Research
Medical tourism in Thailand: a cross-sectional study
Thinakorn Noree,a Johanna Hanefeldb & Richard Smithc
Objective To investigate the magnitude and characteristics of medical tourism in Thailand and the impact of such tourism on the Thai
health system and economy.
Methods In 2010, we checked the records of all visits to five private hospitals that are estimated to cover 63% of all foreign patients. We
reviewed hospital records of foreign patients and obtained data on their countries of origin, diagnoses and interventions. We surveyed
293 medical tourists to collect demographic characteristics and information on their expenditure and travelling companions. To help
understand the impact of medical tourism on the Thai health system, we also interviewed 15 hospital executives and 28 service providers
from the private hospitals.
Findings We obtained 911 913 records of hospital visits, of which 324 906 came from 104 830 medical tourists. We estimated that there
were 167 000 medical tourists in Thailand in 2010. Of the medical tourists who attended our study hospitals, 67 987 (64.8%) came from
the eastern Mediterranean region or Asia and 109 509 (34%) of them were treated for simple and uncomplicated conditions – i.e. general
check-ups and medical consultations. The mean self-reported non-medical expenditure was 2750 United States dollars. According to the
hospital staff interviewed, medical tourism in 2010 brought benefits to – and apparently had no negative impacts on – the Thai health
system and economy.
Conclusion We estimate that the total number of medical tourists visiting Thailand is about 10% of previous national government estimates
of 1.2 million. Such tourists appear to bring economic benefits to Thailand and to have negligible effects on the health system.
land and provided an estimated revenue of approximately
Introduction US$ 1.1 billion – i.e. about 9% of Thailand’s total estimated
Although reliable estimates of the annual number of people revenue from tourism in 2006.19,20 Between the start of 2004
travelling abroad to purchase medical services – so-called and end of 2008, medical tourism was estimated to have
medical tourists – are difficult to identify, there has been a rise brought Thailand US$ 7.5 billion in revenue.20
in medical tourism in the past decade.1 The increasing costs Since 2003, the Thai Government has attempted to make
of health care and the expansion of the middle class in many Thailand a global centre for medical tourism through a Centre
low- and middle-income countries have led to an increase in of Excellent Health Care of Asia initiative. Efforts at patient
such tourism.2–4 recruitment have included international road shows and tax
The global gross profit from medical tourism has been exemptions for investment in new health facilities that target
estimated to be about 60 billion United States dollars (US$) medical tourists.21
per year and to be growing by about 20% annually.5,6 Most The Thai Government appreciates the potential of foreign
studies of medical tourism have focused on the residents of patients as a source of foreign currency earnings. In 2011,
North America, western Europe and the eastern Mediterra- it was estimated that revenues from medical tourists would
nean region, many of whom have high purchasing power.7,8 generate the equivalent of 0.4% of Thailand’s gross domestic
In 2007, an estimated 50 000–120 000 residents of the United product.19 Despite such financial benefits, there is considerable
States of America travelled abroad to obtain medical services.9 concern about the equity impact of medical tourism, especially
In 2010, an estimated 63 000 residents of the United Kingdom in areas where the health systems are weak and the resources
of Great Britain and Northern Ireland also travelled abroad may have to be diverted towards the care of patients from
for medical care – mainly for fertility, cosmetic or bariatric abroad.19 Another concern is the current lack of regulation
treatments10 and predominately to Asia, eastern Europe, the and oversight of the providers of medical tourism.22 Ethical
Caribbean or South America.11–14 issues have been raised in relation to patients travelling after
Medical tourism has often been portrayed as involving pa- being given very limited information23 and foreign patients
tients from high-income countries travelling to access cheaper purchasing organs or surrogacy services from local popula-
care in low- and middle-income countries.15 However, a more tions in low- and middle-income countries.24,25 The world’s
complex market – with increasing numbers of medical tourists media recently described a boy who was born with Down
from low- and middle-income countries – is emerging. 16,17 syndrome to a surrogate mother in Thailand before being
Regardless of the direction of travel, some middle-income reportedly abandoned by his Australian parents.26
countries have been positioning themselves as destination At present the division between those promoting the
countries for medical tourism.18 economic benefits of medical tourism and those convinced
The Thai Ministry of Commerce estimated that, in 2006, of the damaging effects of such tourism on health systems
1.2 million medical tourists accessed health services in Thai- is unbridgeable because much of the discussion is based on
a
International Health Policy Program, Ministry of Public Health, Tiwanon Road, Nonthaburi 11000, Thailand.
b
Department of Global Health and Development, London School of Hygiene & Tropical Medicine, London, England.
c
Faculty of Public Health and Policy, London School of Hygiene & Tropical Medicine, London, England.
Correspondence to Thinakorn Noree (email: thinakorn@ihpp.thaigov.net).
(Submitted: 26 December 2014 – Revised version received: 30 September 2015 – Accepted: 14 October 2015 – Published online: 9 December 2015 )
30 Bull World Health Organ 2016;94:30–36 | doi: http://dx.doi.org/10.2471/BLT.14.152165
Research
Thinakorn Noree et al. Medical tourism in Thailand
poor empirical evidence. 27,28 Here we Table 1. Areas of origin of the medical tourists attending five hospitals, Thailand, 2010
attempt to provide further evidence by
investigating the extent and the impact Origin No. of medical tourists (%)
of medical tourism in Thailand.
Eastern Mediterranean 40 554 (38.7)
South-east Asia 14 730 (14.1)
Methods Europe 14 004 (13.4)
Five private hospitals were purposively South Asia 12 703 (12.1)
selected for a survey. According to an North America 9 481 (9.0)
unpublished survey of 55 hospitals East Asia 4 166 (4.0)
conducted by the Thai Ministry of Com- Africa 3 957 (3.8)
merce in 2007, the five selected hospitals Australasia 3 949 (3.8)
together took 63% of all foreign patients Unknown 1 252 (1.2)
visiting Thailand – with the remaining Other area 34 (0.0)
37% diffusely distributed across the Total 104 830 (100.0)
other 50 hospitals surveyed across the
country (Department of International
Trade Promotion, Thai Ministry of the records that involved at least one ist’s expenditure and companions. The
Commerce, unpublished observations, procedure to code for the related organ interviewers were nurses and translators
2007). Three of the surveyed hospitals system involved. from the hospitals, who had to take a
are in Bangkok and the other two are Between May and August of 2012, to half-day training course in data collec-
in the major tourist destinations of help understand the impact of medical tion to standardize the interview process
Chonburi and Phuket. Each surveyed tourism on the Thai health system, we and minimize data collection errors. The
hospital provides many foreign patients conducted face-to-face semi-structured interviews were held in Arabic, English
with highly specialized tertiary care and interviews with 43 key informants – i.e. or Japanese. All interviewees provided
tailored service packages. 15 hospital executives and 28 service written informed consent.
