Professional Documents
Culture Documents
Insect Bites
Uploaded by
zeniafadilaOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Insect Bites
Uploaded by
zeniafadilaCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/304954037
Insect bite infestations
Chapter · December 2011
CITATIONS READS
0 5,270
4 authors, including:
Rama Jayaraj Shelley F Walton
Charles Darwin University University of the Sunshine Coast
104 PUBLICATIONS 393 CITATIONS 181 PUBLICATIONS 3,096 CITATIONS
SEE PROFILE SEE PROFILE
Some of the authors of this publication are also working on these related projects:
Scabies Diagnosis: Development of Sero-Diagnostic Test View project
Genetic Diversity Analysis of Goat Breeds based on Microsatellite Polymorphism View project
All content following this page was uploaded by Rama Jayaraj on 10 August 2016.
The user has requested enhancement of the downloaded file.
Chapter 21
Insect Bite Infestations
Rama Jayaraj, PhD* • Shelley F. Walton, PhD† •
Deborah C. Holt, PhD‡ • Kabir Sardana, MD, DNB, MNAMS§
SCABIES by direct, close contact with an infected person,
although transmission by fomites is possible.
Scabies is an ectoparasitic skin disease caused by the
burrowing itch mite Sarcoptes scabiei var hominis. CLINICAL FEATURES Patients of all ages may
be afflicted. However, children are commonly
affected. It occurs equally in both sexes. The clinical
AETIOLOGY The major factors that contrib-
features are as follows:
ute to the spread of scabies are poverty and over-
crowded living conditions. In developed countries, • Generalised pruritis occurs which is often more severe
outbreaks of scabies commonly occur in hospitals, at night.
kindergartens and old age facilities. • Papular or vesicular lesions are seen in the vicinity of
The female Sarcoptes mites burrow into the burrows which in some cases become pustular or bul-
stratum corneum and lay two to three eggs per lous (Fig. 21.1).
day, for up to 6 weeks at a time, resulting in raised
papules on the skin surface. The female mite does
not penetrate deeper than the S. granulosum. The
developmental stages of the mite include egg, larva,
protonymph and tritonymph. Adult mites emerge
after approximately 2 weeks. The average burden
on a normal host is 10–12 mites.
Some authors have reported fluctuations of
scabies every 7 years (scabies is also termed ‘7-year
itch’). Some studies have suggested that there is a
higher incidence during the winter months as colder
weather encourages overcrowding in human beings.
The mites might also be sensitive to antimicrobial
peptides in human sweat, leading to reduced infes-
tation in summer.
Crusted scabies is a more severe form of infes-
tation and is also known as Norwegian scabies. It
occurs in the immunocompromised patients (HIV Figure 21.1 The interdigital area is dominated by linear
infected, especially), those with decreased sensory papules and burrows and because of
function (e.g. people with leprosy), and institu- constant scratching, the classic burrow is
tionalised patients. Transmission of scabies occurs rarely seen.
* Lecturer, Tropical and Emerging Infectious Disease Division, Menzies School of Health Research and School of Environmental and Life
Sciences, Charles Darwin University, Darwin, Australia.
†Associate Professor, School of Health and Sport Sciences, University of the Sunshine Coast, Sippy Downs, Queensland, Australia.
‡Senior Research Officer, Skin Pathogens Research Laboratory, Menzies School of Health Research, Institute of Advanced Studies,
Charles Darwin University, Darwin, Australia.
§Associate Professor, Department of Dermatology and Nodal Officer STD (Regional STD Centre), Maulana Azad Medical College and
Lok Nayak Hospital, New Delhi, India.
M21_WK_XXXXX_C21.indd 500 12/18/11 12:05 PM
Insect Bite Infestations 501
Figure 21.4 Secondary infection and eczematisation
Figure 21.2 Urticarial lesions on the abdomen. superimposed on the classic findings of
scabies.
• Generalised itchy papular eruption/skin rash is com-
monly seen around the axillae, the peri-areolar regions,
abdomen, buttocks and thighs (Fig. 21.2). and the penis in males and the peri-areolar region
• Symptoms in children follow a pattern similar to that in females (Figs 21.1–21.3).
in adults. However, the face, neck, scalp, palm/soles • Chronic excoriation and eczematisation
(Fig. 21.3) and the post-auricular folds are more often (Fig. 21.4) of the skin is frequently observed in
involved in children. patients with long-standing infestations.
• The majority of the patients complain of an
Clinical Types intense itch, especially at night and after a hot
shower. This has been associated with a hypersen-
1. Ordinary scabies
sitivity reaction to the excreta that the mite depos-
• Ordinary lesions of scabies are seen in the webs
its within the burrow.
of the fingers, the volar aspects of the wrists and
2. Norwegian or crusted scabies
arms, the extensor aspect of the elbow, periumbili-
• This can be attributed to immunosuppression
cal skin, pelvic girdle including buttocks, ankles
(such as topical or systemic glucocorticoid ther-
apy, HIV, human T-lymphotropic virus 1 (HTLV-
1) infection, organ transplant patients), mentally
retarded and physically incapacitated patients.
• Hyperkeratotic skin crusts are either loose, scaly
and flaky, or thick and adherent.
• The lesions of this severe form (Fig. 21.5)
can either be distributed all over the body or
(Fig. 21.5) localised in the neck, scalp, face, eye-
lids, legs, feet and the area under the nails.
• Mites are commonly found beneath the nails of
affected patients, and in crusted scabies, this can
result in thickened dystrophic nails. In ordinary
scabies, the distal ends of nails may harbor scabies
mites, where they are protected from topical treat-
ment. However, in crusted scabies, larger popula-
tions of mites may cause subungual hyperkeratosis
and longitudinal splitting of the nail. Untreated
Figure 21.3 Papules on the palm. nails can act as a reservoir of infection, resulting
M21_WK_XXXXX_C21.indd 501 12/18/11 12:05 PM
502 Insect Bite Infestations
Figure 21.5 A case of Norweigian scabies with
erythroderma and involvement of the web
space of the hand. (Courtesy: Dr. Chander
Grover Kubba )
in treatment failure with recurrence of symptoms Figure 21.6 Scabeitic nodules on the scrotum.
months later.
• Generalised adenopathy and eosinophilia are
present in some cases.
DIAGNOSIS
• Due to an altered immune response in immuno- Laboratory and Special Examination Microscopic
compromised subjects, the itching is less intense identification of mites, mite parts, eggs, egg shell
or absent in these subset of patients. This occurs fragments or faecal pellets of mites from skin
also because they have physical limitations, lack of scrapings, is confirmatory for diagnosis (Fig. 21.9);
control or unawareness of the defensive scratch- however, the sensitivity of this test is less than 50%.
ing movements, as in neuropsychiatric disorders,
The diagnosis becomes difficult in patients who have
osteoarticular deformities, muscular atrophy or
other neuromuscular problems. Sometimes, it is
associated with loss of sensation and hypoesthe-
sia. These patients are highly infested with mites.
3. Nodular scabies
• Violaceous, pruritic, nodules are seen on the
glans, scrotum, thighs, buttocks and axilla
(Figs 21.6 and 21.7). Mites cannot be recovered
from these nodules.
• It is believed that this represents a form of hyper-
sensitivity reaction to mite antigens.
4. Vesicular–bullous scabies
• It is commonly seen in elderly patients and is located
on the extremities or on the trunk (Fig. 21.8).
• It clinically and histologically mimics bullous
pemphigoid.
• It may result from super infection with Staphylo-
coccus aureus, with a mechanism similar to the
development of blisters in bullous impetigo.
• This condition is mainly due to the penetration
of the mite in the dermo-epidermal junction, or
a cross-reaction with bullous pemphigoid antigen
or lytic secretions produced by the mite at the der-
moepidermal junction. Figure 21.7 Multiple nodules with eczematisation on the
5. Other minor variants: These are discussed in Table 21.1. scrotum.
M21_WK_XXXXX_C21.indd 502 12/22/11 1:21 PM
Insect Bite Infestations 503
Figure 21.9 Examination of skin scrapings from patients
Figure 21.8 Bullous lesions with crusted papules. of scabies and the observation of mites
under the microscope (40×).
severe hypersensitivity reactions that result in the examination of the patient’s skin, from the surface
development of multiple excoriations or plaques. to the superficial papillary dermis. This equipment
In this situation, a biopsy or the examination of is expensive and is available only in well-resourced
scrapings obtained from the papules–vesicles may hospitals or clinics.
be helpful. The burrows may be demonstrated in The latest test is the detection of the DNA of
these cases with the help of stains such as India ink S. scabiei from cutaneous scales based on ampli-
or gentian violet. fication by polymerase chain reaction (PCR)
Epiluminescence microscopy and high- or detection by enzyme-linked immunosorbent
resolution video dermatoscopy allow comprehensive assay.
