You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
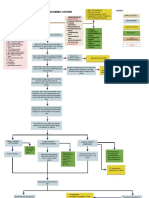
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Emergency TrolleyDocument25 pagesEmergency TrolleyBintang Lenny Sihotang100% (4)
- Pfo IntroDocument9 pagesPfo IntroabdirashidNo ratings yet
- Laparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleDocument4 pagesLaparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleAndrei GheorghitaNo ratings yet
- Anatomy and Physiology of LarynxDocument13 pagesAnatomy and Physiology of LarynxAmin MasromNo ratings yet
- Barret's Syndrome Case ReportDocument3 pagesBarret's Syndrome Case ReportResearch ParkNo ratings yet
- Abnormal Labour and It ManagementDocument27 pagesAbnormal Labour and It ManagementOsama AhmadNo ratings yet
- Trauma 1 ShoulderDocument61 pagesTrauma 1 ShoulderDr Abdallah BahaaNo ratings yet
- Intro ACLS EPDocument46 pagesIntro ACLS EPbrentupdegraff100% (1)
- High Risk Labor and DeliveryDocument5 pagesHigh Risk Labor and DeliveryCarl John ManaloNo ratings yet
- WEEKLY Study Plan DentistryDocument14 pagesWEEKLY Study Plan DentistryWarisha AmirNo ratings yet
- MD MDCG 2019 14 MDR Codes enDocument23 pagesMD MDCG 2019 14 MDR Codes enLeilNo ratings yet
- 5 PDFDocument8 pages5 PDFoskar ORTIZNo ratings yet
- Trigen Húmero + ShureshotDocument56 pagesTrigen Húmero + Shureshotgpe nola jpNo ratings yet
- VAN 201 Introduction To Gross AnatomyDocument3 pagesVAN 201 Introduction To Gross AnatomyOsakuni OlaoluwakitanNo ratings yet
- Anaesthetic Consideration For Neonatal Surgical emDocument7 pagesAnaesthetic Consideration For Neonatal Surgical emLong LongNo ratings yet
- Brachial Plexus InjuryDocument18 pagesBrachial Plexus InjuryZunnoorain RaeNo ratings yet
- Practical Emergency Resuscitation and Critical Care, 2nd Edition (Original PDF From Publisher)Document655 pagesPractical Emergency Resuscitation and Critical Care, 2nd Edition (Original PDF From Publisher)Duk Han KimNo ratings yet
- KN-5T TibiaDocument21 pagesKN-5T TibiaJarinthon Armengot LopezNo ratings yet
- Jadwal Operasi, Rabu 21 Juni 2023Document1 pageJadwal Operasi, Rabu 21 Juni 2023Kevin YonathanNo ratings yet
- Medicalmodsim ResultDocument209 pagesMedicalmodsim ResultNa da NadaNo ratings yet
- 1578.2-GLBL-En Persona Kinematically Aligned TKA SurgTech-digital1Document64 pages1578.2-GLBL-En Persona Kinematically Aligned TKA SurgTech-digital1mamyeu1801No ratings yet
- ECG Workshop 2006Document15 pagesECG Workshop 2006Eggi ErlanggaNo ratings yet
- 4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)Document5 pages4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)SONY MANDAPNo ratings yet
- Urology: Urological Applications Using Bowa Electrosurgical SystemsDocument24 pagesUrology: Urological Applications Using Bowa Electrosurgical SystemsMohamedNo ratings yet
- LSCPR Pals Study Guide 2020Document57 pagesLSCPR Pals Study Guide 2020Juan Ma100% (1)
- Med Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFDocument101 pagesMed Surg Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students Nodrm PDFEya BaldostamonNo ratings yet
- Assessment of Metabolic and Gastrointestinal, Liver AlterationsDocument10 pagesAssessment of Metabolic and Gastrointestinal, Liver AlterationsGel JamsNo ratings yet
- Development of Body CavitiesDocument20 pagesDevelopment of Body CavitiesFaith ChepoghishoNo ratings yet
- Abdomen OSPE Charts Questions OnlyDocument29 pagesAbdomen OSPE Charts Questions OnlyRathnaNo ratings yet