In a cross-sectional survey designed providers – from four of the surveyed The study protocol was approved
to identify all of the medical tourists hospitals that gave permission for such by the ethics committees of the London
who sought medical services at any of interviews. In the category of hospital School of Hygiene & Tropical Medicine
the surveyed hospitals in 2010, we ana- executives, we interviewed chief execu- and each study hospital. The initial find-
lysed the records of all 911 913 hospital tive officers, hospital directors, medical ings were triangulated, for validity and
visits that occurred between 1 January directors, human resources directors the reduction of bias, in a presentation to
2010 and 31 December 2010. These or marketing directors. The questions policy-makers and related stake-holders
records, which we retrieved from each for this category assessed hospitals’ in March 2014.
hospital’s electronic database, included policies on serving foreign patients and
diagnoses coded according to the Inter- on handling the revenue generated by Results
national Classification of Diseases, tenth these patients. In the category of service
Numbers of medical tourists
revision (ICD-10).29 Foreign patients providers we interviewed doctors or
who had a permanent postal address nurses about how the services delivered We identified 104 830 medical tourists
in Thailand, had lived in Thailand for to medical tourists differed from local who each visited one of the five sur-
more than six months and/or were residents. veyed hospitals in 2010. These tourists
employed in Thailand were considered In another series of interviews, we accounted for 44.3% of the 236 885
to be expatriates and not medical tour- investigated medical tourists, mainly to foreign patients identified in the hos-
ists. Following the advice of clinicians assess their expenditure while in Thai- pital records and for 324 906 (35.6%) of
from the surveyed hospitals, foreign land. We recruited these interviewees the 911 913 attendances by foreigners.
patients who had – according to their by consecutive case selection in the The mean number of visits per tourist
ICD-10 codes – presented with acute same hospitals as the key informants was 3.1.
illnesses such as common cold and between June and September of 2012.
Origins of medical tourists
acute diarrhoea or as the result of minor We used a probability-proportional-to-
accidents were assumed to be tour- size sampling technique to account for The medical tourists were less likely to
ists who had fallen ill or been injured the between-hospital differences in the be residents of high-income countries in
while on holiday in Thailand. All other annual number of medical tourists. Our North America or Australasia than to be
foreign patients were considered to be target – based on the available relevant residents of the eastern Mediterranean
medical tourists and their attendance data, a 5% level of precision and a 95% or south-east or south Asia (Table 1).
records were analysed in terms of six confidence interval – was to interview The highest numbers of medical tour-
demographic or service-use variables: 578 medical tourists. Interviews were ists in Thailand in 2010 came from the
(i) country of origin; (ii) treated as an based on an unpublished questionnaire United Arab Emirates (21 568), followed
inpatient or outpatient; (iii) diagnosis; used by the Thai Ministry of Tourism by Bangladesh (8443), the USA (7855)
(iv) type of procedure; (v) length of stay: and Sports for a survey of general tour- and Myanmar (7568); (Table 2).
and (vi) medical expenditure. To stan- ist expenditure. This questionnaire was
dardize data extraction among hospitals, designed to collect demographic char-
we used ICD-9 clinical modification for acteristics and information on the tour-
Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165 31
Research
Medical tourism in Thailand Thinakorn Noree et al.
Table 2. Origins of medical tourists attending five hospitals, Thailand, 2010 ture for themselves of US$ 2750, and
US$ 2678 for their companions – spent
Rank Origin No. (%) Mean no. of visits mainly on accommodation, food,
drinks and shopping. Medical tourists
Medical tourists Visits per medical tourist
and companions who had travelled on
(n = 104 830) (n = 324 906) long-haul flights – e.g. from Australasia,
1 United Arab 21 568 (20.57) 63 457 (19.53) 2.94 Europe and North America – spent an
Emirates average of US$ 2142 and US$ 2387,
2 Bangladesh 8443 (8.05) 26 338 (8.11) 3.12 respectively, on traditional tourist
3 United States 7855 (7.49) 24 262 (7.47) 3.09 activities within Thailand. This was
4 Myanmar 7568 (7.22) 32 940 (10.14) 4.35 considerably less than the correspond-
5 Oman 7096 (6.77) 21 699 (6.68) 3.06 ing values – of US$ 3031 and US$ 2800,
6 Qatar 5212 (4.97) 17 784 (5.47) 3.41 respectively – for the medical tourists
and companions who had travelled
7 United Kingdom 3935 (3.75) 10 779 (3.32) 2.74
shorter distances within Asia.
8 African countries 3857 (3.68) 17 491 (5.38) 4.53
other than South Using our estimated numbers and
Africaa expenditures, we estimated that the
9 Cambodia 3837 (3.66) 10 919 (3.36) 2.85 gross tourism revenue from medical
10 Australia 3360 (3.21) 10 136 (3.12) 3.02 tourists and their companions in 2012
was approximately US$ 900 million.
11 Kuwait 3159 (3.01) 11 330 (3.49) 3.59
12 Japan 1995 (1.90) 4681 (1.44) 2.35
13 France 1742 (1.66) 4275 (1.32) 2.45 Discussion
14 Germany 1545 (1.47) 3780 (1.16) 2.45 Together the five surveyed hospitals had
15 Canada 1474 (1.41) 4115 (1.27) 2.79 been estimated to handle 63% of medi-
a
The hospitals categorized the origins of African patients as “South Africa” or “other African countries”. cal tourists in Thailand, which would
Note: The table only represents the top 15 countries. indicate from our results that there
were about 167 000 medical tourists
Interviews with hospital executives who attended Thai hospitals in 2010.
Procedures
and service providers indicated no dif- Our estimate of medical tourists falls
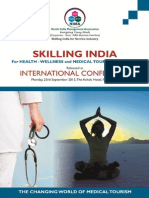
Fig. 1 shows the organ system in- ference in the key aspects of clinical care far below the national government es-
volved in medical or surgical services between foreign and domestic patients. timate of 1.2 million in 200619 and puts
purchased by medical tourists from Whatever their origins, patients were into doubt the accuracy of the projected
Australia, the United Arab Emirates reportedly treated according to the same figure of some 7 million foreign patients
and the USA. Medical tourists from medical guidelines. However, there were being seen in Thailand in 2015.21 Earlier
the USA most frequently purchased some differences in terms of peripheral estimates have probably been affected by
cosmetic surgery procedures (on the services, such as provision of a transla- the failure to separate medical tourists
integumentary system), followed by or- tor, transfer services from the airport from expatriates, immigrants and tour-
thopaedic operations (musculoskeletal) and special food for medical tourists. ists who have simply fallen ill or been
and eye operations. Cosmetic surgery Difficulties in communication often injured while on holiday in Thailand.
accounted for most of the services meant that doctors and nurses spent Another potential cause of inaccuracy
purchased by Australian patients, while more time with a medical tourist than is that Thai hospitals traditionally re-
patients from the United Arab Emirates with a domestic patient. However, all port the number of foreign patients
primarily purchased digestive system of our interviewees were adamant that by the number of visits – rather than
surgeries. the reported differences – and medical the number of patients – and, as we
tourism in general – did not affect the observed, each foreign patient may ac-
Impacts
overall quality of medical services that count for multiple visits in any year. The
The 104 830 medical tourists represented they provided to any patient. possibility remains that other national
approximately 14% of the 734 150 pa- and global estimates of the numbers of
Non-medical expenditure
tients seen at our five surveyed hospi- medical tourists are also far too high.