Table 21.1 Minor Variants of Scabies
Types Clinical features Comments
Scabies incognito • This is consequent to topical application of • Hypereosinophilia in the presence of
corticosteroids. It is less itchy mild reduction of immunity
Scabies in infants and • Vesicles, pustules and nodules • A dense Langerhans cell infiltrate may
young children • Sites: hands, feet and body folds be present in histological sections
Scabies in elderly • Senile itch or bullous lesione • Frequently misdiagnosed
Scabies of the scalp • Seen in elderly, children, infants,
immunosuppressed patients and patients with
crusted scabies
Subungual scabies • Persistent nail plate dystrophy. The nails may have • Cutting of the nails prevents both the
a thickened, whitened appearance with or without condition and the relapse
nail plate deformity and/or subungual horny debris
Canine scabies • Site: Forearms, thighs, chest and abdomen • The pet is easily recognised because
• Onset: Within 24–96 h after contact with the it presents with patches of hair loss
infected pet and/or scratching. Treatment of the
• Course: Self-limited, lasting an average of 5–13 wk dog is required
M21_WK_XXXXX_C21.indd 503 12/18/11 12:06 PM
504 Insect Bite Infestations
TREATMENT The treatment options can be 2. Permethrin: This is a pyrethroid component and is a
classified according to the evidence-based approach highly efficacious topical scabicide. Five per cent per-
as follows: methrin is applied overnight once a week for 2 weeks,
over the entire body from neck downwards. Although
1. Randomised controlled trials: These are available for permethrin is the most expensive of all the topical
comparison between the effects of the following drugs: applications, it has almost no allergic side effects. The
• Ivermectin versus benzyl benzoate recommended period of contact with permethrin is
• Ivermectin versus permethrin about 8 hours. A case report of the treatment of 467
• Ivermectin versus benzyl benzoate patients in an outbreak of scabies cited that a single
• Permethrin versus crotamiton application of 5% permethrin was as effective as 1%
2. Case series: These are available for the following lindane. A second application is necessary 1 week
therapies: later only if there is clear evidence of treatment fail-
• Benzyl benzoate ure. However, Walton and colleagues (1999, 2004)
• Permethrin have demonstrated growing concerns about resis-
• Ivermectin tance to permethrin in Australia. It is often used in
• Permethrin versus lindane pregnant women, and the application time is short-
3. Case reports: These are available for the following ened to 2 hours and it is also widely used in young
therapies: children (greater than 2 months). At present, despite
• Pimecrolimus the limitations of small trials, a dearth of placebo-
• Monosulfiram controlled trials, and some conflicting information;
the first-line treatment for uncomplicated scabies
General Measures Washing bed linens and cloth- continues to be 5% permethrin.
ing is highly recommended. This can be performed 3. Lindane (γ-hexachlorcyclohexane): It is available
by machine washing at 60°C followed by heat dry- as 1% cream or lotion, and its application time is
ing. Unwashed clothes can be stored in a bag for a approximately 6 hours. It is also recommended that
minimum of 3 days as mites do not survive for more the application be repeated after 1 week. A single,
6-hour application is effective in the treatment of sca-
than a few days after isolation from human host.
bies. Although it is a cost-effective topical scabicide,
Exposing mattresses to direct sunlight can also be a it can cause severe skin irritation, allergic contact der-
useful technique. Vacuuming is also beneficial. matitis and neurological symptoms such as insomnia,
irritability, vertigo, convulsions, vomiting, diarrhoea,
Drugs Used in the Treatment of Scabies The restlessness and collapse. As a result, the use of this
major factors that determine the suitability of dif- drug has been prohibited in the European Union since
ferent scabicidal drugs for patients are the age of the 2001. It is banned in children younger than 3 years
patient, presence of pregnancy and lactative stage of due its toxicity and increasing resistance.
women, efficacy of the drugs, degree of eczematisa- 4. Crotamiton: It is widely prescribed for newborn
babies. For the treatment of scabies in children
tion and the cost involved.
between 2 months and 5 years of age, 5% perme-
1. Benzyl benzoate: The treatment of thousands of thrin was compared with 10% crotamiton cream in a
cases of scabies with topical benzyl benzoate was randomised trial. Two weeks after a single overnight
documented in Denmark during the 1930s; 10–25% treatment, 30% and 13% of children were cured with
benzyl benzoate applied in the form of a cream or permethrin and crotamiton respectively, and 4 weeks
lotion is highly efficient. Benzyl benzoate requires fre- after treatment, 89% and 60% of patients respectively,
quent applications such as twice daily for 2–3 days were cured. This indicates that crotamiton may not be
and needs to be repeated after 10 days. Benzyl ben- as efficacious as permethrin. It should be applied twice
zoate is very effective when used correctly. If not, it a day for five consecutive days, and the contact period
may cause skin irritation and or a burning sensation has to be 48 hours. It has an additional antipruritic
particularly with the 25% lotion. If the skin irritation effect but may cause erythema and conjunctivitis.
is severe, the benzyl benzoate should be washed off. 5. Sulphur: Sulphur can be used as an ointment in a
It may cause irritant dermatitis on the face and scro- concentration between 2% and 10%, and most
tum. The use of analgesia and antihistamines is often commonly, the 6% formulation is used. Sulphur is
advisable before the application. A trial found that highly recommended in that subset of patients who
48% patients treated with topical benzyl benzoate cannot tolerate lindane, permethrin or ivermectin,
were cured as compared with 70% of patients treated though it is substandard to all these agents in efficacy.
with oral ivermectin. The ointment is applied to the entire surface of the
M21_WK_XXXXX_C21.indd 504 12/18/11 12:06 PM
Insect Bite Infestations 505
body on two to three consecutive nights. It is cheap further studies need to be performed to prove both
and is a safe choice for the treatment of scabies in the efficacy and safety.
infants, children and pregnant women. Sulphur has
an unpleasant smell and can cause staining of clothes.
In addition, in some cases it may have irritant effects
Drug Resistance Resistance to lindane, permeth-
and variable absorption may result in side effects in rin and crotamiton treatment has been observed.
the kidney. In El Salvador, Peru, Panama, New Zealand, Egypt
6. Monosulfiram: It is used in an emulsion form which and United States, resistance to lindane has been
is applied all over the body after a bath. It is recom- recorded. In vitro evidence of resistance to permeth-
mended that this should be applied once a day on two rin was reported in recurrent crusted scabies. A recent
or three consecutive days. The use of alcohol should study highlighted the in vitro tolerance of Sarcoptes
be strictly avoided during treatment to avoid severe scabiei mites to ivermectin in scabies-endemic com-
reactions. munities. In such circumstances, a cocktail of lindane
7. Malathion: This is an organophosphate insecticide
and benzyl benzoate or permethrin can be used.
which is not currently recommended for the treat-
ment of scabies due to its severe adverse effects.
8. Pimecrolimus: It is a class of immunomodulatory Type-Specific Treatment The basic principles of
drugs and a recent report suggests that it appears to treatment of scabies include the establishment of a
be effective in the treatment of eczema on keratinised diagnosis of scabies and the decision regarding a
skin. A case report highlights that nodular scabies suitable medication. If the treatment is topical, the
treated with topical pimecrolimus showed a marked
whole body should be treated, from the neck to the
improvement after therapy.
9. Ivermectin (systemic): It is used as a treatment of
toes in adults and including the head and face in
choice for a large number of endoparasites (nema- babies. It is also necessary to treat all the direct
todes) and ectoparasites (insects, Sarcoptes scabiei contacts of the case. Follow-up of treated cases
[0.2 mg/kg in a single dose], Pediculus humanus, should be carried out at 1 and 4 weeks after scabi-
Demodex folliculorum and Cheyletiella spp.). Mul- cidal treatment. In addition to scabicidal treatment,
tiple doses are used repeatedly for the treatment of antipruritic agents such as antihistamines may be
Norwegian scabies (200 μg/kg along with kerato- necessary to alleviate itching. Furthermore, suitable
lytics), and in immunocompromised patients. More antibiotics can be used if secondary bacterial infec-
than 98% of the oral dose of ivermectin is excreted tion is present.
in the faeces and it is also metabolised in the liver.
A study conducted on 1153 scabies infested prison- 1. Crusted scabies: Most cases of Norwegian scabies
ers revealed that a single dose of ivermectin cured need to be admitted to the hospital for treatment.
88% of recipients after 4 weeks and showed 95.5% Multiple doses of oral ivermectin may be required in
efficacy after 8 weeks. Some trials highlighted that a addition to topical agents which should be applied all
single dose of 200 μg/kg of oral ivermectin is as effec- over the body. A cure is generally attained after three
tive as traditional topical applications such as benzyl consecutive treatments with topical applications.
benzoate, lindane and permethrin for the treatment However, in some cases, additional treatments such
of ordinary scabies. It is likely a second dose after 1 as keratolytics (5–10% salicylic acid in petrolatum)
week may be required in many patients. The adverse will be required to increase the penetration of scabi-
effects may include anorexia, asthenia, headache, cides. Decayed nails should be trimmed and brushed
arthralgia, myalgias, fever, eosinophilia and macu- with a scabicidal agent. Ten per cent precipitated sul-
lopapular rashes. Due to the limited data on safety, phur in petrolatum is more reliable than permethrin
ivermectin should not be used in children weighing in this setting. Oral ivermectin can be used alone, but
<15kg or during pregnancy or lactation. One study is more effective when used in combination with topi-
suggested a possible neurotoxicity in the elderly. The cal treatment.
resistance of scabies mites to ivermectin has been 2. Scabies in children: A total of 2–10% sulphur in pet-
reported in two cases. rolatum can be used in infants and 5% permethrin
10. Ivermectin (Topical): It has been tested in a few open cream can be used in infants older than 2 months.
label studies; in the most recent one, two applications Crotamiton is also recommended for use in babies
of 1% ivermectin (400 μg/kg per dose) in a solution and toddlers. In infants, the use of ivermectin and lin-
of propylene glycol, spaced 1 week apart, had 100% dane are not advisable. A case report demonstrated
success in treating scabies in adults and children that when oral ivermectin was used in combination
as young as 1 year old with no side effects. Again, with lindane and keratolytics, an 11-year-old girl
M21_WK_XXXXX_C21.indd 505 12/18/11 12:06 PM
506 Insect Bite Infestations
with crusted scabies was cured without any side are because of reinfection from untreated con-
effects. A 12.5% benzyl benzoate emulsion can also tacts. It has also been suggested that pruritus can
be used in children. temporarily worsen after treatment secondary to
3. Scabies in pregnant and lactating women: Six per cent the massive death of mites and the release of their
sulphur precipitate/crotamiton are the drugs of choice
toxic products.
in pregnant women and lactating women. Use of iver-
mectin, permethrin (category B) and lindane should
be avoided. SUMMARY OF THERAPY IN SCABIES The
4. Nodular scabies: The use of a scabicide followed by summary of evidence-based treatment is given in
intra-lesional steroids is recommended for the treat- Figure 21.10. Some general treatment tips are given
ment of nodular scabies. Corticosteroids can be rec- in Box 21.1.
ommended if the nodules persist after repeated treat-
ment. A recent report demonstrated that nodular
scabies was cured by topical pimecrolimus.
