You might also like
- Vitamin D effects on healthDocument5 pagesVitamin D effects on healththarhanNo ratings yet
- Apem 20 198Document8 pagesApem 20 198Sari MustikaNo ratings yet
- Association Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysisDocument9 pagesAssociation Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysiswatiNo ratings yet
- Risk Factors of Vitamin D Deficiency in Children With Epilepsy Taking Anticonvulsants at Initial and During Follow-UpDocument12 pagesRisk Factors of Vitamin D Deficiency in Children With Epilepsy Taking Anticonvulsants at Initial and During Follow-UpSari MustikaNo ratings yet
- Can Vitamin D Status Be Assessed by Serum 25OHD in Children2015Document7 pagesCan Vitamin D Status Be Assessed by Serum 25OHD in Children2015Sheyla Alegre ParionaNo ratings yet
- Association Between Vitamin D Status and Undernutrition Indices in Children - A Systematic Review and Meta-Analysis of Observational StudiesDocument9 pagesAssociation Between Vitamin D Status and Undernutrition Indices in Children - A Systematic Review and Meta-Analysis of Observational StudiesAnggie DiniayuningrumNo ratings yet
- 9.endo Wilsford2013Document5 pages9.endo Wilsford2013faithlophpeace21No ratings yet
- v8 I92920jmscr PDFDocument6 pagesv8 I92920jmscr PDFGilbert SimamoraNo ratings yet
- DR - Sazzad JRNL-3Document32 pagesDR - Sazzad JRNL-3Dr SazzadNo ratings yet
- Jurnal Vit DDocument5 pagesJurnal Vit Dida ayu agung WijayantiNo ratings yet
- Wang 2015Document10 pagesWang 2015Andana TrisaviNo ratings yet
- Zhang 2014Document8 pagesZhang 2014darius2311No ratings yet
- Makalah TerbaruDocument8 pagesMakalah Terbaruq9tt4ftcxnNo ratings yet
- Anak Jurnal 2Document6 pagesAnak Jurnal 2Muhammad HidayatNo ratings yet
- Vitamin D de Ficiency in Critically Ill Children: AuthorsDocument8 pagesVitamin D de Ficiency in Critically Ill Children: AuthorsArdi PratamaNo ratings yet
- Ijcp-5470 oDocument6 pagesIjcp-5470 oDrkaleembrimsNo ratings yet
- Ijmb 22 71Document4 pagesIjmb 22 71Research OfficeNo ratings yet
- Vitamin D and AutisimDocument12 pagesVitamin D and AutisimAbditsion DhiisaniiNo ratings yet
- A Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsDocument5 pagesA Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsRatnaNo ratings yet
- Vitamin D and bone health in Indian childrenDocument6 pagesVitamin D and bone health in Indian childrenTerri PerryNo ratings yet
- Vitamin D Intake and Risk of Cardiovascular Disease in US Men and WomenDocument9 pagesVitamin D Intake and Risk of Cardiovascular Disease in US Men and WomenAgafioNo ratings yet
- Investigacion CanadaDocument9 pagesInvestigacion CanadaAgustín CerraNo ratings yet
- Vitamin D For Postmenopausal WomenDocument2 pagesVitamin D For Postmenopausal Womensoos.edinaNo ratings yet
- Prevalence of Vitamin D Deficiency and Associated Risk Factors in The US Population (2011-2012)Document10 pagesPrevalence of Vitamin D Deficiency and Associated Risk Factors in The US Population (2011-2012)Mahida El shafiNo ratings yet
- Prenatal Vitamin D Status and Offsprings Growth Adiposity and Metabolic Health A Systematic Review and Meta AnalysisDocument10 pagesPrenatal Vitamin D Status and Offsprings Growth Adiposity and Metabolic Health A Systematic Review and Meta Analysismisslcassidy2No ratings yet
- High-dose vitamin D3 supplementation in pregnancy and risk of neurodevelopmental disorders in the children at age 10_ A randomized clinical trialDocument9 pagesHigh-dose vitamin D3 supplementation in pregnancy and risk of neurodevelopmental disorders in the children at age 10_ A randomized clinical trialFransiska FranshuidNo ratings yet
- Relationship Between Serum Vitamin D Level and Ectopic Pregnancy: A Case-Control StudyDocument6 pagesRelationship Between Serum Vitamin D Level and Ectopic Pregnancy: A Case-Control StudyMatias Alarcon ValdesNo ratings yet