tals in 2010. They represented a small Time constraints of the study meant It was once thought that most
proportion of the private patients seen that we only interviewed 293 medi- medical tourists from North America
in hospitals across Thailand in the same cal tourists – i.e. 50.7% of the target and Europe were seeking complicated
period – and an even smaller proportion sample. Only 100 (34%) had arranged procedures when they travelled to
of the patients seen at any Thai hospital. to visit Thailand solely for medical ser- Thailand for medical care.30 However,
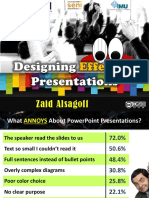
Furthermore, of the 324 906 visits by vices. Another 54 (18%) had decided to this study and others have found that
medical tourists, 303 167 (93%) were seek medical care in the country after most such tourists travel to Thailand
outpatient-only and 109 509 (34%) were they had arrived. About half (151) had for minor elective procedures, such as
only for a general check-up, a medi- travelled to Thailand with at least one cosmetic surgery.31 In contrast, we found
cal consultation or for the treatment companion. that medical tourists visiting Thailand
of a simple, uncomplicated condition The medical tourists we interviewed from the United Arab Emirates were
(Fig. 2). reported a mean non-medical expendi- generally purchasing services such as
32 Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165
Research
Thinakorn Noree et al. Medical tourism in Thailand
Fig. 1. Most commonly-recorded procedures or targeted systems among medical tourists from three countries attending five hospitals,
Thailand, 2010
900
Australia
800 United Arab Emirates
United States of America
700
600
No. of medical tourists
500
400
300
200
100
0
Integumentary Digestive Miscellaneous Musculoskeletal Eye Female genital Other procedure Cardiovascular
system system therapeutic system organ system
procedure
Reported procedure or targeted system
Notes: The procedures targeted at the integumentary system were mostly cosmetic. Cardiac catheterizations accounted for most of the “miscellaneous therapeutic
procedures” and angiocardiograms accounted for most of the “other procedures”.
Fig. 2. Most commonly-recorded diseases of medical tourists and Thai patients attending five hospitals, Thailand, 2010
40
Medical tourists
35 Thai patients
30
25
% of patients
20
15
10
0
None Disease of Disease of Disease of Endocrine Disease of Neoplasm Disease of Disease of eye Infectious or
digestive genitourinary musculoskeletal nutritional or circulatory skin or or ocular parasitic
system system system or metabolic system subcutaneous adnexa disease
connective tissue disease tissue
Recorded disease
Note: When no disease was reported, the tourist or Thai patient was usually attending hospital solely for a health check-up or medical consultation.
cardiac catheterization, angiocardio- public hospitals accounted for 80% of cal schools and one private one – that
grams, other cardiovascular procedures beds,33 although private hospitals have together produce about 2500 new gradu-
and gastric bypasses. a proportionately larger role in Bangkok ates annually,34 there remains a shortfall
The Thai health system is pre- and other urban centres. Of the 35 789 in doctors. It has been estimated that at
dominantly public, with a relatively physicians working in Thailand in 2009, the current rate of training, Thailand
small proportion of patients visiting 82.9% worked in the public sector. 33 will not achieve its targeted physician
private health facilities. 32 In 2008, Although Thailand has 18 public medi- density – of one per 1500 people – until
Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165 33
Research
Medical tourism in Thailand Thinakorn Noree et al.
2020. 34 The situation is compounded and interview results indicate that medi- to Thailand should affect non-medical
by the distribution of doctors, with an cal tourism is on such a small scale in expenditure in Thailand but one pos-
acute shortage in rural areas. In 2009, Thailand that its effect on the domestic sibility is that the long-haul medical
there was one doctor per 565 people in health system is marginal. If such tour- tourists and companions are, in gen-
Bangkok but only one per 2870 people ism does have any detrimental effect it eral, less affluent compared with their
in the north-eastern provinces.33 This is likely to be primarily via its impact on short-haul counterparts and so spend
inequitable distribution may be made the distribution of doctors. Most of the less on accommodation, food, drinks
worse by doctors moving from tertiary doctors and nurses who work in private and shopping.
public hospitals to urban private hospi- hospitals in Thailand have been trained
tals. Part of this flow has been attributed in the public sector, through the use of
to the large numbers of medical tourists public funds. However, the results from
Conclusion
attending urban private hospitals.21,32 this study indicate that it is the provi- Medical tourists in Thailand do not
There have been few empirical sion of private health care to residents form a homogeneous group. They are a
studies examining the impacts of medi- of Thailand that drives most of the flow mix of patients who travel with serious
cal tourism in Thailand on the health of doctors to the private sector. health issues and those seeking minor
system. In 2006, it was estimated that Medical tourists make a net con- treatments while taking a holiday. Their
176–303 additional doctors would be tribution to the domestic economy, numbers have been over-estimated in
required to service foreign patients by not only in terms of their medical the past. They appear to have a negligible
2015 – i.e. 9–12% of the additional doc- spending but also, frequently, in terms effect on the national health system but
tors that were estimated to be needed for of their spending on traditional tour- do contribute to the Thai tourism in-
the entire national health system.21 In ist activities. In 2012, the Ministry of dustry. A medical tourist tax, to channel
2011, however, it was estimated that far Tourism and Sports estimated that each some of the proceeds from the tourism
more additional doctors – i.e. 528–909 – non-medical tourist spent a mean of industry into the health system, could be
would be required to service foreign pa- US$ 80335 whereas – according to our considered to redistribute some of these
tients by 2015.19 However, both of these interviews and excluding any medical gains to the sector that is providing the
estimates of the numbers of additional expenditure – the medical tourists and relevant services. ■
doctors required were based on esti- their companions each spent more than
mates of the numbers of medical tourists three times this figure in the same year. Competing interests: None declared.