Treatment of Persistent Symptoms It is normal PEDICULOSIS
for patients to experience persistence of symptoms
for 2–6 weeks after successful treatment because There are two species of lice that can infect
of the immune response against the mite antigens. humans—P. humanus humanus and P. humanus
If the symptoms persist beyond 2 weeks, it could capitis. Only the body louse is capable of trans-
be because of an incorrect initial diagnosis, incor- mitting the disease-endemic typhus (Rickettsia
rect application of treatment and poor penetra- prowazekii), trench fever (Bartonella quintana) and
tion of treatment through thick scales, reinfection relapsing fever (Borrelia recurrentis, Borrelia dut-
or drug-resistant mites. Most cases of recurrence toni). P. capitis is not a known vector for disease.
First line
Topical antiscabietic agents
• Permethrin$
Oral antiscabetic agent
• Benzyl benzoate$
• Ivermectin^
• Lindane$
• Sulphur$
• Crotamiton$
• Monosulfiram+
Second line
Pimecrolimus+ (nodular scabies)
Supportive therapy
• Keratolytics
• Antipruritics
• Antibiotics (infection)
Figure 21.10 Evidence-based treatment of scabies.
^Randomised controlled trials.
$Case series/retrospective studies.
+Case reports/small case series.
M21_WK_XXXXX_C21.indd 506 12/18/11 12:06 PM
Insect Bite Infestations 507
BOX 21.1 Treatment Tips
• Ensure that the cream is applied to the whole body,
specifically on the scalp (children) and under the free
edges of nails.
• As fomites can play a role, the laundering of sheets and
clothing also helps.
• Close physical contact with the infested patients
spreads the disease. It is estimated that 15–20 minutes
of close contact with an infected patient is enough to
transfer the mites from one person to another.
• People that are reinfected are at risk of cumulative
drug toxicity.
• Clothes and bed linens can be machine washed at 60°C
followed by heat drying. If washing is not possible,
they should be isolated in a bag for at least 3 days.
• In the setting of crusted scabies, the use of insecticidal
powders or aerosols may be considered for materials
that cannot be washed.
Figure 21.11 Multiple nits are seen on the scalp.
Extreme pruritus is the primary character- CLINICAL FEATURES
istic of pediculosis. This is a manifestation of the Symptoms One of the first indications of infesta-
immune response and it takes 4–6 weeks for the tion is intense itching. Pruritus indicates an infesta-
pruritus to develop in a non-sensitised individual tion of about 2 months’ duration.
and only 24–48 hours in case of repeat exposure.
Rarely, children may be totally asymptomatic.
Examination The lice are difficult to be seen in
clean individuals. Yet, they can be abundant and
PEDICULOSIS CAPITIS are easily seen in malnourished individuals and in
those with poor hygiene (Fig. 21.11). Head lice
The head louse is responsible for spreading the can be identified with the naked eye or with a
disease and can be a cause of social stigma, and hand lens but are difficult to find. The majority
be embarrassing and uncomfortable. Head lice, of patients have a population of 10 head lice. Nits
paradoxically, prefer to infest a clean healthy are firmly cemented to the hairs; vary in number
head and will leave a host if the conditions are from only a few to thousands. Nits are deposited
not optimal. Straight hair is more vulnerable than by the head lice on the hair shaft as it emerges
curly hair. from the follicle.
LIFE CYCLE DIFFERENTIAL DIAGNOSIS Nits can be con-
• The incubation period from the time of exposure to fused with dandruff. The flakes of dandruff fall eas-
the development of pruritus is approximately 30 days. ily from the hair whereas nits are firmly attached
• The ova (nits), hatch in approximately 7–9 days and to it. Pseudonits are bits of desquamated epithe-
mature in another week. lium which encircle the hair but are more readily
• The ova are laid very close to the scalp and hatch removed than true nits.
before the hair grows more than 1/4 inch. Thus, if no
nits are found within 1/2 inch of the scalp and no lice
are seen, treatment is not necessary. COMPLICATIONS
• As nits can live for 10 days, and nymph and adult 1. Eczema and lichen simplex chronicus: These occur
lice for 3 days away from human host, head lice may on the occipital part of the scalp and over the
be transmitted by both direct contact and by fomites neck secondary to chronic scratching and rubbing
(combs, brushes, hats, helmets). (Fig. 21.12).
M21_WK_XXXXX_C21.indd 507 12/18/11 12:06 PM
508 Insect Bite Infestations
DIAGNOSIS The gold standard for diagnosis is
direct identification of a live louse (nits are within
1 cm of head). In tropical countries like India,
viable nits may be located greater than 1 cm from
the scalp. A microscopic examination of the nit is
necessary to see whether the egg case is empty or
viable. Areas that provide a higher yield for screen-
ing include the nape of the neck and that behind
the ears.
In a recent study it was found that the louse
comb method was found to be four times more effi-
cient and twice as fast, as direct visual examination,
in the diagnosis of P. capitis infestations.
TREATMENT
Topical Therapy Permethrin and malathion are
effective in the treatment of head lice, whereas syn-
ergised pyrethrins are slightly less effective. A recent
Figure 21.12 Secondary infection with crusting on the study found that out of five head lice treatments
scalp with eczematisation on the neck used in vitro against lice that had previous exposure
(plica polonica). to permethrin and pyrethrins, 0.5% malathion was
the most effective pediculicide and ovicide, killing
2. Excoriations, crusts and secondarily impetiginisation all the lice and eggs within 10 minutes. Also effec-
(Figs 21.12 and 21.13): These lesions are seen com- tive was 1% permethrin, which killed all lice in
monly on the neck, forehead, face and ears. In the
about an hour. The ovicidal activity of permethrin
extreme cases, the hair over the entire scalp becomes
a confluent, purulent mass of matted hair, lice, nits,
was 73% in its diluted form and 90% in its non-
crusts and purulent discharge, so-called plica polon- diluted form, demonstrating that permethrin should
ica. This can result in alopecia (Fig. 21.13) be used on dry hair. One per cent lindane was found
to be the slowest-acting pediculicide and the least
effective ovicide.
Systemic Therapy
Ivermectin The drug is pediculicidal, but only
when the lice takes a blood meal. Apart from the
standard dose (Table 21.2) of ivermectin, three
doses of 12 mg given every 7 days, has also been
used to eradicate body lice in the homeless adult
population in France. It is not approved by FDA for
patients with a weight under 15 kg.
A recent study (Chosidow et al., 2010) has
found that for difficult-to-treat cases of infestation
with head-lice infestation, oral ivermectin, given
twice at a 7-day interval, had superior efficacy as
compared with topical 0.5% malathion lotion, a
finding that suggests that it could be an alternative
treatment.
Figure 21.13 Scalp shows areas of hair loss due to Trimethoprim-Sulfamethoxazole It works by
secondary infection. killing bacterial flora necessary for the synthesis of
M21_WK_XXXXX_C21.indd 508 12/18/11 12:06 PM
Insect Bite Infestations 509
Table 21.2 Therapy of Louse Infestation*
Agent Application Comments
• Permethrin cream, 1% (age • Applied for 10 min and then rinsed off • It has low toxicity, is cosmetically
>2 mo; pregnancy B) well. One single application is sufficient acceptable
although it can be repeated in 10 days
to treat the viable ova that may have
hatched since the initial application
• Lindane 1% (pregnancy C) • Applied to dry hair, left on for 4 min • Excessive application induces resistance
and rinsed. No re-treatment needed and/or toxicity, especially if it is applied
after a warm bath which favours its
absorption. Toxicity may include local
irritation
• Malathion 0.5% lotion (age • Apply to dry hair, leave on 8–12 h, rinse; • Not available in India
>6 yr; pregnancy B) repeat in 7–9 d
Ivermectin • 200 μg/kg/dose; repeat in 7–10 d —
• Off-label for scabies, head lice
• Prescription (pregnancy C)
*Dimethicone has been launched in India.
B vitamins in the louse. There are two combinations CONCLUSION The best treatment depends on
proposed for the use of this oral drug. local patterns of resistance. Due to the absence
of these data in India, we rely on western data.
• Combination of 1% permethrin cream and oral TMP
(10 mg/kg/d based on TMP for 10 days in two divided
Resistance can increase if the same formulation
doses) has been used for an extended period of time.
• Combination of 1% lindane shampoo plus oral TMP Resistance has been reported to occur with per-
(8 mg/kg/d based on TMP for 12 days in two divided methrin, synergised pyrethrins and lindane. Most
doses) treatment failures can be attributed to poor tech-
nique, non-compliance or reinfection. As there is
Further studies need to be performed to fully evalu- no product that kills 100% of the eggs; all patients
ate the role of oral TMP as an adjunctive treatment. should be retreated in 1 week’s time to eradicate
Use of louse repellants is another approach to the mature eggs.
minimise infestation. Piperonal is twice as effec- Although the American Academy of Pediat-
tive as DEET (N,N-diethyl-m-toluamide) in a body rics prefers malathion, a European study favours
louse model. Slow-release citronella has some effect the use of oral ivermectin over malathion. In India,
but may cause scalp irritation. in the absence of malathion, ivermectin is a good
The search for newer drugs has focused on option; though it is not FDA approved less than
newer, non-toxic methods of intervention such as 15 kg. Although transmission from fomites has not
5% benzyl alcohol, 4% dimethicone lotion and suf- been proven, it is still recommended to wash, dry
focants. Recently spinosad has been approval for clean, vacuum or isolate (in a sealed plastic bag for
use in patients greater than 4 years of age. 2 weeks) items such as hats, combs, brushes and
linens.
