You might also like
- Master Key Bonus - The Healing CodeDocument8 pagesMaster Key Bonus - The Healing CodeChanterelle Vasto100% (12)
- Adult Mental Health CMHT SOP SummaryDocument19 pagesAdult Mental Health CMHT SOP SummaryRafael Sebastian100% (1)
- GORUCK Heavy - 6-week training program overviewDocument4 pagesGORUCK Heavy - 6-week training program overviewJohn Rohrer100% (2)
- Septic Abortion PDFDocument4 pagesSeptic Abortion PDFmariachrismayaniNo ratings yet
- Treatment of Macular EdemaDocument48 pagesTreatment of Macular EdemaPushpanjali RamtekeNo ratings yet
- GAD Accomplishment ReportDocument1 pageGAD Accomplishment ReportRenante Naga100% (6)
- Dowell's Price List 18.3.2022Document26 pagesDowell's Price List 18.3.2022Sunil WadekarNo ratings yet
- Comparison of Subfoveal Choroidal Thickness ValuesDocument7 pagesComparison of Subfoveal Choroidal Thickness ValuesNurul Ramadhani MustafaNo ratings yet
- 9-Original ArticleDocument4 pages9-Original Articlearthur.fleck.997No ratings yet
- RomJOphthalmol 59 252Document3 pagesRomJOphthalmol 59 252angiNo ratings yet
- Glaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandraDocument5 pagesGlaucoma and Diabetes - Is There An Association? Jain Shashi, Lakhtakia Sujata, Tirkey Eva Rani, Jain Sheel ChandranjmdrNo ratings yet
- GlaukomaDocument9 pagesGlaukomaddpNo ratings yet
- Social Approach to Diabetic Retinopathy in Nigeria (39Document14 pagesSocial Approach to Diabetic Retinopathy in Nigeria (39Emmanuel OgochukwuNo ratings yet
- Prevalence and Risk Factors of Thyroid-Associated Ophthalmopathy Among IndiansDocument4 pagesPrevalence and Risk Factors of Thyroid-Associated Ophthalmopathy Among IndiansLastry WardaniNo ratings yet
- Landmark Studies in GlaucomaDocument53 pagesLandmark Studies in GlaucomaDrEknathPawarNo ratings yet
- 1 s2.0 S1056872722000071 MainDocument5 pages1 s2.0 S1056872722000071 Maindzaky fadhilNo ratings yet
- LUTFI-FULL PAPER-PIT 2024Document6 pagesLUTFI-FULL PAPER-PIT 2024Lutfi MaulanaNo ratings yet
- Association of HbA1c Levels and Diabetic Retinopathy SeverityDocument6 pagesAssociation of HbA1c Levels and Diabetic Retinopathy SeverityYoga TDNo ratings yet
- Clinical and Epidemiology: Relationship between age and intraocular pressureDocument3 pagesClinical and Epidemiology: Relationship between age and intraocular pressurePutri YingNo ratings yet
- Prevalence of Normal Tension Glaucoma in AsiaDocument4 pagesPrevalence of Normal Tension Glaucoma in AsiaSonia RogersNo ratings yet
- DM Dan GlaukomaDocument5 pagesDM Dan GlaukomaYandhie RahmanNo ratings yet
- Use of β‑Blockers and Risk of Age‑Related Macular Degeneration Among Hypertensive PatientsDocument9 pagesUse of β‑Blockers and Risk of Age‑Related Macular Degeneration Among Hypertensive PatientsMierNo ratings yet
- Assessment of Color Vision in Diabetic Patients: Tarek M Radwan, Ehab M Ghoneim, Waleed A Ghobashy, Ahmed A OrmaDocument10 pagesAssessment of Color Vision in Diabetic Patients: Tarek M Radwan, Ehab M Ghoneim, Waleed A Ghobashy, Ahmed A OrmaSuresh NairNo ratings yet
- Aos0091 0406Document7 pagesAos0091 0406maandre123No ratings yet
- Predictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusDocument6 pagesPredictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusdrheriNo ratings yet
- Steriod Cataract PDFDocument4 pagesSteriod Cataract PDFLisa IskandarNo ratings yet
- Correlation Between Systemic Risk Factors and Diabetic Macular Edema in Diabetes Mellitus - Dian Paramitasari 1Document8 pagesCorrelation Between Systemic Risk Factors and Diabetic Macular Edema in Diabetes Mellitus - Dian Paramitasari 1Hutami Sri UmmiyatiNo ratings yet
- RF GlaucomaDocument6 pagesRF Glaucomamaandre123No ratings yet
- Glaucoma American Journal of OphtalmologyDocument7 pagesGlaucoma American Journal of OphtalmologyListya NormalitaNo ratings yet