that now appear far too high. Our survey It is unclear why the distance travelled
ملخص
القطاعات متعددة دراسة:تايلند يف طبية ألغراض السياحة
سائح167000 وتشري تقديراتنا إىل توافد.ألغراض السياحة الغرض استقصاء حجم السياحة ألغ��راض طبية يف تايلند
(بنسبة67987 وكان.2010 ألغراض طبية يف تايلند يف عام وخصائصها وتأثري هذا النوع من السياحة عىل النظام الصحي
) من بني السائحني ألغ��راض طبية الذين قدموا إىل64.8% .واالقتصاد يف البالد
املستشفيات التي شملتها دراستنا قادمني من منطقة رشق البحر الطريقة فحصنا سجالت مجيع الزيارات يف مخس مستشفيات خاصة
) منهم العالج فيام34% (بنسبة109509 وتلقى،املتوسط أو آسيا ، من مجيع املرىض األجانب وف ًقا للتقديرات63% تشمل خدماهتا
يتعلق بحاالت بسيطة وغري معقدة – أي ملجرد إجراء فحوصات وراجعنا سجالت املستشفيات املتعلقة.2010 وذلك يف عام
وبلغ متوسط النفقات غري.طبية عامة وبح ًثا عن استشارات طبية باملرىض األجانب كام حصلنا عىل بيانات عن البلدان األصلية التي
وطب ًقا ملا ورد. دوالر أمريكي2750 الطبية وف ًقا ملا ذكره أصحاهبا 293 واستطلعنا آراء. والتدخالت، والتشخيصات،ينتمون إليها
عادت،يف املقابالت التي تم إجراؤها مع العاملني باملستشفيات من السياح القادمني ألغراض طبية جلمع اخلصائص الديموغرافية
بالنفع عىل النظام الصحي2010 السياحة ألغراض طبية يف عام كام أجرينا.هلم واملعلومات املتعلقة بالنفقات ورفقاء السفر
. دون أي تأثريات سلبية بادية عليهام،واالقتصاد التايلندي من28 من املسؤولني التنفيذيني باملستشفيات و15 مقابالت مع
بلغت نسبة إمجايل عدد السياح القادمني،االستنتاج وف ًقا لتقديراتنا وذلك للمساعدة،مقدمي اخلدمات العاملني باملستشفيات اخلاصة
مليون وف ًقا1.2 من10% إىل تايلند ألغ��راض طبية حوايل عىل استيعاب تأثري السياحة ألغراض طبية عىل النظام الصحي
وحقق هذا النوع من السياح.لتقديرات احلكومة الوطنية السابقة .التايلندي
بعض املنافع االقتصادية لتايلند يف ظاهر األمر وكان له تأثريات ،ال لزيارات املستشفيات ً سج911913 النتائج حصلنا عىل
.طفيفة عىل النظام الصحي وافدً ا104830 زيارة منها كانت من324906 ووجدنا أن
摘要
泰国医疗旅游 :横断面研究
目的 旨在调查泰国医疗旅游的规模和特征,以及此类 所有外国患者总数的 63%。我们查看了外国患者的就
旅游对于泰国卫生系统和经济的影响。 医记录,并且获得了有关其原籍国、诊断和干预措施
方法 在 2010 年,我们翻查了五家私立医院的所有就 的资料。我们调查了 293 位医疗游客,收集了人口统
诊记录。据估计,这五家私立医院接诊的外国患者占 计特征及其开支和旅伴方面的信息。为了帮助了解医
34 Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165
Research
Thinakorn Noree et al. Medical tourism in Thailand
疗旅游对泰国卫生系统的影响,我们还采访了私营医 般的体检和医疗咨询。平均自我报告的非医疗支出
院中的 15 位医院主管和 28 位医务人员。 为 2750 美元。据接受采访的医院工作人员称,医疗旅
结 果 我 们 获 得 911 913 项 医 院 就 诊 记 录, 其 中 游在 2010 年给泰国的卫生系统和经济带来了效益,显
有 324 906 项 来 自 104 830 位 医 疗 游 客。 我 们 估 然没有任何负面影响。
计 2010 年中有 167 000 位医疗游客入境泰国。在我们 结论 我们估计,在国家政府先前估算的 120 万游客中,
研究的医院中,接诊的 67 987 (64.8%) 位医疗游客来 前往泰国的医疗游客总数约占 10%。此类游客显然给
自东地中海地区和亚洲,其中 109 509 (34%) 位医疗 泰国带来了经济效益,对卫生系统产生的影响微不足
游客的病情简单且不复杂,在治疗过程中接受了一 道。
Résumé
Le tourisme médical en Thaïlande: étude transversale
Objectif Étudier l’ampleur et les caractéristiques du tourisme médical avons estimé que 167 000 touristes étaient venus en Thaïlande pour
en Thaïlande et l’impact de ce type de tourisme sur le système de santé raison médicale en 2010. Parmi les touristes médicaux qui se sont rendus
et l’économie du pays. dans les hôpitaux de notre étude, 67 987 (64,8%) venaient de la région de
Méthodes En 2010, nous avons examiné les dossiers de toutes les la Méditerranée orientale ou d’Asie et 109 509 (34%) d’entre eux étaient
consultations réalisées dans cinq hôpitaux privés qui recevaient, selon traités pour des affections simples et sans complications – contrôles
les estimations, 63% de l’ensemble des patients étrangers. Nous avons d’ordre général et consultations médicales. Les dépenses moyennes
consulté les dossiers d’hospitalisation des patients étrangers et recueilli déclarées de nature autre que médicale s’élevaient à 2750 dollars des
des informations sur leur pays d’origine, le diagnostic et les interventions États-Unis. Selon le personnel hospitalier interrogé, en 2010, le tourisme
pratiquées. Nous avons interrogé 293 touristes médicaux afin d’en médical a eu des effets bénéfiques - et apparemment pas d’impact
savoir plus sur leurs caractéristiques démographiques, leurs dépenses négatif - sur le système de santé et l’économie thaïlandais.
ainsi que leurs accompagnateurs. Afin de mieux comprendre l’impact Conclusion Nous estimons que le nombre total de touristes se
du tourisme médical sur le système de santé thaïlandais, nous avons rendant en Thaïlande pour raison médicale représente environ 10%
également interrogé 15 cadres hospitaliers et 28 prestataires de services des précédentes estimations nationales du gouvernement, qui étaient
de ces hôpitaux privés. de 1,2 millions. Ce type de tourisme semble apporter des bénéfices
Résultats Nous avons examiné 911 913 dossiers de consultations en économiques pour la Thaïlande, avec des effets négligeables sur le
hôpital, dont 324 906 concernaient 104 830 touristes médicaux. Nous système de santé.
Резюме
Медицинский туризм в Таиланде: одномоментное поперечное исследование
Цель Изучить масштабы и характеристики медицинского посетивших исследуемые больницы, 67 987 (64,8%) прибыли
туризма в Таиланде и влияние туризма такого вида на систему из стран Восточного Средиземноморья или Азии, а
здравоохранения и экономику Таиланда. 109 509 (34%) лечились от простых и неосложненных заболеваний,
Методы В 2010 году были просмотрены записи всех посещений т. е. проходили общий медицинский осмотр и получали
пяти частных больниц, которые, согласно подсчетам, обслуживают консультацию врача. Немедицинские расходы, о которых
63% всех иностранных пациентов. Были проанализированы исследуемые пациенты сообщали самостоятельно, в среднем
больничные записи иностранных пациентов и получены составили 2750 долларов США. По сообщениям опрошенных
данные о странах их происхождения, диагнозах и врачебном сотрудников больниц, медицинский туризм в 2010 году
вмешательстве. Были опрошены 293 туриста-пациента, на оказал положительное воздействие и, судя по всему, не имел
основании чего получены демографические характеристики и негативного влияния на систему здравоохранения и экономику
сведения об их расходах и сопровождающих их лицах. Для оценки Таиланда.