- Outcome of Calcium & Vit D Level in Premenopausal Female Visiting Teaching HospitalDocument4 pagesOutcome of Calcium & Vit D Level in Premenopausal Female Visiting Teaching HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Artikel 2Document7 pagesArtikel 2Claudia BuheliNo ratings yet
- Vit D Dan Faktor Resiko EpilepsiDocument9 pagesVit D Dan Faktor Resiko Epilepsieronika sasongkoNo ratings yet
- Vitamin D Birth Cohort StudyDocument9 pagesVitamin D Birth Cohort StudyRita ChatrinNo ratings yet
- Nutrients 07 03427Document22 pagesNutrients 07 03427Nurfadhilah YusufNo ratings yet
- Vitamin D Deficiency and Metabolic Syndrome in Ukrainian AdolescentsDocument8 pagesVitamin D Deficiency and Metabolic Syndrome in Ukrainian Adolescentstrisna amijayaNo ratings yet
- Vitamin D and Ocular InflammationDocument5 pagesVitamin D and Ocular InflammationRIYA PARVEENNo ratings yet
- Vitamin D and Metabolic Disturbances in Polycystic Ovary Syndrome (PCOS) - A Cross - Sectional StudyDocument13 pagesVitamin D and Metabolic Disturbances in Polycystic Ovary Syndrome (PCOS) - A Cross - Sectional StudyAmarendra WardhanaNo ratings yet
- Pone 0058725Document13 pagesPone 0058725HS SarohaNo ratings yet
- Research ArticleDocument5 pagesResearch ArticleiwanNo ratings yet
- Jop 2014 130686Document12 pagesJop 2014 130686Karen HoffmanNo ratings yet
- Iron and Vitamin D Deficiency in Healthy Young Children in Western Europe Despite Current Nutritional RecommendationsDocument8 pagesIron and Vitamin D Deficiency in Healthy Young Children in Western Europe Despite Current Nutritional RecommendationsJeff Willian Rosas QuinaNo ratings yet
- Low Vitamin D Levels Are Associated With Atopic Dermatitis, But Not Allergic Rhinitis, Asthma, or Ige Sensitization, in The Adult Korean PopulationDocument15 pagesLow Vitamin D Levels Are Associated With Atopic Dermatitis, But Not Allergic Rhinitis, Asthma, or Ige Sensitization, in The Adult Korean PopulationJundi Agung SamjayaNo ratings yet
- s 1368980016000173 ADocument8 pagess 1368980016000173 Atihemex618No ratings yet
- 1 FullDocument13 pages1 FullAdina MicuNo ratings yet
- Pubmed 18088161Document5 pagesPubmed 18088161DomenicaNo ratings yet
- Vitamin DStatus in Early ChildhoodDocument9 pagesVitamin DStatus in Early ChildhoodSulingallo JeinzenNo ratings yet
- Sharifi2019 PDFDocument7 pagesSharifi2019 PDFmoussaouiNo ratings yet
- Reduced Serum Concentrations of 25-Hydroxy Vitamin D in Children With Autism: Relation To AutoimmunityDocument7 pagesReduced Serum Concentrations of 25-Hydroxy Vitamin D in Children With Autism: Relation To AutoimmunityAchmad YunusNo ratings yet
- Correlation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaDocument4 pagesCorrelation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaOmWawanNo ratings yet
- Study of Prevalence of Vitamin D Deficiency in Nephrotic SyndromeDocument7 pagesStudy of Prevalence of Vitamin D Deficiency in Nephrotic SyndromeDrShibsankar PalNo ratings yet
- Vitamin D Insufficiency Linked To Asthma Severity: Medscape Medical NewsDocument6 pagesVitamin D Insufficiency Linked To Asthma Severity: Medscape Medical NewsMichal MajewskiNo ratings yet
- Vit D Deficiency Cin Obesity Meta-AnalysisDocument7 pagesVit D Deficiency Cin Obesity Meta-AnalysisJade IreneNo ratings yet
- Vitamin D Levels in Children Diagnosed With Acute Otitis MediaDocument5 pagesVitamin D Levels in Children Diagnosed With Acute Otitis MediamuthiafadhilahNo ratings yet
- Associations Between Vitamin D Levels and Depressive SymptomsDocument6 pagesAssociations Between Vitamin D Levels and Depressive SymptomsRafifa AmruNo ratings yet
- The Effect of Vitamin D Supplementation On Depressive Symptoms in Adults A Systematic Review and Meta Analysis of Randomized Controlled TrialsDocument19 pagesThe Effect of Vitamin D Supplementation On Depressive Symptoms in Adults A Systematic Review and Meta Analysis of Randomized Controlled TrialsEmillya SariNo ratings yet
- Hipovitaminoza DDocument29 pagesHipovitaminoza DekatarinaNo ratings yet