- Jurnal Mata 2Document30 pagesJurnal Mata 2Reza AryantiNo ratings yet
- Bjophthalmol 2016 310063.fullDocument7 pagesBjophthalmol 2016 310063.fullEvenjelina EveNo ratings yet
- Retinal Nerve Fiber Layer and Ganglion Cell Complex Thickness in Patients With Type 2 Diabetes Mellitus Original ArticleDocument2 pagesRetinal Nerve Fiber Layer and Ganglion Cell Complex Thickness in Patients With Type 2 Diabetes Mellitus Original ArticledrblurryfaceNo ratings yet
- Effect of Focal Laser Photocoagulation in Eyes With Mild To Moderate Non-Proliferative Diabetic RetinopathyDocument5 pagesEffect of Focal Laser Photocoagulation in Eyes With Mild To Moderate Non-Proliferative Diabetic RetinopathyyheyenNo ratings yet
- Jurnal Reading GlaucomaDocument6 pagesJurnal Reading GlaucomawidyawirapNo ratings yet
- Effect of Latanoprost on Central Corneal ThicknessDocument4 pagesEffect of Latanoprost on Central Corneal ThicknessrandyhermawanNo ratings yet
- PDML Article1Document4 pagesPDML Article1kingdeyNo ratings yet
- Correlation Between Diabetic Cognitive Impairment and Diabetic Retinopathy in Patients With T2DM by 1H-MRSDocument7 pagesCorrelation Between Diabetic Cognitive Impairment and Diabetic Retinopathy in Patients With T2DM by 1H-MRSppdsretinaNo ratings yet
- Diabetic Retinopathy 2013 ArticleDocument3 pagesDiabetic Retinopathy 2013 ArticleRe-zha 'Putra'No ratings yet
- Role of Flicker Perimetry in Predicting Onset of Late-Stage Age-Related Macular DegenerationDocument10 pagesRole of Flicker Perimetry in Predicting Onset of Late-Stage Age-Related Macular DegenerationHarold Estiven MarinNo ratings yet
- Advances in managing diabetic macular edema based on evidence from DRCR.net studiesDocument11 pagesAdvances in managing diabetic macular edema based on evidence from DRCR.net studiesNatalia LeeNo ratings yet
- Am J Ophthalmol 2004 - p401Document6 pagesAm J Ophthalmol 2004 - p401Abrilia OctafijayantiNo ratings yet
- Treatment Outcomes in The DRy Eye Amniotic MembraneDocument5 pagesTreatment Outcomes in The DRy Eye Amniotic MembraneDiny SuprianaNo ratings yet
- Axial Myopia and Low HbA1c Level Are Correlated AnDocument8 pagesAxial Myopia and Low HbA1c Level Are Correlated AnGeert SmoldNo ratings yet
- Jurnal HighlightDocument4 pagesJurnal HighlightStrangersNo ratings yet
- Papers: Treatment of Ocular Hypertension and Open Angle Glaucoma: Meta-Analysis of Randomised Controlled TrialsDocument3 pagesPapers: Treatment of Ocular Hypertension and Open Angle Glaucoma: Meta-Analysis of Randomised Controlled TrialsDanil Anugrah JayaNo ratings yet
- Journal Reading Presentation GinaDocument12 pagesJournal Reading Presentation GinaRegina FristasariNo ratings yet
- Articulo Fisio 3Document7 pagesArticulo Fisio 3Oumaima Ahaddouch ChiniNo ratings yet
- Tham 2020 Oi 200342Document10 pagesTham 2020 Oi 200342Oscar Julian Perdomo CharryNo ratings yet
- Epidemiology and Clinical Characteristics of Patients With Glaucoma: An Analysis of Hospital Data Between 2003 and 2012 Original ArticleDocument7 pagesEpidemiology and Clinical Characteristics of Patients With Glaucoma: An Analysis of Hospital Data Between 2003 and 2012 Original Articlesyntacs skNo ratings yet
- JOVRDocument5 pagesJOVRkrishan bansalNo ratings yet
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials: EditorialsDocument4 pagesIntensive Glycemic Control in The ACCORD and ADVANCE Trials: EditorialsMarco CarvajalNo ratings yet
- Risk factors for diabetic foot in IndonesiaDocument4 pagesRisk factors for diabetic foot in IndonesiaFernando SilalahiNo ratings yet
- Evaluation of Ocular Manifestations in Type 2 Diabetes MellitusDocument5 pagesEvaluation of Ocular Manifestations in Type 2 Diabetes MellitusDona Parenta NantaliaNo ratings yet