влияния медицинского туризма на систему здравоохранения Вывод Согласно нашим подсчетам общее количество
Таиланда были также опрошены 15 руководителей больниц и туристов-пациентов, посетивших Таиланд, составляет
28 поставщиков услуг из частных больниц. приблизительно 10% от ранее определенного национальным
Результаты Были получены 911 913 записей о посещении правительством числа в 1,2 миллиона. Туристы, посещающие
больниц, 324 906 из которых поступили от 104 830 туристов- страну с такой целью, приносят экономическую пользу
пациентов. Согласно подсчетам в 2010 году Таиланд посетили Таиланду и оказывают несущественное влияние на систему
167 000 туристов-пациентов. Из всех туристов-пациентов, здравоохранения.
Resumen
Turismo sanitario en Tailandia: un estudio transversal
Objetivo Investigar la magnitud y las características del turismo sanitario los pacientes extranjeros. Se revisaron los registros hospitalarios de los
en Tailandia y el impacto de dicho turismo sobre el sistema sanitario y pacientes extranjeros y se obtuvieron datos de sus países de origen,
la economía del país. diagnósticos e intervenciones. Se encuestó a 293 turistas sanitarios
Métodos En 2010 se comprobaron los registros de todas las visitas a para recopilar características demográficas e información sobre sus
cinco hospitales privados que se estima que cubren el 63% de todos gastos y compañeros de viaje. También se entrevistó a 15 ejecutivos
Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165 35
Research
Medical tourism in Thailand Thinakorn Noree et al.
de hospitales y 28 proveedores de servicios de hospitales privados gastos autodeclarados en gastos no médicos fue de 2.750 dólares
para ayudar a entender el impacto del turismo sanitario en el sistema estadounidenses. De acuerdo con el personal hospitalario entrevistado,
sanitario tailandés. el turismo sanitario en 2010 trajo beneficios a (y aparentemente no tuvo
Resultados Se obtuvieron 911.913 registros de visitas hospitalarias, de un efecto negativo sobre) el sistema sanitario y la economía de Tailandia.
los cuales 324.906 provenían de 104.830 turistas sanitarios. Se estimó Conclusión Se estima que el total de los turistas sanitarios que visitan
que en 2010 hubo 167.000 turistas sanitarios en Tailandia. De los turistas Tailandia es cerca del 10% de las anteriores estimaciones del gobierno
sanitarios que atendieron los hospitales analizados, 67.987 (64,8%) nacional de 1,2 millones. Esta clase de turistas parece traer beneficios
provenían de la región del Mediterráneo Oriental o Asia y 109.509 económicos a Tailandia y no tienen efectos negativos en el sistema
(34%) fueron tratados de condiciones simples y sin complicaciones. sanitario.
Es decir, chequeos generales y consultas médicas. El promedio de
References
1. Connell J. Contemporary medical tourism: conceptualisation, culture 19. NaRanong A, NaRanong V. The effects of medical tourism: Thailand’s
and commodification. Tourism Manage. 2013;34:1–13. doi: http://dx.doi. experience. Bull World Health Organ. 2011 May 1;89(5):336–44. doi: http://
org/10.1016/j.tourman.2012.05.009 dx.doi.org/10.2471/BLT.09.072249 PMID: 21556301
2. Bies W, Zacharia L. Medical tourism: outsourcing surgery. Math 20. Thailand: medical hub of Asia [Technical report]. Nonthaburi: Office of the
Comput Model. 2007;46(7-8):1144–59. doi: http://dx.doi.org/10.1016/j. Civil Servant Commission; 2010.
mcm.2007.03.027 21. Pachanee CA, Wibulpolprasert S. Incoherent policies on universal coverage
3. Hopkins L, Labonté R, Runnels V, Packer C. Medical tourism today: what is of health insurance and promotion of international trade in health services
the state of existing knowledge? J Public Health Policy. 2010 Jul;31(2):185– in Thailand. Health Policy Plan. 2006 Jul;21(4):310–8. doi: http://dx.doi.
98. doi: http://dx.doi.org/10.1057/jphp.2010.10 PMID: 20535101 org/10.1093/heapol/czl017 PMID: 16728511
4. Horowitz MD, Rosensweig JA. Medical tourism – health care in the global 22. Smith R, Lunt N, Hanefeld J. The implications of PIP are more than just
economy. Physician Exec. 2007 Nov-Dec;33(6):24–6,. PMID: 18092615 cosmetic. Lancet. 2012 Mar 31;379(9822):1180–1. doi: http://dx.doi.
5. Heung V, Kucukusta D, Song H. Medical tourism development in Hong org/10.1016/S0140-6736(12)60166-4 PMID: 22305764
Kong: an assessment of the barriers. Tourism Manage. 2011;32(5):995–1005. 23. Snyder J, Crooks VA. Medical tourism and bariatric surgery: more moral
doi: http://dx.doi.org/10.1016/j.tourman.2010.08.012 challenges. Am J Bioeth. 2010 Dec;10(12):28–30. doi: http://dx.doi.org/10.1
6. Herrick MD. Medical tourism: global competition in healthcare. Dallas: 080/15265161.2010.528510 PMID: 21161839
National Center for Policy Analysis; 2007. Available from: http://www.ncpa. 24. Crush J, Chikanda A, Maswikwa B. Patients without borders: medical tourism
org/pdfs/st304.pdf [cited 2015 Sep 13]. and medical migration in southern Africa. Cape Town: Megadigital; 2012.
7. Medical tourism: consumers in search of value. Washington: Deloitte Center for 25. Whittaker A, Speier A. “Cycling overseas”: care, commodification, and
Health Solutions; 2008. Available from http://www.academia.edu/9144718/ stratification in cross-border reproductive travel. Med Anthropol. 2010
Medical_Tourism_Consumers_in_Search_of_Value_Produced_by_the_ Oct;29(4):363–83. doi: http://dx.doi.org/10.1080/01459740.2010.501313
Deloitte_Center_for_Health_Solutions [cited 2015 Sep 10]. PMID: 21082483
8. Connell J. Medical tourism: sea, sun, sand and surgery. Tourism Manage. 26. Baby Gammy may be given Australian citizenship, government suggests.
2006;27(6):1093–100. doi: http://dx.doi.org/10.1016/j.tourman.2005.11.005 The Guardian. 2014 Aug 4. Available from: http://www.theguardian.com/
9. Johnson TJ, Garman AN. Impact of medical travel on imports and exports of world/2014/aug/04/baby-gammy-australian-citizenship-government-
medical services. Health Policy. 2010 Dec;98(2-3):171–7. doi: http://dx.doi. suggests [cited 2014 Aug 5].
org/10.1016/j.healthpol.2010.06.006 PMID: 20619919 27. Hanefeld J, Smith R, Horsfall D, Lunt N. What do we know about medical
10. Hanefeld J, Horsfall D, Lunt N, Smith R. Medical tourism: a cost or benefit tourism? A review of the literature with discussion of its implications for the
to the NHS? PLoS ONE. 2013;8(10):e70406. doi: http://dx.doi.org/10.1371/ UK National Health Service as an example of a public health care system.