- Relation of Body Fat Indexes To Vitamin D Status and Deficiency Among Obese AdolescentsDocument9 pagesRelation of Body Fat Indexes To Vitamin D Status and Deficiency Among Obese AdolescentsJill R SendowNo ratings yet
- Vitamin D Levels May Impact IVF Success Rates Differently by RaceDocument7 pagesVitamin D Levels May Impact IVF Success Rates Differently by RaceMohamed AliNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)From EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)No ratings yet
- Board Review in Preventive Medicine and Public HealthFrom EverandBoard Review in Preventive Medicine and Public HealthRating: 3.5 out of 5 stars3.5/5 (2)
- 06 Combination Therapy in Epilepsy PDFDocument5 pages06 Combination Therapy in Epilepsy PDFTariq AbdoNo ratings yet
- Respiratory InfectionDocument15 pagesRespiratory InfectionRatnaNo ratings yet
- Dengue TropMed New Sept'12Document62 pagesDengue TropMed New Sept'12RatnaNo ratings yet
- Sepsis 2013Document42 pagesSepsis 2013RatnaNo ratings yet
- Pengaruh Suplementasi Seng Dan Zat BesiDocument8 pagesPengaruh Suplementasi Seng Dan Zat BesiRatnaNo ratings yet
- The Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734Document4 pagesThe Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734RatnaNo ratings yet
- Perawatan Luka Diabetes Mellitus Menggunakan Teknik Modern Dressing Alberikus Dimantika, Sugiyarto, Yuyun SetyoriniDocument13 pagesPerawatan Luka Diabetes Mellitus Menggunakan Teknik Modern Dressing Alberikus Dimantika, Sugiyarto, Yuyun SetyoriniNita ZahriNo ratings yet
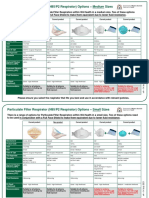
- Respirator Comparison TDBDocument4 pagesRespirator Comparison TDBalopezvillavicencioNo ratings yet
- Fistula Kista Duktus Tiroglosus: Laporan KasusDocument6 pagesFistula Kista Duktus Tiroglosus: Laporan KasusRatnaNo ratings yet
- Protokol Apnea AiimsDocument16 pagesProtokol Apnea AiimsAlessandro AlfieriNo ratings yet
- COVID19 N95 and P2 Respirator OptionsDocument2 pagesCOVID19 N95 and P2 Respirator OptionsRatnaNo ratings yet
- AnemiaDocument3 pagesAnemiaRatnaNo ratings yet
- Nutricia Global Virtual Conference: Impacting Health in The New Norm With Specialized NutritionDocument9 pagesNutricia Global Virtual Conference: Impacting Health in The New Norm With Specialized NutritionRatnaNo ratings yet
- Growth FalteringDocument56 pagesGrowth FalteringRatnaNo ratings yet
- Emergency Care Issues in HemophiliaDocument14 pagesEmergency Care Issues in Hemophiliamuhammad gagas sasongkoNo ratings yet
- Approach To Liver Function Tests in Children: Mahmood HaghighatDocument4 pagesApproach To Liver Function Tests in Children: Mahmood HaghighatRatnaNo ratings yet
- The Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734Document4 pagesThe Association of Antiepileptic Drugs With Vitamin D Status in Childhood Epilepsy December 2019 1576325924 5710734RatnaNo ratings yet
- 3887-Article Text-17080-1-2-20191014Document10 pages3887-Article Text-17080-1-2-20191014RatnaNo ratings yet
- Nelson MCQ PDFDocument595 pagesNelson MCQ PDFPavan Kumar100% (5)
- Emergency Care Issues in HemophiliaDocument14 pagesEmergency Care Issues in Hemophiliamuhammad gagas sasongkoNo ratings yet
- A Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsDocument5 pagesA Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsRatnaNo ratings yet
- Growing PainDocument7 pagesGrowing PainRatnaNo ratings yet
- Chromosome 22q11.2 Deletion PDFDocument14 pagesChromosome 22q11.2 Deletion PDFRatnaNo ratings yet
- Vitamind Supplementation Among Children With EpilepsyDocument4 pagesVitamind Supplementation Among Children With EpilepsyRatnaNo ratings yet
- Vit D and As ValproatDocument4 pagesVit D and As ValproatRatnaNo ratings yet
- Pedsql Module CardioDocument31 pagesPedsql Module CardioRatna100% (1)
- 52 HypoglycemiaDocument2 pages52 HypoglycemiaphobicmdNo ratings yet