Future Therapies The newer therapies target In Table 21.2, we have excluded pyrethrins as
components of the nit sheath, which is an insolu- they are not available in India. The current recom-
ble polymer that acts as a glue to attach the egg mendations for treatment in order of decreasing
case to the hair shaft. Potential therapeutic agents, efficacy include (i) permethrin 1% cream followed
including proteases, denaturants, β-sheet breaker by (ii) lindane 1%, (iii) pyrethrins with piperonyl
proteins and small protein inhibitors of sheath butoxide and (iv) malathion 0.5%. Dimethicone is
formation. a safer but probably less efficacious options.
M21_WK_XXXXX_C21.indd 509 12/18/11 12:06 PM
510 Insect Bite Infestations
• As with pediculosis capitis, the symptoms begin only
First line after several weeks of infestation or sooner, in cases of
reinfestation.
• Pruritis is the main symptom, although in cases with
• Malathion 0.5%*,^ secondary infection, there may also be pain, fever, mal-
• Permethrin 1%†,^ aise and lymphadenopathy.
• Carbaryl 0.5%$
TREATMENT Body lice are treated by the
improvement of hygiene and laundering (heat to a
Second line temperature of 65ºC for 15–30 minutes), discard-
ing, or applying insecticides to clothing. In severe
infestations, topical pediculicides can also be used.
• Crotomiton 10%$
It should be emphasised that though there is no evi-
• Occlusive therapy (dimethicone^, dence for the use of topical agents for body louse,
cetaphil cleanser$, petroleum most clinicians prescribe pediculicides (Fig. 21.15)
jelly+) Box 21.2.
• Home remedies (vinegar, olive
oil, melted butter)+
PEDICULOSIS PUBIS (PUBIC LICE)
The crab or pubic louse (P. pubis), which usually
Third line inhabits the genital region, is short (1–2 mm) and
broad, and the first pair of legs is shorter than
the claw-like second and third pairs. Infestation
• Lindane 1%^ may occur in other areas including the moustache,
• Oral ivermectin$ beard, axillae, chest and even scalp hair. They are
• TMP/SMX, Levamisole$
seen in STD patients and more commonly in homo-
• Head shaving+
sexual men.
Figure 21.14 Evidence-based management of P. capitis.
LIFE CYCLE/TRANSMISSION Crab lice usually
^ Randomised controlled trials.
lay only three eggs per day. Adult lice can live off
$ Retrospective study/large case series. the host for up to 36 hours and the viable eggs, for
+ Small case series/case reports. 10 days. Eggs continue to hatch for 1 week after
* It is the preferred first line as it is shown to reduce the resistance.
treatment. The chances of acquiring pediculosis
† In India in the absence of malathion, permethrin is the preferred
line of therapy.
General measures
An evidence-based management of P. capitis is • Laundering (>60°C—10 min)
depicted in Figure 21.14. • Seal mattress for 3 wk
Insecticidal agents
PEDICULOSIS CORPORIS Topical agents
The adult body louse (Pediculosis humanis) lives on • Malathion 0.5%, carbaryl 0.5%, permethrin 5%+
and lay eggs in clothing and not directly on the human Systemic agents
skin. Body lice are most often found in the homeless, • Oral ivermectin+
refugees, beggars and in people staying in generally
unsanitary and/or crowded living conditions.
CLINICAL FEATURES Figure 21.15 Evidence-based management of P. corporis.
• Papular lesions, scabs, urticaria and excoriations are
usually seen. + Small case series/case reports.
M21_WK_XXXXX_C21.indd 510 12/19/11 12:40 PM
Insect Bite Infestations 511
BOX 21.2 General Measures for Treatment of Pediculosis
First line
1. The presence of dead organisms on the scalp/body
is an issue that is rarely addressed. The only certain
way to remove dead nits is with a fine-toothed comb • Malathion 0.5%+
or a forceps. Pediculicides have varying ovicidal • Permethrin 1%$
activity, and eggs attached to hair shafts require • Carbaryl 0.5%+
7–10 d to hatch. Thus, a second application is
needed after this interval only if the living lice can be
demonstrated or eggs are observed. Combs and Second line
brushes should be soaked in 2% Lysol or a
pediculicidal shampoo for approximately 1 h or
heated in water for 5–10 min.
2. For treatment of pediculosis corporis, the patient • Lindane 1%$
needs to wash with soap and water and apply topical • Oral ivermectin+
antipruritic lotions. If lice are present on the body, • TMP/SMX, Levamisole+
pediculicides should be used. Lice residing in clothing
may be killed by washing the clothes and/or dried by Figure 21.16 Evidence-based management of P. pubis.
machine (hot cycle in each); by boiling, followed by
$ Retrospective
ironing the seams; by dry-cleaning; or by the study/large case series.
+ Small case series/case reports.
application of dry heat at 60ºC for 20 min.
3. Products with an oil base (vaseline, olive oil,
mayonnaise and margarine) may smother the adult
lice, but have no effect on the nits. Vinegar or TREATMENT The body and axillary hair as well
formic acid has been reported to remove the glue as the eyelashes and beard should also be examined
that holds the nit firmly to the hair shaft. Alcohol, for nits; the scalp may rarely be involved. Shaving
kerosene and paint thinners have also been used of the pubic area should be discouraged because fol-
but carry extreme risks. liculitis and irritation may develop.
The treatment recommended for pediculosis
pubis includes (i) permethrin 1% cream applied for
10 minutes and then washed off; (ii) lindane 1%
pubis from one sexual exposure with an infected applied for 4 minutes and then washed; and (iii)
person are approximately 95%. The transmission pyrethrins with piperonyl butoxide applied for 10
of crab lice can occur without body contact, espe- minutes and then washed off.
cially in warm environments. Lindane should not be used in pregnant
women or children younger than 2 years of age, In
CLINICAL FEATURES Pubic lice cause severe addition, bedding and clothing should be decon-
pruritus that is difficult to ignore. Examination of taminated (machine washed/dried with high heat);
the patient reveals the presence of black powder- sexual partners in the last month should be treated;
like louse faeces as well as lice firmly adherent to and patients should be examined for the presence
hair in the pubic and abdominal areas. Small blue- of other STDs.
black dots caused by the irritating secretion of the Summary of treatment for P. pubis is depicted
lice’s bite (macula cerulea) are characteristically in Figure 21.16.
seen on the lower abdomen and thighs.
COMPLICATIONS These include secondary bac-
PHTHIRIASIS PALPEBRARUM
terial infections and lymphadenopathy. Most therapies for this disease are based on case
reports. No clinical trials have been performed to
DIFFERENTIAL DIAGNOSIS The yellow-grey help delineate the best treatment for phthiriasis
adult louse may be difficult to find and are usually palpebrarum (Fig. 21.17). The various treatments
located at the base of the hairs, resembling small include mechanical removal; maximal trimming of
freckles, scabs or moles. the eyelashes; or topical applications of occlusive
M21_WK_XXXXX_C21.indd 511 12/18/11 12:06 PM
512 Insect Bite Infestations
4. After a further period of exposure, the delayed reac-
First line tion no longer occurs, and eventually there is no reac-
tion at all. The patient is then said to be immune.
• Petroleum jelly+
• Mechanical removal+ AETIOLOGY Fleas (dog or cat), mosquitoes,
• Physostigmine 0.25%/1%+ bedbugs, lice, scabies or mites (fowl, grain, grass)
can be implicated in most cases. In India, the most
common cause is mosquito bite. While cimicosis
Second line (bed bugs) is discussed later in the chapter the other
causes are enumerated in Table 21.3.
• Cryotherapy+ CLINICAL FEATURES Papular urticaria is
• Yellow oxide of mercury+ described as an urticarial wheal reaction followed
• Oral TMP/SMX, teracycline+
by the development of a firm pruritic papule, which
usually persists for several days. The wheal and
Figure 21.17 Evidence-based management papule may show a central haemorrhagic punctum,
of P. palpebrarum. and the papule may be surmounted by a tiny vesicle.
+ Small
Lesions are often grouped in clusters, and develop
case series/case reports.
in crops at irregular intervals (Fig. 21.18).
The number and distribution of skin lesions
ointments (e.g., petrolatum or precipitated sulfur- produced by the bites depends upon the type of
based ointments) used twice daily for 7–10 days, exposure and the feeding habits of the arthropod
4% pilocarpine nitrate twice daily for 4 days, anti- involved. New bites by an arthropod of the same
cholinesterase eye ointments, 1% yellow oxide of species often cause recrudescence of activity in
mercury (applied for a few minutes before washing existing lesions.
off) twice daily for 14 days, permethrin cream, or Bullous reactions (Fig. 21.19) are common on
20% fluorescein. the lower legs but may occur at other sites, especially
in children. In cases with venous hypertension in the
INSECT BITES HYPERSENSITIVITY
REACTION (PAPULAR URTICARIA)
Papular urticaria is a common sequelae which
occurs because of injection of pharmacologically
active substances, and partly because of sensitisa-
tion to injected antigens. The type of reaction in an
individual patient provoked by an arthropod bite
or sting largely depends on previous exposure to
the same or related species. The sequence of events
which determine this was described initially by Mel-
lanby (1944, 1946) and is as follows:
1. In the first instance of exposure, there is commonly
no reaction.
2. After repeated bites, sensitivity begins to develop,
which manifests as an itchy papule that develops
about 24 hours after each bite and persists for several
days. Figure 21.18 Urticarial wheal with a central vesicle and
3. With prolonged exposure, there is an immediate wheal a crusted lesions which corresponds to the
reaction followed by the delayed papular reaction. morphology of popular urticaria.