journal.pone.0070406 PMID: 24204556 J Travel Med. 2014 Nov-Dec;21(6):410–7. doi: http://dx.doi.org/10.1111/
11. Tattara G. Medical tourism and domestic population health [working jtm.12147 PMID: 25156070
paper]. Venice: University of Venice; 2010. Available from: http://papers.ssrn. 28. Smith R, Martínez Álvarez M, Chanda R. Medical tourism: a review of the
com/sol3/papers.cfm?abstract_id=1544224 [cited 2014 Aug 12]. literature and analysis of a role for bi-lateral trade. Health Policy. 2011
12. Connell J, Fara X. Medical tourism in the Caribbean Islands: a cure for Dec;103(2-3):276–82. doi: http://dx.doi.org/10.1016/j.healthpol.2011.06.009
economies in crisis? Isl Stud J. 2013;8:115–30. PMID: 21767892
13. Lautier M. Export of health services from developing countries: the case of 29. International statistical classifications of diseases and related health
Tunisia. Soc Sci Med. 2008 Jul;67(1):101–10. doi: http://dx.doi.org/10.1016/j. problems, 10th revision. Geneva: World Health Organization; 2010. Available
socscimed.2008.01.057 PMID: 18468756 from: http://apps.who.int/classifications/icd10/browse/2010/en [cited 2014
14. Kangas B. Hope from abroad in the international medical travel of Jul 18].
Yemeni patients. Anthropol Med. 2007;14(3):293–305. doi: http://dx.doi. 30. Executive summary: a development of Thailand medical hub policy.
org/10.1080/13648470701612646 Nonthaburi: Ministry of Public Health; 2010.
15. Mazzaschi A. Surgeon and safari: producing valuable bodies in 31. Noree T, Hanefeld J, Smith R. UK medical tourists in Thailand: they are not
Johannesburg. Signs (Chic). 2011;36(2):303–12. doi: http://dx.doi. who you think they are. Global Health. 2014;10(1):29. doi: http://dx.doi.
org/10.1086/655941 PMID: 21114075 org/10.1186/1744-8603-10-29 PMID: 24885204
16. Crush J, Chikanda A. South-South medical tourism and the quest for health 32. Wibulpolprasert S, Pengpaibon P. Integrated strategies to tackle
in southern Africa. Soc Sci Med. 2015 Jan;124:313–20. doi: http://dx.doi. the inequitable distribution of doctors in Thailand: four decades of
org/10.1016/j.socscimed.2014.06.025 PMID: 24973022 experience. Hum Resour Health. 2003 Nov 25;1(1):12. doi: http://dx.doi.
17. Lunt N, Horsfall D, Smith R, Exworthy M, Hanefeld J, Mannion R. org/10.1186/1478-4491-1-12 PMID: 14641940
Market size, market share and market strategy: three myths of 33. Thailand health profile 2008–2010. Nonthaburi: The War Veterans
medical tourism. Policy Polit. 2014;42(4):597–614. doi: http://dx.doi. Organization of Thailand; 2012.
org/10.1332/030557312X655918 34. Suphanchaimat R, Wisaijohn T, Thammathacharee N, Tangcharoensathien V.
18. Leng CH. Medical tourism and the state in Malaysia and Projecting Thailand physician supplies between 2012 and 2030: application
Singapore. Glob Soc Policy. 2010;10(3):336–57. doi: http://dx.doi. of cohort approaches. Hum Resour Health. 2013;11(1):3. doi: http://dx.doi.
org/10.1177/1468018110379978 org/10.1186/1478-4491-11-3 PMID: 23374250
35. Report on international tourists in Thailand in 2012. Nonthaburi: Ministry of
Tourism and Sports; 2012. Available from: http://www.tourism.go.th/home/
details/11/222/2137 [cited 2015 Sep 13].
36 Bull World Health Organ 2016;94:30–36| doi: http://dx.doi.org/10.2471/BLT.14.152165
You might also like
- Genesis ApeDocument7 pagesGenesis Apefer sotoNo ratings yet
- The Effects of Medical Tourism: Thailand's Experience by Anchana NaRanong & Viroj NaRanongDocument9 pagesThe Effects of Medical Tourism: Thailand's Experience by Anchana NaRanong & Viroj NaRanongViroj NaRanongNo ratings yet
- Practice and Determinants of Medical Tourism in NigeriaDocument7 pagesPractice and Determinants of Medical Tourism in NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- How To Promote International Medical Tourism in Southeast AsiaDocument6 pagesHow To Promote International Medical Tourism in Southeast AsiazarishNo ratings yet
- SoukyaDocument5 pagesSoukyaBonnyMJoyNo ratings yet
- Medical Tourism Ethics Risks and Benefits IJPERDocument10 pagesMedical Tourism Ethics Risks and Benefits IJPERHealthcare Pro LearningNo ratings yet
- The Analysis Factor of Medical Tourism in Singapore: MartinDocument9 pagesThe Analysis Factor of Medical Tourism in Singapore: MartinBibiana CardenasNo ratings yet
- Health hubs in Asia attract foreign patients with affordable careDocument6 pagesHealth hubs in Asia attract foreign patients with affordable careHasan ErkenNo ratings yet
- Medical Tourism in Thailand: A Comparison of Yahnee Hospital and Johns Hopkins HospitalDocument8 pagesMedical Tourism in Thailand: A Comparison of Yahnee Hospital and Johns Hopkins HospitalJasmine ThomasNo ratings yet
- Rev - Final MTDocument177 pagesRev - Final MT89chenweiNo ratings yet
- ESCAP (2009), Medical Travel in Asia and The Pacific. Challenges and OpportunitiesDocument42 pagesESCAP (2009), Medical Travel in Asia and The Pacific. Challenges and OpportunitiesZana Anita0% (1)
- Medical Tourism in ThailandDocument6 pagesMedical Tourism in ThailandJasmine ThomasNo ratings yet
- Factsheet Life Sciences & Health in ThailandDocument4 pagesFactsheet Life Sciences & Health in ThailandElly Nu'ma ZahrotiNo ratings yet
- Health Problems and Health Care Seeking Behavior Among Adult Backpackers While Traveling in ThailandDocument5 pagesHealth Problems and Health Care Seeking Behavior Among Adult Backpackers While Traveling in ThailandodiliaNo ratings yet
- Medical Travellers' Perspective On Factors AffectingDocument17 pagesMedical Travellers' Perspective On Factors AffectingBisma HarjunoNo ratings yet
- Going Global Medical TourismDocument47 pagesGoing Global Medical TourismAhmad SidqiNo ratings yet
- Key Success Factors in Medical Tourism Marketing: Yang, Yung-ShengDocument7 pagesKey Success Factors in Medical Tourism Marketing: Yang, Yung-Shengavijitcu2007No ratings yet
- Medical Tourism Destination SWOT Analysis: A Case Study of Malaysia, Thailand, Singapore and IndiaDocument8 pagesMedical Tourism Destination SWOT Analysis: A Case Study of Malaysia, Thailand, Singapore and IndiaBudi SuhendraNo ratings yet
