S.J.Document2 pagesWhat Is The Self by Michael D. Moga, S.J.Rachelle Alexis Ingente100% (2)
- DuBois, The Pan-Africanist and The Development of African Nationalism - Brandon KendhammerDocument22 pagesDuBois, The Pan-Africanist and The Development of African Nationalism - Brandon KendhammerElmano MadailNo ratings yet
- Begbie, Jeremy Theology, Music and TimeDocument331 pagesBegbie, Jeremy Theology, Music and TimeEdNg100% (1)
- Wolf, Werner and Bernhart, Walter (Ed.) - Description in Literature and Other MediaDocument352 pagesWolf, Werner and Bernhart, Walter (Ed.) - Description in Literature and Other MediaElNegroLiterario100% (3)
- Mintal Comprehensive High School: Detailed Lesson Plan (DLP) SY 2019-2020Document4 pagesMintal Comprehensive High School: Detailed Lesson Plan (DLP) SY 2019-2020Teofilo BuenoNo ratings yet
- 4 Methods of Philosophizing ScientificDocument23 pages4 Methods of Philosophizing ScientificVanessa May AbarcaNo ratings yet
- Mathematical Model To Design Rack and Pinion Ackerman Steering GeomteryDocument5 pagesMathematical Model To Design Rack and Pinion Ackerman Steering GeomteryIntiGowthamSai100% (1)
- How Google WorksDocument9 pagesHow Google WorksHoangDuongNo ratings yet
- Demonstration Teaching PlanDocument6 pagesDemonstration Teaching PlanBagwis Maya100% (2)
- LORDocument3 pagesLORKuldeep SaxenaNo ratings yet
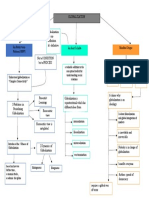
- GCWORLD Concept MapDocument1 pageGCWORLD Concept MapMoses Gabriel ValledorNo ratings yet
- Rumaysa Bint MilhanDocument2 pagesRumaysa Bint Milhanabou78No ratings yet
- Word of MouthDocument141 pagesWord of MouthMurali MuthusamyNo ratings yet
- A Study of The Semiotics of Print AdvertisementsDocument42 pagesA Study of The Semiotics of Print AdvertisementsMay100% (1)