You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eng 3Document20 pagesEng 3Saifan siddiqueNo ratings yet
- Sr. Inspection Engineer Sample ResumeDocument4 pagesSr. Inspection Engineer Sample ResumemaheshNo ratings yet
- CongenitalcholesteatomaDocument20 pagesCongenitalcholesteatomaMeilina Elin WardhaniNo ratings yet
- API 510 Open Book Practice ExamDocument48 pagesAPI 510 Open Book Practice Examcorey jacobsNo ratings yet
- Motor Purge ControllerDocument2 pagesMotor Purge ControllerRONNEL DOMINGONo ratings yet
- Mechatronics & AutomationDocument9 pagesMechatronics & AutomationAnandababuNo ratings yet
- Paper 2 2018 121 EN LP 000 PDFDocument7 pagesPaper 2 2018 121 EN LP 000 PDFFatiha HAMDINo ratings yet
- Digha Nikaya 1. Silakkhandhavagga (Tr. U Htin Fatt, by DPPS) OCRedDocument384 pagesDigha Nikaya 1. Silakkhandhavagga (Tr. U Htin Fatt, by DPPS) OCRedTatagatha Amoghasiddhi Deividas ČepelėNo ratings yet
- PDB-Gross Domestic Product (GDP) - InggrisDocument7 pagesPDB-Gross Domestic Product (GDP) - InggrisPradiptaAdiPamungkasNo ratings yet
- Green Day SongsDocument28 pagesGreen Day SongsUzziah's WorldNo ratings yet
- Nishas Play School, GoaDocument6 pagesNishas Play School, Goasuhana80% (10)
- A Multi-Loop Low-Dropout FVF Voltage Regulator With Enhanced Load RegulationDocument4 pagesA Multi-Loop Low-Dropout FVF Voltage Regulator With Enhanced Load RegulationAram ShishmanyanNo ratings yet
- Boettcher ThermodynamicsDocument78 pagesBoettcher ThermodynamicsCHE.ENG1734No ratings yet
- Handout3 Schrock CarbeneDocument3 pagesHandout3 Schrock CarbeneEustance JuanNo ratings yet
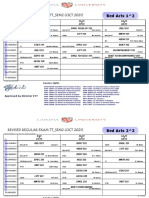
- Revised Regular Exam TT - Sem2 (Oct 2021) : Bed Arts 1 2Document78 pagesRevised Regular Exam TT - Sem2 (Oct 2021) : Bed Arts 1 2kelvinNo ratings yet
- bài tập đọc hiểu 2Document11 pagesbài tập đọc hiểu 2xoanxapxinharmyNo ratings yet
- LIM40E 13 For 48V TelecomDocument2 pagesLIM40E 13 For 48V TelecomBD0% (1)
- BurnerDocument2 pagesBurnerVishnu PatidarNo ratings yet
- Characteristics and Classification of PCMDocument10 pagesCharacteristics and Classification of PCMJinto A JNo ratings yet
- Complemento Uchile (Semigrupos)Document18 pagesComplemento Uchile (Semigrupos)robertoNo ratings yet
- BA 301 Final ReportDocument29 pagesBA 301 Final ReportSamNo ratings yet
- CLB20703 Chemical Engineering Thermodynamics Experiment 2: Performance Characteristics of Steam PlantDocument3 pagesCLB20703 Chemical Engineering Thermodynamics Experiment 2: Performance Characteristics of Steam PlantSiti Hajar MohamedNo ratings yet
- Bags of Little BootstrapsDocument44 pagesBags of Little BootstrapsAbel SNo ratings yet
- Ruckus Complete Product Guide 2013Document3 pagesRuckus Complete Product Guide 2013Atul DeshpandeNo ratings yet
- Smart-Ups On-Line Srt3000xla ApcDocument2 pagesSmart-Ups On-Line Srt3000xla ApcKatty CachagoNo ratings yet
- A Glossary On Psychology LibraryDocument3 pagesA Glossary On Psychology LibraryTVKMNo ratings yet
- DIFFERENT TYPE OF DRAWING Based On MediaDocument23 pagesDIFFERENT TYPE OF DRAWING Based On MediaLeslyn Bangibang DiazNo ratings yet
- Lightning Protection Systems Advantages and DisadvantagesDocument11 pagesLightning Protection Systems Advantages and DisadvantagesRamiro Magbanua FelicianoNo ratings yet
- Ranchi OfficesDocument4 pagesRanchi Officesrajarammohanrai40No ratings yet
- CA3162Document8 pagesCA3162marcelo riveraNo ratings yet