- A Study of Brand Image, Perceived Service Quality, PatientDocument12 pagesA Study of Brand Image, Perceived Service Quality, PatientNurulfitrahhafidNo ratings yet
- The Changing World of Medical TourismDocument104 pagesThe Changing World of Medical TourismNIMA Chandigarh100% (2)
- 172290-Article Text-441902-1-10-20180530Document16 pages172290-Article Text-441902-1-10-20180530Esther Edor OmoweroNo ratings yet
- Medical Tourism Book Chapter: December 2014Document43 pagesMedical Tourism Book Chapter: December 2014spiridus77No ratings yet
- Medical Travel From North - East India: An Assessment of Domestic Medical Tourists' Travel Profile and ExperienceDocument26 pagesMedical Travel From North - East India: An Assessment of Domestic Medical Tourists' Travel Profile and Experiencevijju006No ratings yet
- Lessons from Indonesia and Malaysia on South-South medical travelDocument15 pagesLessons from Indonesia and Malaysia on South-South medical travelAdji KrisbandonoNo ratings yet
- MEDICAL TOURISM MARKETS AND IMPLICATIONSDocument34 pagesMEDICAL TOURISM MARKETS AND IMPLICATIONSsonali mishraNo ratings yet
- Health Tourism and Challenges For India: Mrs. Christy Solomon Dr. Acharyulu G.V.R.KDocument8 pagesHealth Tourism and Challenges For India: Mrs. Christy Solomon Dr. Acharyulu G.V.R.KRathesh KavanamaniNo ratings yet
- Health Tourism in Asia: The Readiness of Bali'S Health TourismDocument16 pagesHealth Tourism in Asia: The Readiness of Bali'S Health TourismYuni DwitriNo ratings yet
- 01 01 01 IIBAJournal PDFDocument10 pages01 01 01 IIBAJournal PDFmonica_elysabethNo ratings yet
- Seminar - Success Factors of Medical Tourism in AsiaDocument14 pagesSeminar - Success Factors of Medical Tourism in AsiaKong KrcNo ratings yet
- Original Article: Health Tourism in Malaysia: The Strength and WeaknessesDocument9 pagesOriginal Article: Health Tourism in Malaysia: The Strength and Weaknessescotek cunNo ratings yet
- Medical Tourism System ModelDocument35 pagesMedical Tourism System ModelDaniel CookNo ratings yet
- The Health Tourism in South KoreaDocument13 pagesThe Health Tourism in South KoreaGeorge NyongesaNo ratings yet
- MAIN REPORT (PDF)Document54 pagesMAIN REPORT (PDF)Md Mehrab HossainNo ratings yet
- Medical Tourism, The Future of Health Services: DR Christine LeeDocument7 pagesMedical Tourism, The Future of Health Services: DR Christine LeeVinosanth SubramaniamNo ratings yet
- Thailand Medical Hub: Impacts On Thailand Medical Industry: Anongnat Wangwatthaka Thammasat UniversityDocument19 pagesThailand Medical Hub: Impacts On Thailand Medical Industry: Anongnat Wangwatthaka Thammasat UniversityjwangwatthakaNo ratings yet
- HRDJ 3 1 03Document16 pagesHRDJ 3 1 03gimenaNo ratings yet
- HIV/AIDS Prevalence & Sudan's National ResponseDocument3 pagesHIV/AIDS Prevalence & Sudan's National ResponseKaren PearlNo ratings yet
- Medical Tourism FacilitarerDocument9 pagesMedical Tourism FacilitarerRaghu VermaNo ratings yet
- Ranking of Sustainable Medical Tourism Destinations in Iran: An Integrated Approach Using Fuzzy SWARA-PROMETHEEDocument32 pagesRanking of Sustainable Medical Tourism Destinations in Iran: An Integrated Approach Using Fuzzy SWARA-PROMETHEEBolaji OdegbesanNo ratings yet
- COuntry COmparisonDocument8 pagesCOuntry COmparisonDevan GoyalNo ratings yet
- Ijerph 18 09721 v2Document12 pagesIjerph 18 09721 v2Jack FruitNo ratings yet
- Final Draft Medical TourismDocument30 pagesFinal Draft Medical TourismAwol AminNo ratings yet
- Patient Satisfaction and Associated Factors Among Ad - 2021 - International JourDocument6 pagesPatient Satisfaction and Associated Factors Among Ad - 2021 - International JourRonald QuezadaNo ratings yet
- Kuwait: Health Profile 2015Document42 pagesKuwait: Health Profile 2015Fahd AltaweelNo ratings yet
- Seminar ReportDocument66 pagesSeminar ReportAnonymousNo ratings yet
- Thesis On Medical TourismDocument4 pagesThesis On Medical Tourismmelissabuckleyomaha100% (1)
- Medical Tourism in Bali: A Critical Assessment On The Potential and Strategy For Its DevelopmentDocument6 pagesMedical Tourism in Bali: A Critical Assessment On The Potential and Strategy For Its Developmentarif candrautamaNo ratings yet
- Turism MedicalDocument14 pagesTurism MedicalGrigore NicoletaNo ratings yet
- Regional Strategy For TM in Western Pacific 2011-2020Document71 pagesRegional Strategy For TM in Western Pacific 2011-2020Nancy KawilarangNo ratings yet
- Farheen Banu THESIS FinalDocument65 pagesFarheen Banu THESIS FinalAtika FatimaNo ratings yet
- IJTMGH Volume 8 Issue 2 Pages 80-88Document9 pagesIJTMGH Volume 8 Issue 2 Pages 80-88hiromi.iida2525No ratings yet
- India's Medical Tourism IndustryDocument75 pagesIndia's Medical Tourism IndustryDrAmit Sharma100% (1)
- Satisfaction of Nigerian Patients With Health Services: A Protocol For A Systematic ReviewDocument6 pagesSatisfaction of Nigerian Patients With Health Services: A Protocol For A Systematic Reviewsopha seyhaNo ratings yet
- Medical Tourism in IndiaDocument5 pagesMedical Tourism in IndiafrmchnnNo ratings yet
- Preview Art of Stock Investing Indian Stock MarketDocument18 pagesPreview Art of Stock Investing Indian Stock Marketavijitcu2007No ratings yet
- Medical TourismDocument9 pagesMedical TourismSaptarishi ChatterjeeNo ratings yet
- (2014 - 08 - 07 13 - 43 - 57 Utc)Document28 pages(2014 - 08 - 07 13 - 43 - 57 Utc)iccang arsenalNo ratings yet
- Peta Topografi Kabupaten SoppengDocument1 pagePeta Topografi Kabupaten Soppengiccang arsenalNo ratings yet
- Kelley Presentation Medical Tourism PDFDocument23 pagesKelley Presentation Medical Tourism PDFAnandhi RamachandranNo ratings yet
- Patient Safety CultureDocument444 pagesPatient Safety Cultureiccang arsenal100% (3)
- Colour Magazine - London 1Document103 pagesColour Magazine - London 1iccang arsenal100% (1)
- Developing A National Health Financing Strategy - A Reference Guide PDFDocument44 pagesDeveloping A National Health Financing Strategy - A Reference Guide PDFdoctorinth100% (1)