M21_WK_XXXXX_C21.indd 512 12/18/11 12:06 PM
Insect Bite Infestations 513
Table 21.3 Other Common Insect Bite/Infestations
Species Example Clinical features
Hymenoptera • Bees, wasps and ants • Mild: Mild wheal and flare reactions with
variable oedema persisting <24 h
• Systemic reactions: Vomiting, diarrhoea,
generalised oedema, dyspnoea,
hypotension and collapse. Rarely, it can be
life-threatening
• Delayed allergic reactions: They occur within
hours to 2 wk following the sting and
have symptoms similar to those of serum
sickness with urticaria accompanied by
lymphadenopathy and polyarthritis
Diptera (flies) • Botfly (Dermatobia hominis) can cause myiasis • Most commonly there is immediate pruritic
• Simulium or black fly (Onchocercosis) wheals followed by itchy, red papules
• Sand fly carries Leishmaniasis • Myiasis: There is a painful furuncle that
occurs when a fly deposits parasitic larvae on
human skin
• Onchocerciasis: Facial oedema, subcutaneous
nodules and iritis
Siphonaptera (fleas) • Human flea (Pulex irritans) • These bites are typically evident as grouped
• Oriental rat flea (Xenopsylla cheopis) which urticaria papules, some with a central
carries Yersinia pestis (plague) and Rickettsia punctum
typhi (endemic typhus)
Mites • Cheyletiella mites (walking dandruff ) • They cause pruritic dermatitis in humans
who handle pets
• House mouse mite • It can cause an extremely pruritic papular
bites
• Scabies mite (Sarcoptes scabei) • Already discussed
• The red mite (Chigger or Trombiculidae) • Chiggers can transmit scrub typhus
(Rickettsia tsutsugamushi), leaving a black
eschar at the bite site, pneumonitis and
constitutional symptoms
• Demodex folliculorum
Ticks • They are found in trees, grass, bushes or on • Tick bites are painless and are recognised
animals (dogs, cattle). After attaching itself later on when there is itching or when
to the human skin, the female tick feeds, the engorged tick is found. Other features
becomes engorged after 7–14 d, and then that can be seen include urticaria, eschar
drops off formation and granulomatous reaction to
insect bites
• Minor or major constitutional symptoms
can be associated with early stages of
Lyme disease. Multiple symptoms can
accompany both the early-disseminated
disease and late-stage disease, depending
on which system is involved (CNS, cardiac or
musculoskeletal). Very rarely, children can
develop a reversible flaccid paralysis that
starts after the tick has been attached for
several days
M21_WK_XXXXX_C21.indd 513 12/18/11 12:06 PM
514 Insect Bite Infestations
tion is severe, there may be fever and malaise.
Secondary infection is a common complication, and
may manifest as impetigo, folliculitis, cellulitis or
lymphangitis. A mnemonic ‘SCRATCH’, has been
used to describe the clinical features (Table 21.4).
Major Clinical Points
1. Children aged 18 months to 10 years are typically
affected
2. One child in the family may be the only person bitten
3. Common in spring or summer
4. May occur anywhere on the body, but typically on
exposed skin
5. Erythematous pruritic papule
6. May be grouped in clusters; where the insect has bit-
ten the patient several times, it looks like ‘breakfast,
lunch and dinner’ (Fig. 21.21)
7. Occasional vesicles or bullae, especially in young
children
8. Some immunosuppressed children or those with HIV
infections can have severe exaggerated reactions
9. Recurrent crops are common
Figure 21.19 Bullous eruption due to insect bite reaction.
COURSE The lesions tend to start after infancy,
and an affected child usually ‘grows out’ of the
lower limbs, haemorrhagic or ulcerated lesions may
problem in a few years, even if the source of the
develop. Severe local changes are sometimes found,
bites is not dealt with. Individual lesions last for 1
with the development of cellulitis and lymphangitis
or 2 weeks and recur in distinct crops, especially in
in the apparent absence of secondary infection.
the summer and hence the lay term ‘heat bumps’.
Irritation is an almost inevitable symptom, and
The lesions disappear with any change of environ-
rubbing and scratching may increase the inflamma-
ment, for example, by going on a holiday. Surpris-
tory changes and induce eczematisation (Fig. 21.20).
ingly, often only one member of a family is affected,
When there are numerous bites, or if the local reac-
perhaps because the others have developed immu-
nological tolerance after repeated bites.
MOSQUITO BITES
Allergic reactions to mosquito bites occur due to sen-
sitisation to mosquito salivary proteins. Mosquito
saliva-specific immunoglobulin IgE, IgG antibodies
and T-cell-mediated delayed type hypersensitivity
reaction appear to be involved in the pathogenesis.
Culex quinquefasciatus, Aedes aegypti and Aedes
vexans are the three most important species of mos-
quitoes worldwide.
A recent study found that mosquito bites were
more commonly seen in females and 50% of cases
had a personal history of atopy. The average age of
Figure 21.20 Eczematous reaction which in Indian onset of this reaction was 5.7 years (range 2–58)
skin causes post-inflammatory and the patients were desensitised by an average of
hyperpigmentation. 9.5 years of age.
M21_WK_XXXXX_C21.indd 514 12/18/11 12:06 PM
Insect Bite Infestations 515
Table 21.4 Clinical Features of Papular Urticaria (SCRATCH)
Abbreviation Description Comments
S • Symmetrical distribution (scalp, neck, • Diaper area is spared
face, torso, extremities) • Trunk is rarely involved with bites along the socks line,
waistline or other sites where clothing is occlusive.
C • Crops/clusters of different colouration • Lesions usually appear in a ‘meal cluster’, sometimes
(Fig. 21.22) (erythema, hypo-/hyper- described as ‘breakfast, lunch and dinner’. These linear
pigmentation) or triangular groupings of lesions are characteristic of
bedbug bites; however, they may also be seen in flea bites
R • Rover not required: pets are not • There is a remote history of exposure to cat fleas,
necessary criteria for diagnosis. In fact, mosquitoes, bedbugs and any stay in hotels which has to
a history of exposure to pets often be elicited
cannot be elicited from the patient
A • Age specific (usually occurring between • Tolerance develops in most children by 10 years of age
2 and 10 yr of age)
T • Target lesions and time (may take weeks • Prevention of secondary infection with appropriate
to years to resolve). It is a chronic hygiene of the nails and hands and the use of moisturisers
condition and takes time to resolve is perhaps the BEST intervention
C • Confused paediatrician/parent: ‘We • It is important but difficult to make the parents appreciate
don’t have fleas!’ that the condition is because of insect bites and it requires
observation and patience for resolution
H • Household with single family member • Since this condition is due to hypersensitivity, some
affected individuals, by definition, will react while others will not
CLINICAL FEATURES The reaction to mosquito Other uncommon reaction include anaphy-
bites is determined by previous exposure, and the lactic reactions, serum sickness-like illness, bullae,
sequence of events following multiple bites was elu-
cidated by Mellanby (1944, 1946)
• Stage 1 (induction of hypersensitivity): In an individual
not previously exposed, the bites produce no response.
• Stage 2 (delayed skin reactions): With subsequent
bites, a delayed reaction occurs (pruritic wheals) which
develop approximately 24 hours after the bites and
persist for several days.
• Stage 3 (immediate skin reactions and delayed reactions):
After repeated bites for several weeks, the response
changes, with the appearance of an immediate wheal at
the bite site. This resolves after about 12 hours, to be
replaced by the delayed reaction. (papule).
• Stage 4 (immediate reactions): Further exposure provokes
the immediate reaction, but not the delayed response.
• Stage 5 (no reaction): Eventually, tolerance is acquired,
and no reaction occurs.
Thus, with time there is no response to the bite. This
sequence of events explains the lack of symptoms in
adults and elder sibling of the affected child. Also,
it gives an idea of the acquisition of immunological Figure 21.21 Clustered papules the so-called ‘breakfast,
tolerance in the child with age. lunch and dinner’.
M21_WK_XXXXX_C21.indd 515 12/18/11 12:06 PM
516 Insect Bite Infestations
of the mosquito to track the vapour trail of carbon
dioxide exhaled by a human. Nets and clothing
treated with repellents not only prevent mosquitoes
from biting through clothes but also from biting the
adjacent areas. Repellents may remain effective for
several days on fabric.
If bedbugs exist in the home, measures such as
laundering the bedding and mattress pads every 2–4
weeks in combination with applying double-sided
tape to the legs of the bed have been shown to pre-
Figure 21.22 Polymorphic presentation on the limbs vent bedbugs from becoming long-term residents in
with papules, central punctum, excoriated
their common dwelling places.
lesions and pigmentation. The associated
hyper/hypopigmentation makes it a
cosmetically inelegant presentation. USE OF INSECT REPELLENTS Although DEET
is recommended (diethyltoluamide [DEET]) as it
works against mosquitoes, flies, fleas, mites and
cellulitis, ecchymosis, urticaria, angioedema and ticks, it is not widely available in India. It should
eczematisation. Exaggerated hypersensitivity be noted that the OTC products in the Indian mar-
responses to mosquito bites have been seen in cases ket contain N,N-diethyl benzamide and not DEET.
of chronic lymphatic leukaemia and HIV infection. However, permethrin is a good alternative and
There have been reports of development of works as an insecticide and repellent against lice,
malignant histiocytosis, but this has only been ticks, fleas, mites, mosquitoes and black flies. The
observed in Japan. The triad is constituted by other agents that have been recommended include
hypersensitivity to mosquito bites, chronic Epstein– ethyl hexanediol, dimethyl phthalate and dimethyl
Barr virus infection and natural killer cell leukae- carbate butopyronoxyl. It should be noted that
mia/lymphoma. sweating reduces the effect of all repellents. The
following repellents are safe for application on the
MANAGEMENT OF INSECT BITE REACTIONS skin: DEET, picaridin, MGK-326, MGK-264, IR
AND IBIH (PAPULAR URTICARIA)
3535 and botanical oils (citronella, lemon oil, euca-
lyptus, geranium).