- Study of Vitamin D Levels in Epileptic Children in Age Group of 2-16 YearsDocument2 pagesStudy of Vitamin D Levels in Epileptic Children in Age Group of 2-16 YearsRatnaNo ratings yet
- Dating Questions and AnswersDocument13 pagesDating Questions and AnswersFelicia Babrant98% (49)
- Euphoria Special Edition Rue ScriptDocument24 pagesEuphoria Special Edition Rue ScriptMoldovan EdithNo ratings yet
- Engineering A New Mouse Model For Vitiligo 2012 Journal of Investigative DermatologyDocument4 pagesEngineering A New Mouse Model For Vitiligo 2012 Journal of Investigative DermatologyAurelian Corneliu MoraruNo ratings yet
- TDS - Rheofinish 288 FDDocument2 pagesTDS - Rheofinish 288 FDVenkata RaoNo ratings yet
- Observation of Unknown SpectrumDocument3 pagesObservation of Unknown SpectrumOmar HusseinNo ratings yet
- Sea Cliff Zanzibar E Fact SheetDocument6 pagesSea Cliff Zanzibar E Fact SheetBenedict MuringakumweNo ratings yet
- 10 DNA Testing Myths Busted, and Other Favorite Posts: by Blaine T. BettingerDocument11 pages10 DNA Testing Myths Busted, and Other Favorite Posts: by Blaine T. BettingerSexy888No ratings yet
- Caterpillar C18 ACERTDocument2 pagesCaterpillar C18 ACERTMauricio Gomes de Barros60% (5)
- UG TRB Physical Education Study MaterialDocument17 pagesUG TRB Physical Education Study Materialசண்முக சுந்தரம் குருசாமி100% (2)
- Smoke & Ventilation CalculationsDocument7 pagesSmoke & Ventilation CalculationsZine ModelsNo ratings yet
- Respiratory Care Anatomy and Physiology 3rd Edition Will Beachey Test BankDocument12 pagesRespiratory Care Anatomy and Physiology 3rd Edition Will Beachey Test BankOcean0% (1)
- Predictor PlatesDocument40 pagesPredictor PlatesrambabuNo ratings yet
- National Ehealth: "Moving Towards Efficient Healthcare"Document30 pagesNational Ehealth: "Moving Towards Efficient Healthcare"nurul fatma diyanaNo ratings yet
- BurgerKing Versus McDonaldsDocument4 pagesBurgerKing Versus McDonaldsmarkus johannessenNo ratings yet
- BS 1290-1983 Wire Rope Sling PDFDocument20 pagesBS 1290-1983 Wire Rope Sling PDFmithilesh100% (2)
- Fbioe 09 624021Document28 pagesFbioe 09 624021Davide Di ZioNo ratings yet
- Cariology-9. SubstrateDocument64 pagesCariology-9. SubstrateVincent De AsisNo ratings yet
- Perlos HistoryDocument21 pagesPerlos HistoryRiyali TardyNo ratings yet
- Self-Confidence and Satisfaction Among Nursing Students With The Use of High Fidelity Simulation at Arab American University, PalestineDocument10 pagesSelf-Confidence and Satisfaction Among Nursing Students With The Use of High Fidelity Simulation at Arab American University, PalestineArianna Jasmine MabungaNo ratings yet
- Goat anatomy and physiology guideDocument8 pagesGoat anatomy and physiology guideLochi GmNo ratings yet
- HDFC Life InsuranceDocument12 pagesHDFC Life Insurancesaswat mohantyNo ratings yet
- SX SeriesDocument6 pagesSX SeriesmattuttezNo ratings yet
- Census of India 2011 Village and Town Level Data for Purba Champaran District, BiharDocument368 pagesCensus of India 2011 Village and Town Level Data for Purba Champaran District, BiharRahul SharmaNo ratings yet
- The Maharashtra Shops and Establishments (Regulation of Employment and Conditions of Service) Rules, 2018Document2 pagesThe Maharashtra Shops and Establishments (Regulation of Employment and Conditions of Service) Rules, 2018Gopinath hNo ratings yet
- Steam Blowing - Disturbance Factor Discusstion2 PDFDocument5 pagesSteam Blowing - Disturbance Factor Discusstion2 PDFchem_taNo ratings yet
- Appliance DocumentationDocument44 pagesAppliance DocumentationВадим КрасноперовNo ratings yet
- The Scientific Facts About WaterDocument7 pagesThe Scientific Facts About WaterNizam HasniNo ratings yet
- Water Hardness Case StudyDocument15 pagesWater Hardness Case StudyTaima GhNo ratings yet
- CPC Sample Exam 1Document9 pagesCPC Sample Exam 1Renika_r80% (5)
- Phytochemical Analysis of Plant of Cissus QuadrangularisDocument7 pagesPhytochemical Analysis of Plant of Cissus QuadrangularisIJRASETPublicationsNo ratings yet