- WV Guidelines enDocument35 pagesWV Guidelines endrkamalakarNo ratings yet
- 2015 Violence PreventionDocument21 pages2015 Violence Preventioniccang arsenalNo ratings yet
- Universal Health Coverage 2Document13 pagesUniversal Health Coverage 2iccang arsenalNo ratings yet
- Uptd Labkesda Dan Elmed KukarDocument1 pageUptd Labkesda Dan Elmed Kukariccang arsenalNo ratings yet
- ED Violence PreventionDocument3 pagesED Violence Preventioniccang arsenalNo ratings yet
- Workplace Violence in Healthcare: Understanding The ChallengeDocument4 pagesWorkplace Violence in Healthcare: Understanding The ChallengeFirman Suryadi RahmanNo ratings yet
- Depth of Knowledge - IccangDocument8 pagesDepth of Knowledge - Iccangiccang arsenalNo ratings yet
- WV Guidelines enDocument18 pagesWV Guidelines eniccang arsenalNo ratings yet
- Preventing Violence in Healthcare FacilitiesDocument27 pagesPreventing Violence in Healthcare Facilitiesiccang arsenalNo ratings yet
- Preventing Violence in Healthcare FacilitiesDocument27 pagesPreventing Violence in Healthcare Facilitiesiccang arsenalNo ratings yet
- WV Guidelines enDocument35 pagesWV Guidelines endrkamalakarNo ratings yet
- Inovasi Layanan - DTPK - Kabid 2018Document20 pagesInovasi Layanan - DTPK - Kabid 2018iccang arsenalNo ratings yet
- TriageDocument101 pagesTriageraighnejames19100% (1)
- World Health Report 2008Document148 pagesWorld Health Report 2008dancutrer2100% (2)
- Rekam Medis Ugd - PuskesmasDocument74 pagesRekam Medis Ugd - Puskesmasiccang arsenalNo ratings yet
- TriageDocument101 pagesTriageraighnejames19100% (1)
- A Mass Casualty Management PDFDocument56 pagesA Mass Casualty Management PDFiccang arsenal100% (1)
- EntrepreneurshipDocument42 pagesEntrepreneurshipiccang arsenalNo ratings yet
- A Mass Casualty Management PDFDocument56 pagesA Mass Casualty Management PDFiccang arsenal100% (1)
- A Mass Casualty ManagementDocument20 pagesA Mass Casualty Managementiccang arsenalNo ratings yet
- PGRS 2014Document165 pagesPGRS 2014Rizky Arifandy75% (8)
- Concept of State and GovernmentDocument35 pagesConcept of State and Governmenticcang arsenalNo ratings yet
- Ebook - Starbucks 1 PDFDocument19 pagesEbook - Starbucks 1 PDFiccang arsenal100% (1)
- Report WritingDocument3 pagesReport WritingRabea ShabbirNo ratings yet
- Statistical Methods SupplemetaryDocument2 pagesStatistical Methods SupplemetaryNavinNo ratings yet
- How Instagram Boosted Cake SalesDocument15 pagesHow Instagram Boosted Cake SalesKang Ato100% (1)
- STARBUCKS CASE STUDY IN MOTIVATION THEORIESDocument6 pagesSTARBUCKS CASE STUDY IN MOTIVATION THEORIESAnê Xuân HươngNo ratings yet
- Diagnostic Lab ServicesDocument19 pagesDiagnostic Lab ServicesNaina Garg100% (3)
- Acupressure On Self-Reported Sleep Quality During Pregnancy: Journal of Acupuncture and Meridian StudiesDocument5 pagesAcupressure On Self-Reported Sleep Quality During Pregnancy: Journal of Acupuncture and Meridian StudiesSofia SagitaNo ratings yet
- Problem Set1-Introductory ConceptsDocument1 pageProblem Set1-Introductory ConceptsJoeyNo ratings yet
- Disi PationDocument23 pagesDisi PationYonymMillaNo ratings yet
- Exercises 3Document20 pagesExercises 3Thành ĐạtNo ratings yet
- Case Study For Contract Management - Hydro Power Projects PDFDocument4 pagesCase Study For Contract Management - Hydro Power Projects PDFpradeepsharma62100% (1)
- Q3 2023 State of Developer NationDocument65 pagesQ3 2023 State of Developer Nationapex9107290No ratings yet
- Social Oriented Quality: From Quality 4.0 Towards Quality 5.0Document8 pagesSocial Oriented Quality: From Quality 4.0 Towards Quality 5.0AngeloNo ratings yet
- Understanding Consumer Behavior and Decision Making in the Hospitality SectorDocument20 pagesUnderstanding Consumer Behavior and Decision Making in the Hospitality SectorPalak ShahNo ratings yet
- Games of Perfect Information, Predatory Pricing and The Chain-Store ParadoxDocument9 pagesGames of Perfect Information, Predatory Pricing and The Chain-Store ParadoxÁlvaro OlórteguiNo ratings yet
- Quantitative Techniques Notes: Measures of Central TendencyDocument89 pagesQuantitative Techniques Notes: Measures of Central TendencyVartika NagarNo ratings yet
- Algebra II Unit 7 StatisticsDocument14 pagesAlgebra II Unit 7 Statisticsapi-287816312No ratings yet
- Curriculum VitaeDocument7 pagesCurriculum VitaeGelo SuacilloNo ratings yet
- An Analysis of Retention Issues in Icici Pru Dr. D. Ranadheer ReddyDocument19 pagesAn Analysis of Retention Issues in Icici Pru Dr. D. Ranadheer ReddySaumyaAcharyaNo ratings yet
- Research Proposal Sample OutlineDocument17 pagesResearch Proposal Sample OutlineGuidance and Counseling OfficeNo ratings yet
- Tips For Writing A Good Reaction PaperDocument7 pagesTips For Writing A Good Reaction PaperL-D Loyd DalanginNo ratings yet
- Motor Development in Children With Autism SpectrumDocument7 pagesMotor Development in Children With Autism SpectrumFlávia AquinoNo ratings yet
- 2-Astm d5298.10910. Suction Measurement-Filter Paper MTD PDFDocument6 pages2-Astm d5298.10910. Suction Measurement-Filter Paper MTD PDFAkshay bvNo ratings yet
- Aligning Goals and Priorities To Manage TimeDocument9 pagesAligning Goals and Priorities To Manage TimeAnurag Sharma100% (1)
- Research and DevDocument14 pagesResearch and DevP NjroNo ratings yet
- Best Practices Volunteer ManagementDocument126 pagesBest Practices Volunteer Managementanitar2010100% (3)
- Comparing Legal SystemsDocument6 pagesComparing Legal SystemsAnastasia KlochkoNo ratings yet
- Template Jurnal Peweka TadulakoDocument3 pagesTemplate Jurnal Peweka TadulakoRizaldy PutraNo ratings yet
- Walking As A Source of Electricity Through The Use of Piezoelectric Plated ShoesDocument5 pagesWalking As A Source of Electricity Through The Use of Piezoelectric Plated ShoesBrave MitraNo ratings yet
- Bibliography Journal On Diabetic FootDocument3 pagesBibliography Journal On Diabetic FootCamille GraceNo ratings yet
- ALARP GuidanceDocument39 pagesALARP Guidancebaaziz2015100% (1)