PREVENTION It is a useful measure to explain Insect repellents containing DEET in a concen-
the importance of this as it is easier to prevent than tration of 10% or less may be applied to clothing or
to treat insect bite reactions especially insect bite- skin (caution should be exercised as it can be neuro-
induced hypersensitivity (IBIH). This includes wear- toxic). Special fabrics impregnated with acaricides
ing of protective clothing for outdoor play with the are available. No product will protect against spi-
judicious use of insect repellents. Families with pets ders, wasps or bees.
should participate in aggressive measures for flea-
control (flea collars, flea medication, frequent bath- TREATMENT
ing of the dog/cat and frequent washing of personal General Measures Parents should be advised of
bedding in hot water). Patients should be asked to the frustrating, persistent, recurrent nature of IBIH
avoid attractants such as perfumes, scented prepa- and reassured by the eventual development of toler-
rations; brightly coloured clothing or jewellery; ance and resolution of symptoms. They should be
and wool, suede or leather apparel. Factors that made to understand the natural history of IBIH in
attract mosquitoes to skin include warmth, sweat, order to prevent multiple consultations and inva-
moisture, carbon dioxide and other body secretions sive, unnecessary investigative studies.
found in the convective air currents above or down-
wind of humans. Mosquito repellents do not mask
these attractive stimuli but form a barrier against Active Therapy (IBIH/Mosquito Bites) Pruritic
penetration that extends to a distance of less than lesions can be individually treated with a topi-
4 cm away from the skin. DEET blocks the ability cal steroid (low to medium strength) two to three
M21_WK_XXXXX_C21.indd 516 12/18/11 12:06 PM
Insect Bite Infestations 517
times a day. Oral antihistamines (diphenhydramine,
First line
hydroxyzine) may help reduce itching. Topical cro-
tamiton is a useful adjunct to therapy. Although it
does not have evidence topical benzoyl peroxide is
• Elimination+
effective in resolution of mosquito bite reactions • Antihistaminics
(personal experience). A summary of the evidence- • Topical steroids, topical
based therapy for IBIH (papular urticaria) is given (calamine, camphor/menthol)+
in Figure 21.23. • Crotomiton+
Active Therapy (Other Insect Bites) Insects
should be flicked or brushed (not squeezed) off the Second line
skin in a way that the venom sac is also removed.
The removal of the stinger with a forceps is not
recommended as it may squeeze the attached
• I/L steroids, oral steroids+
venom sac. • Insect repellants+
The administration of cold packs, systemic
antihistamines and a topical steroid may be useful
for the control of pruritus and inflammation associ-
ated with local reactions. Third line
A summary of the evidence-based therapy for
insect bites is provided in Figure 21.24.
• Phototherapy, cyclosporin+
Treatment of Anaphylaxis
1. A total of 0.3–0.5 mg epinephrine HCl (0.3–0.5
mL of a 1:1000 dilution) should be injected IM and Figure 21.23 Evidence-based approach to papular
repeated after15–30 minutes, as needed. Lower doses urticaria (IBIH).
should be used in the elderly and in patients with car-
diovascular problems. + Small case series/case reports.
• Elimination of insects
• Use of repellants (DEET, permethrin)
• Botanicals oils+
Prevention • Fleas (lufenuron, fipronil, Imidacloprid)^
• Topical steroids, camphor, menthol, lidocane
Active
therapy+
Figure 21.24 Summary of preventive and therapeutic measures for insect bites.
^ Randomised controlled trials.
+ Small case series/case reports.
M21_WK_XXXXX_C21.indd 517 12/18/11 12:06 PM
518 Insect Bite Infestations
2. In severe anaphylaxis with hypotension and poor parasite in the faeces of the host. On humid soil or
peripheral circulation, epinephrine should be admin- sand, they hatch giving rise to rhabditiform larva
istered intravenously in a dilution of 1:10,000 (1 mg = which form filariform larva which penetrate unpro-
10 mL) in a bolus dose of 0.1 mg until symptoms tected skin. Through the circulatory system, the lar-
improve. An intravenous line should be started. If the
vae lodge in the small intestine. Eggs, as well as the
patient does not respond to initial measures, critical
care referral is essential. These measures include the
larvae, can be transported by flies, increasing their
administration of oxygen, intravenous aminophylline dissemination. The human skin can be penetrated
and inhaled bronchodilators. by mud, dirt or, especially, sand. They are capable
3. Antihistamines should be administered as an adjunct of invading the skin through follicular pores or
to epinephrine because their effect is not immediate. sweat glands where they could remain for a long
4. Steroids have a delayed onset of action and are not time and lead to folliculitis. Usually, they migrate
the first-line drugs for treating a severe systemic reac- through the epidermis at speeds that vary from a
tion. However, unless medically contraindicated, few millimetres to centimetres per day. Rarely, they
they should be used to prevent continued reaction in may also penetrate the dermis.
all but the mildest allergic reactions. The treatment
should begin with 100 mg of hydrocortisone given IV
every 6 hours and the patient should be discharged on CLINICAL FEATURES
a dose of 30 mg of prednisone per day, tapering over 1. Larva migrans caused by Uncinaria: Skin penetration
3–7 days as symptoms dictate. is usually asymptomatic. The infestation presents
5. Immunotherapy with insect venom is effective and with the formation of a pruritic papule associated
should be considered mandatory for patients who with an erythematous track that follows an erratic
have had an immediate systemic reaction to an insect course. This lesion is usually intensely pruritic,
sting. Commercial venoms and fire ant extract can be and it can cause burning or pain (Fig. 21.25). The
used for diagnosis (skin testing) and desensitisation. most commonly involved areas are the soles, hands,
Adults with a previous systemic reaction to a sting gluteus and back.
and a positive venom test will have a similar reaction 2. Larva migrans caused by Gnathostoma (Gnathostomi-
in approximately 50% of instances if stung again. asis): The clinical manifestations vary depending on the
After immunotherapy, a re-sting will elicit a systemic organ involved; the digestive and genitourinary tract,
reaction in less than 5% of patients. kidney, lungs, brain, eyes and ears may be affected.
Skin is the most frequently involved organ and the easi-
est to detect and present in the following forms:
MISCELLANEOUS CONDITIONS
LARVA MIGRANS
(LARVA MIGRANS SYNDROME)
Larva migrans or creeping eruption is an infestation
of the skin by the nematode larvae. These worms
normally parasitise the intestine of other animal
species. The nematode cannot complete its life cycle
in man. As the worm migrates in the epidermis, it
produces a characteristic lesion.
AETIOLOGY/LIFE CYCLE The following types
of worms can cause cutaneous larva migrans:
Uncinaria, Gnathostoma and Necator. Some fly lar-
vae of the varieties Gasterophylus and Hypoderma
bovis also cause similar clinical pictures. Most cases
are caused by Uncinaria. The principal agents are
Ancylostoma braziliensis and A. caninum. Their
life cycle begins with the expulsion of eggs of the Figure 21.25 Serpiginous track associated with vesiculation.
M21_WK_XXXXX_C21.indd 518 12/18/11 12:06 PM
Insect Bite Infestations 519
• The inflammatory form or migratory panniculitis CUTANEOUS AMEBIASIS
is of variable intensity. It is characterised by the
formation of erythematous, oedematous, circular This is a parasitosis caused by the protozoan,
or irregular, elevated plaques. The surface is Entamoeba hystolytica, which may be found in
warm, and may be associated with pain or a the digestive tract. Through different ways, it may
burning sensation and the rate of migration of the invade the skin and cause painful, rapidly growing
larvae is about 1–5 cm/d. necrotic ulcers.
• The superficial or serpiginous form presents as an
irregular, sinuous track with a mild inflammatory
reaction.
CLINICAL FEATURES The cutaneous form of
3. Larva migrans caused by Strongyloides (anguilluli- amebiasis is rare and is characterised by rapidly
dos): The systemic phase is manifested by Larva cur- growing, necrotic ulcers associated with severe
rens, characterised by rapidly developing (5–15 cm/h) pain, regional adenopathy, fever and malaise. The
serpentine skin lesions that may spontaneously disap- ulcers have a central zone of granulation covered by
pear in a few hours. They frequently present around purulent exudates or fibrin with necrotic tissues and
the anus and in the gluteal area and can affect the an intensely erythematous halo and well-defined
lumbar, pelvic and thoracic regions. The cutaneous margins. Rarely, multiple ulcers and other clinical
lesions are accompanied by intense pruritus and variants including vegetative, verrucous or hyperk-
sometimes, by a papular, pseudourticarial eruption.
eratotic tumours may be present. The lesions do not
4. Larva migrans caused by fly larvae: This is also known
as rampant or migratory myasis. The species of gen-
usually heal spontaneously. They grow rapidly and
der Gasterophylus are the main aetiological agents, can lead to extensive destruction of genital areas.
and the species G. intestinalis, G. haemorrhoidalis and
G. precorum are, among others, the most frequently INVESTIGATIONS Amoeba are usually found
involved. These are habitual parasites of the stomach microscopically from fresh material taken from
and rectum of horses. In humans, the larvae tunnel into the base of the ulcer and placed on a glass slide to
the epidermis and form linear tracks that progress by which warm saline solution is added to stimulate
1–2 cm daily. Vesicles and blisters form along the track. movement. On biopsy of the edge of the lesion, tro-
Larval activity and pruritis are more intense at night. phozoites may be seen.
COURSE This is a self-limited disease and humans TREATMENT Emetine and dehydroemetine are
are ‘dead-end’ hosts. Most larvae die and the lesions the drugs of choice. Emetine is given in a dose of
resolve within 4–6 weeks. 1 mg/kg/d for 10 days. Dehydroemetine is given IM
and its dose should not exceed 60 mg/d, because of
MANAGEMENT The best way to prevent cuta- cardiac effects.
neous larva migrans (CLM) is to ban dogs from Metronidazole may be given orally, in a dose
beaches or wear shoes while walking on the beach of 30–40 mg/kg/d, for 21 days. Iodochlorohydroxy-
and to lie on the sand only on tide-washed areas or quinolein 0.25 g can be given 3 times a day for 2–3
on a mattress (a towel does not give enough protec- weeks along with emetine and dehydroemetine.
tion). Symptomatic relief can be provided by topical
application of a corticosteroid preparation under MYIASIS
occlusion.