- Barriers To Glaucoma Medication Compliance Among Veterans: Dry Eye Symptoms and Anxiety DisordersDocument5 pagesBarriers To Glaucoma Medication Compliance Among Veterans: Dry Eye Symptoms and Anxiety DisorderssrngmNo ratings yet
- 1 s2.0 S0039625722000455 MainDocument14 pages1 s2.0 S0039625722000455 Maindr. Yaltafit Abror JeemNo ratings yet
- tmp1617 TMPDocument7 pagestmp1617 TMPFrontiersNo ratings yet
- Appendix B: Analysis Plan/Application Data/materialsDocument6 pagesAppendix B: Analysis Plan/Application Data/materialsOtieno MosesNo ratings yet
- PSJ - Volume 3 - Issue 2 - Pages 203-205Document3 pagesPSJ - Volume 3 - Issue 2 - Pages 203-205SamuelRexyNo ratings yet
- Natural History and Outcome of Optic Pathway Gliomas in ChildrenDocument7 pagesNatural History and Outcome of Optic Pathway Gliomas in ChildrenCamilo Benavides BurbanoNo ratings yet
- Imp Landmark Glauc StudiesDocument100 pagesImp Landmark Glauc StudiesASHOK KUMAR SINGHNo ratings yet
- 2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADDocument4 pages2017 - Bansal - Corelation of HbA1c Levels and Duration of Diabetes With PADbuat nugas28No ratings yet
- Risk Factors For High-Risk Proliferative Diabetic RetinopathyDocument20 pagesRisk Factors For High-Risk Proliferative Diabetic RetinopathyOdilia Rondang Mauli SimarmataNo ratings yet
- Makale Neo-Adma - Eng V2Document12 pagesMakale Neo-Adma - Eng V2Thomas LeonNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)From EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)No ratings yet
- Biophysical Properties in Glaucoma: Diagnostic TechnologiesFrom EverandBiophysical Properties in Glaucoma: Diagnostic TechnologiesIngrida JanulevicieneNo ratings yet
- Comment. in This Case, The Excimer Laser Was Used in ADocument3 pagesComment. in This Case, The Excimer Laser Was Used in ARafael SebastianNo ratings yet
- Rainie YangDocument3 pagesRainie YangRafael SebastianNo ratings yet
- QUIZ 1-EAP - Med-AB With AnswersDocument24 pagesQUIZ 1-EAP - Med-AB With AnswersRafael SebastianNo ratings yet
- Exercise helps lower high blood pressureDocument2 pagesExercise helps lower high blood pressureRafael SebastianNo ratings yet
- Research Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaDocument6 pagesResearch Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaRafael SebastianNo ratings yet
- Daftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019Document113 pagesDaftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019FarhanNo ratings yet
- The Dangers of Cramming and Computers in EducationDocument11 pagesThe Dangers of Cramming and Computers in EducationRafael SebastianNo ratings yet
- QUIZ 1-EAP - Med-AB With AnswersDocument24 pagesQUIZ 1-EAP - Med-AB With AnswersRafael SebastianNo ratings yet
- The Open Microbiology JournalDocument10 pagesThe Open Microbiology Journalnoor ainNo ratings yet
- Comment. in This Case, The Excimer Laser Was Used in ADocument3 pagesComment. in This Case, The Excimer Laser Was Used in ARafael SebastianNo ratings yet
- 99149246Document11 pages99149246Retma Rosela NurkayantyNo ratings yet
- 1750 1172 5 39Document11 pages1750 1172 5 39Agus TianaNo ratings yet
- Stevens-Johnson Syndrome and Abuse of Anabolic SteroidsDocument4 pagesStevens-Johnson Syndrome and Abuse of Anabolic SteroidsRafael SebastianNo ratings yet
- Eye 2013280 ADocument7 pagesEye 2013280 A18juni1995No ratings yet
- Research Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaDocument6 pagesResearch Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaRafael SebastianNo ratings yet
- Photoretinitis: An Underestimated Occupational Injury?Document4 pagesPhotoretinitis: An Underestimated Occupational Injury?Rafael SebastianNo ratings yet
- Eye 2013280 ADocument7 pagesEye 2013280 A18juni1995No ratings yet