Myiasis is an infestation of tissues by the larval form
Although the human host is a ‘dead end’ in the
of non-biting dipterous insects (flies). Species of flies
life cycle and this disease is self limiting, spontane-
involved in myiasis include the genera Dermatobia
ous remission takes up to 12 weeks and intervention
(human botfly), Cochliomyia (screw worm), Cordy-
is essential. This includes administration of topical
lobia, Chrysomya, Cuterebra (rodent or rabbit bot-
or oral antihelminthics (albendazole, thiabendazole
fly), Oestrus (sheep botfly), Gasterophilus (horse
and ivermectin). The regimens include:
botfly), Hypoderma (warble fly), Phaenicia (also
• Topical thiabendazole 10–15% cream, applied twice known as Lucilia) (blowfly) and Wohlfahrtia (flesh
to thrice daily, for 5–10 days fly), among others. In Asia, the common causes are
• Oral albendazole in a dose of 400 mg daily for 3–5 days Chrysomya and Wohlfahrtia and in Africa, Cordy-
• A single dose of 12 mg of oral ivermectin lobia and Chrysomya.
M21_WK_XXXXX_C21.indd 519 12/18/11 12:06 PM
520 Insect Bite Infestations
MODE OF TRANSMISSION The mode of trans- removal of the human botfly from pregnant women
mission is different for different species. The human involves surgical removal using a cruciform incision.
botfly deposits its eggs on a mosquito or other The three-step process is as follows:
blood-feeding insect, which then transfers them to • Aesthetising the area around the aperture (which
effectively paralyses the larva) with an injection of
the host. Cordylobia species deposit their eggs onto
1% lidocaine.
moist clothing, blankets or sand. The larvae pen- • Covering the breathing hole with a sterile occlu-
etrate the skin after contact with the host. sive ointment (polymyxin B in this case) to suf-
Other organisms deposit their eggs directly on focate the larva.
open wounds or orifices. In some cases, the larvae • Placement of a cruciform incision slightly off centre
move about in the subcutis (migratory myiasis), from the breathing hole to extract the whole larva.
mimicking the pattern of cutaneous larva migrans.
Miscellaneous Agents Camphor (in a concentra-
This is caused by Hypoderma bovis (warble fly),
tion of 1:0 and 1:1) demonstrated a 100% mortal-
whose normal hosts are cattle, or Gasterophilus intes-
ity rate of the Oestrus ovis (sheep nasal botfly) lar-
tinalis (horse botfly), which normally infects horses.
vae. Essential oil of betel in a concentration of 3%
In wound myiasis (Cochliomyia hominivorax—
and 4% was effective in killing 100% of the larvae
New World screw worm), the larvae initially consume
(Chrysomya).
necrotic debris but may proceed to feed on normal
tissue. Furuncular myiasis occurs following the
penetration of normal skin by the larvae. A pruritic BEDBUGS (HEMIPTERA)
papule develops at the site. This slowly enlarges over This small blood-sucking insect was largely eradi-
several weeks into a domed nodule (resembles a cated in developing countries around the 1950s sec-
furuncle). The lesion has a central pore through which ondary to the widespread use of DDT. Within the
the posterior end of the larva protrudes intermittently. past 3 years, 500% increase in the number of cases
The larva can be induced to exit the lesion by covering of bedbug infestations have been reported from the
this exit with pork fat or petrolatum. United States and Europe.
The factors for this increase include, the fre-
TREATMENT quency and ease of international travel, their non-
General Measures To prevent infestation by dependence on the surrounding environment for
Cordylobia spp., people should avoid wearing reproduction, survival time of up to 1 year without
damp clothing or resting in sandy areas and cloth- a blood meal and the ideal environment prevalent
ing can be sun- or heat-dried and/or pressed Insect in urban cities. The sites of transfer include shelters,
repellents can be used to keep mosquitoes carrying hotels and apartment units.
larval eggs away.
Insect: Flattened dorsolaterally, with an ovoid body.
Specific Treatment Most treatment recommenda-
The light to red brown bedbug is wingless, and the adult
tions are based on in vitro experiments or case studies. is typically about 6 mm in length.
1. Furuncular myiasis: The various options include sur-
gical debridement; occlusion/suffocation (i.e. with
petrolatum, liquid paraffin, beeswax, nail polish, LIFE CYCLE/MODE OF INFECTION The life
heavy oils); ethyl chloride sprays; lidocaine injections; cycle has five stages and it completes in about 6–8
cryotherapy; chloroform in vegetable oil or ivermec- weeks. The adult bedbug can typically live for 6–12
tin. Treatment consists of the following measures: months. A female lays 200–500 eggs which remain
• Mechanical removal with a haemostat cemented and hatch within 6–10 days at room tem-
• Compression with a pair of wooden spatula on perature. They are extremely robust creatures and
either side of the nodule so that the larva emerges
remain alive in temperatures as low as 7°C, and as
vertically out of the skin, like a ‘grain of rice’
• Mechanical removal with forceps—in some cases
high as 45°C. At homes, bedbugs hide in the dark
under anaesthesia—after applying a small amount crevices of walls, furniture, picture frames, and peel-
of commercially available mineral turpentine) ing wall-paper, the folds of clothing and linens or in
2. Wound myiasis can be cured by surgical debridement the corners of suitcases. There are two separate species
or surgical removal. An effective treatment for the of bedbug, Cimex adjunctus and Cimex pilosellus.
M21_WK_XXXXX_C21.indd 520 12/18/11 12:06 PM
Insect Bite Infestations 521
TREATMENT
Management of Bites Bedbug bites are self-lim-
ited and usually resolve within 1–2 weeks without
treatment. Topical steroids may be used to control
inflammation, and antihistamines may be given to
control pruritus in pronounced cases.
Other Measures
1. The patient should be instructed to launder all bed
linen and vacuum clean the furniture to reduce the
number of bedbugs and their progeny in the home.
2. Prevention of bites and infestations. Covering exposed
parts is the simplest way of preventing the bites. The
following measures should be followed:
• Covering entrances to known refuges of bedbugs
with tape or other tightly woven material effec-
tively hampers bedbug mobility.
• Covering bedposts with petrolatum or inserting
bedposts into jars of paraffin oil may help prevent
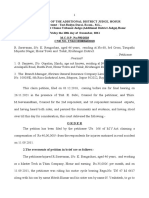
Figure 21.26 Although the classic clustering is seen it is bedbugs from gaining access to the bed.
by no way specific of bedbugs and can be • Insecticides like pyrethroid class of insecticides are
seen due to other insect bites also. particularly effective in controlling bedbug infes-
tations. A study from India compared effective-
CLINICAL FEATURES Typically, bedbug bites ness of DEET, DEPA (diethyl phenyl acetamide)
occur at night, and the patient awakes with new and DMP (diethylphthalate) against bedbugs. It
lesions. Bite reactions occur on exposed sites such found DEET to be superior to the rest. Mattresses
as the face, neck, arms and hands, with two to three can be treated with many formulations, but only
lesions in a row (‘breakfast, lunch, dinner’; Fig. 21.26). at seams and buttons.
The typical reaction to the bite of is the development • Vacuuming bedbugs is particularly effective, but it
of an erythematous wheal, followed by a firm, reddish does not usually remove eggs effectively because
they are glued to the substrate.
papule. Occasionally a small central haemorrhagic
punctum may be visualised. In unexposed individu-
als, the bite appears as erythematous, pruritic mac- Resistance Resistance to both deltamethrin and
ules while in sensitised individuals, intensely pruritic L-cyhalothrin, two pyrethroid insecticides, as well
papules, papular urticaria or vesicles/bullae may occur. as chlorfenapyr, has occurred in laboratory popula-
Changes secondary to scratching include exco- tions of bedbugs. Moreover, pyrethroid insecticides
riations, eczematous dermatitis and secondary can cause bedbugs to scatter within a home simply
infections. to avoid treated areas.
ACKNOWLEDGEMENTS
The first three authors have contributed to the section on scabies. The images are of Indian patients.
REFERENCES
Chosidow O, Giraudeau B, Cottrell J, et al. Oral ivermectin versus malathion lotion for difficult-to-treat head lice.
N Engl J Med 2010;362(10):896–905.
Mellanby K. Man’s reaction to mosquito bites. Nature 1946;158:554.
Mellanby K. The development of symptoms, parasitic infection and immunity in human scabies. Parasitology
1944;35:197–206.
M21_WK_XXXXX_C21.indd 521 12/18/11 12:06 PM
522 Insect Bite Infestations
Walton S, Low Choy J, Bonson A, et al. Genetically distinct dog-derived and human-derived Sarcoptes scabiei in scabies-
endemic communities in northern Australia. Am J Trop Med Hyg 1999;61(4):542–7.
Walton SF, Holt DC, Currie BJ, Kemp DJ. Scabies: New future for a neglected disease. Adv Parasitol 2004;57:309–76.
FURTHER READING
Albanese G, Venturi C, Galbiati G. Treatment of larva migrans cutanea (creeping eruption): A comparison between
albendazole and traditional therapy. Int J Dermatol 2001;40:67–71.
Alexander JOD. Arthropods and Skin. Berlin: Springer-Verlag. 1984:50–55.
Almeida HJ. Treatment of steroid-resistant nodular scabies with topical pimecrolimus. J Am Acad Dermatol
2005;53:357–8.
Barkwell R, Shields S. Deaths associated with ivermectin treatment for scabies. Lancet 1997;349(9059):1144–5.
Bigby M. A systematic review of the treatment of scabies. Arch Dermatol 2000;136(3):387–9.
Billich A, Aschauer H, Aszodi A, Stuetz A. Percutaneous absorption of drugs used in atopic eczema: Pimecrolimus per-
meates less through skin than corticosteroids and tacrolimus. Int J Pharm 2004;269(1):29–35.
Blackwell V, Vega-Lopez F. Cutaneous larva migrans: Clinical features and management of 44 cases presenting in the
returning traveler. Br J Dermatol 2001;145:434–7.
Brwon M, Hebert AA. Insect repellants: An overview. JAAD 1997;36:243–9.