- Research Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaDocument6 pagesResearch Article Assessment of The Use of Safety Devices by Welders in Osogbo, NigeriaRafael SebastianNo ratings yet
- Hubungan Perilaku Diet Dengan Kadar Gula Darah Pada Penderita Diabetes Melitus Tipe Ii (Di Desa Jogomerto Kecamatan Tanjung Anom)Document9 pagesHubungan Perilaku Diet Dengan Kadar Gula Darah Pada Penderita Diabetes Melitus Tipe Ii (Di Desa Jogomerto Kecamatan Tanjung Anom)Rafael SebastianNo ratings yet
- Ocular Effects of Chronic Exposure To Welding Light On Calabar Welders K. G. Davies U. Asana C. O. Nku and E. E. OSIMDocument4 pagesOcular Effects of Chronic Exposure To Welding Light On Calabar Welders K. G. Davies U. Asana C. O. Nku and E. E. OSIMRafael SebastianNo ratings yet
- Pengaruh Ukuran Potongan Kopra Dalam Proses Pengeringan: Effect of The Copra Cut Size in The Drying ProcessDocument5 pagesPengaruh Ukuran Potongan Kopra Dalam Proses Pengeringan: Effect of The Copra Cut Size in The Drying ProcessAlexia Desi Ratnasari Loi 1841100210No ratings yet
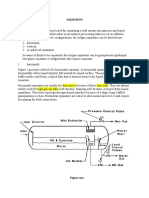
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Chap 24 Econ 40Document4 pagesChap 24 Econ 40Racel DelacruzNo ratings yet
- Thai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)Document32 pagesThai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)DibbaSotaNanaNo ratings yet
- Make Every Day Count: George Eliot's inspirational poemDocument3 pagesMake Every Day Count: George Eliot's inspirational poemRUTUJA KALENo ratings yet
- LV CB Catalogue PDFDocument260 pagesLV CB Catalogue PDFBoobesh Kumar SekarNo ratings yet
- Ufara QasrinDocument14 pagesUfara Qasrinroni setiawanNo ratings yet
- 85 HP John Deere 4045DFM50 Marine Diesel EngineDocument2 pages85 HP John Deere 4045DFM50 Marine Diesel EngineDAVIDNo ratings yet
- Winged Scapula Caused by Dorsal Scapular.21Document4 pagesWinged Scapula Caused by Dorsal Scapular.21emilio9fernandez9gatNo ratings yet
- Providing Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityDocument62 pagesProviding Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityBenjamae MaqueNo ratings yet
- Inside Out or Outside In. Meeting With Couples. Hugh JenkinsDocument24 pagesInside Out or Outside In. Meeting With Couples. Hugh JenkinsRita1976No ratings yet
- STC Bec Wir Plu D 0209 01 PDFDocument10 pagesSTC Bec Wir Plu D 0209 01 PDFAdel MorsyNo ratings yet
- SITE. Defining Project Goals & ObjectivesDocument1 pageSITE. Defining Project Goals & Objectivescoach balaNo ratings yet
- C612Document5 pagesC612dinhtung2210100% (1)
- SECTION 03380 Post-Tensioned Concrete Rev 1Document30 pagesSECTION 03380 Post-Tensioned Concrete Rev 1Abdalrahman AntariNo ratings yet
- Starbucks BSC Project Analyzes Store PerformanceDocument8 pagesStarbucks BSC Project Analyzes Store Performanceandrea100% (1)
- Will The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityDocument2 pagesWill The Real SMART Goals Please Stand Up?: Robert S. Rubin Saint Louis UniversityKyoko TakayanagiNo ratings yet
- InfraTapp - Infra Tapp - Manual ENGDocument64 pagesInfraTapp - Infra Tapp - Manual ENGEliaNo ratings yet
- Della Core DutiesDocument12 pagesDella Core DutiesSt SNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- Government Schemes Current Affairs PDF E Book PDFDocument106 pagesGovernment Schemes Current Affairs PDF E Book PDFRohini VjNo ratings yet
- Importance and Uses of Medicinal Plants - An Overview: December 2016Document8 pagesImportance and Uses of Medicinal Plants - An Overview: December 2016safamanz001 safaNo ratings yet
- Perfect Scale Pro ManualDocument9 pagesPerfect Scale Pro ManualAnthony VargasNo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Dahong PalayDocument2 pagesDahong PalayAngela MontenegroNo ratings yet