Burgess I. Head lice. Clin Evid 2004;11:2168–73.
Burgess IF. Pediculosis. J Am Acad Dermatol 2004;50:1–12.
Cabrera R, Dahl MV. The immunology of scabies. Semin Dermatol 1993;12(1):15–21.
Caumes E. Treatment of cutaneous larva migrans. Clin Infect Dis 2000;30:811–14.
Chosidow O. Clinical practices. Scabies. N Engl J Med 2006;354(16):124–9.
Chosidow O. Ivermectin: Main results of efficacy and safety data in scabies. In: 20th World Congress of Dermatology.
Paris; 2002.
Chosidow O. Scabies. N Engl J Med 2006;354(16):1718–27.
Chosidow O. Scabies and pediculosis. Lancet 2000;355(9206):819–26.
Currie BJ, Harumal P, McKinnon M, Walton SF. First documentation of in vivo and in vitro ivermectin resistance in
Sarcoptes scabiei. Clin Infect Dis 2004;39(1):8–12.
Diamantis SA, Morrell DS, Burkhart CN. Treatment of head lice. Dermatol Ther 2009;22(4):273–8.
Dissemond J, Schröter S, Franckson T, Herbig S, Goos M. Pimecrolimus in an adhesive ointment as a new treatment
option for oral lichen planus. Br J Dermatol 2004;150(4):782–4.
Elston D. Controversies concerning the treatment of lice and scabies. J Am Acad Dermatol 2002;46(5):794–96.
Elston DM. Drugs used in the treatment of pediculosis. J Drugs Dermatol 2005;4:207–11.
Estes S, Arlian L. Survival of Sarcoptes scabiei. J Am Acad Dermatologic Clin 1981;5(3):343.
Flinders DC, de Schweinitz P. Pediculosis and scabies. Am Fam Phys 2004;69(2):341–8.
Frankowski BL. American Academy of Pediatrics guidelines for the prevention and treatment of head lice infestation.
Am J Manag Care 2004;10:S269–72.
Gibbs S. Skin disease and socioeconomic conditions in rural Africa: Tanzania. Int J Dermatol 1996;35(9):633–9.
Glaziou P, Cartel JL, Alzieu P, Briot C, Moulia-Pelat JP, Martin PMV. Comparison of ivermectin and benzyl benzoate for
treatment of scabies. Trop Med Parasitol 1993;44:331–2.
Greive KA, Lui AH, Barnes TM, Oppenheim VM. A randomized, assessor-blind, parallel-group, multicentre, phase
IV comparative trial of a suffocant compared with malathion in the treatment of head lice in children. Australas J
Dermatol 2010;51(3):175–82.
Hengge UR, Currie BJ, Jager G, Lupi O, Schwartz RA. Scabies: A ubiquitous neglected skin disease. Lancet Infect Dis
2006;6(12):769–79.
Hernandez-Perez E. Resistance to antiscabietic drugs. J Am Acad Dermatol 1983;8:1121–2.
Heukelbach J, Feldmeier H. Scabies. Lancet 2006;367(9524):1767–74.
M21_WK_XXXXX_C21.indd 522 12/18/11 12:06 PM
Insect Bite Infestations 523
Hogan D, Schachner L, Tanglertsampam C. Diagnosis and treatment of childhood scabies. Pediatr Clin North Am J
Physiol 1990;38:941–56.
Jacobson CC, Abel EA, Parasitic infestations. J Am Acad Dermatol 2007;56:1026–43.
Kar SK, Mania J, Patnaik S. The use of ivermectin for scabies. Natl Med J India 1994;7(1):15–16.
Karthikeyan K. Treatment of scabies: Newer perspectives. Postgrad Med J 2005;81(951):7–11.
Kolb A, Needham GR, Neyma KM, High WA. Bedbugs. Dermatol Ther 2009;22: 347–52.
Kulthanan K, Wongkamchai S, Triwongwaranat D. Mosquito allergy: Clinical features and natural course. J Dermatol
2010;37:1–7.
Kumarasinghe SP, Karunaweera ND, Ihalamulla RL, Arambewela LS, Dissanayake RD. Larvicidal effects of mineral
turpentine, low aromatic white spirits, aqueous extracts of Cassia alata, and aqueous extracts, ethanolic extracts
and essential oil of betel leaf (Piper betle) on Chrysomya megacephala. Int J Dermatol 2002;41:877–80.
Kumarasinghe SPW, Karunaweera ND, Ihalamulla RL. A study of cutaneous myiasis in Sri Lanka. Int J Dermatol
2000;39:689–94.
Kurt O, Balcio lu IC, Burgess IF, et al. Treatment of head lice with dimeticone 4% lotion: Comparison of two formula-
tions in a randomized controlled trial in rural Turkey. BMC Public Health 2009;9:441.
Labeling changes for Lindane. FDA Consum 2003;37(3):6.
Lalli PN, Morgan MS, Arlian LG. Skewed Th1/Th2 immune response to Sarcoptes scabiei. J Parasitol 2004;90(4):
711–14.
Leppard B, Naburi AE. The use of ivermectin in controlling an outbreak of scabies in a prison. Br J Dermatol
2000;143(3):520–23.
Ly F, Caumes E, Ndaw CA, Ndiaye B, Mahe A. Ivermectin versus benzyl benzoate applied once or twice to treat human
scabies in Dakar, Senegal: A randomized controlled trial. Bull World Health Organ 2009;87(6):424–30.
Mackenzie I. Scabies treated by a benzyl benzoate emulsion. Br Med J 1941;1:403–5.
Mallen K. Benzyl benzoate in treatment of scabies. A comparison of the effects of aqueous and spirit emulsions. Br Med
J 1942;2:452–3.
Maria IH, Dirk ME. Scabies. Dermatologic Ther 2009;22(4):279–92.
McKoy R, Moshella S, Orkin M, et al. Parasitic infections and infestations. In: Orkin M, Maibach HI, Dahl MV, editors.
Dermatology. East Norwalk CI: Appleton & Lange; 1991:189–214.
Meinking T, Infestations. Curr Prob Dermatol 1999;11:80–103.
Meinking T, Taplin D, Hermida J, Pardo R, Kerdel F. The treatment of scabies with ivermectin. N Engl J Med
1995;333(1):26–30.
Meinking TL, Villar ME, Vicaria M, et al. The clinical trials supporting benzyl alcohol lotion 5% (Ulesfia): A safe and
effective topical treatment for head lice (pediculosis humanus capitis). Pediatr Dermatol 2010;27(1):19–24.
Mounsey KE, Holt DC, McCarthy JS, Currie BJ, Walton SF. Longitudinal evidence of increasing in vitro tolerance of
scabies mites to ivermectin in scabies-endemic communities. Arch Dermatol 2009;145(7):840–41.
Mytton OT, McGready R, Lee SJ, et al. Safety of benzyl benzoate lotion and permethrin in pregnancy: A retrospective
matched cohort study. BJOG 2007;114(5):582–7.
Oberoi S, Ahmed RS, Suke SG, Bhattacharya SN, Chakraborti AD, Banerjee B. Comparative effect of topical appli-
cation of lindane and permethrin on oxidative stress parameters in adult scabies patients. Clin Biochem 2007;
40(16–17):321–4.
O’Quinn JC, Dushin R. Cutaneous larva migrans. Case report with current recommendations for treatment. J Am Podi-
atr Med Assoc 2005;95:291–4.
Ostlere LS, Harris D, Rustin MHA. Scabies associated with a bullous pemphigoid-like eruption. Br J Dermatol
1993;128:217–19.
Paasch U, Haustein UF. Treatment of endemic scabies with allethrin, permethrin and ivermectin. Evaluation of a treat-
ment strategy. Hautarzt 2001;52(1):31–7.
Purvis R, Tyring S. An outbreak of lindane-resistant scabies treated successfully with permethrin 5% cream. J Am Acad
Dermatol 1991;25(6, Pt 1):1015–16.
Roos TC, Alam M, Roos S, Merk HF, Bickers DR. Pharmacotherapy of ectoparasitic infections. Drugs 2001;61(8):
1067–88.
M21_WK_XXXXX_C21.indd 523 12/18/11 12:06 PM
524 Insect Bite Infestations
Roth W. Scabies resistant to lindane 1% lotion and crotamiton 10% cream. J Am Acad Dermatol 1991;24(3):502–3.
Schultz M, Gomez M, Hansen R, et al. Comparative study of 5% permethrin cream and 1% lindane lotion for the treat-
ment of scabies. Arch Dermatol 1990;126:167–70.
Shahab RKA, Loo DS. Bullous scabies. J Am Acad Dermatol 2003;49(2):346–50.
Sullivan JR, Watt G, Barker B. Successful use of ivermectin in the treatment of endemic scabies in a nursing home.
Australas J Dermatol 1997;38(3):137–40.
Taplin D, Meinking T. Infestations. In: Schachner L, Hansen R, editors. Pediatric Dermatology. New York: Churchill
Livingstone; 1988:1465–515.
Taplin D, Meinking TL, Chen JA, Sanchez R. Comparison of crotamiton 10% cream (eurax) and permethrin 5% cream
(elimite) for the treatment of scabies in children. Pediatr Dermatol 1990;7(1):67–73.
Taplin D, Porcelain SL, Meinking TL, et al. Community control of scabies: A model based on use of permethrin cream.
Lancet 1991;337:1016–18.
Usha V, Gopalakrishnan Nair TV. A comparative study of oral ivermectin and topical permethrin cream in the treatment
of scabies. J Am Acad Dermatol 2000;42(2, Pt 1):236–40.
Victoria J, Trujillo R, Barreto M. Myiasis: A successful treatment with topical ivermectin. Int J Dermatol 1999;38:142–4.
Walker GJ, Johnstone PW. Interventions for treating scabies. Cochrane Database Syst Rev 2000;3.
Walton SF, Currie BJ. Problems in diagnosing scabies, a global disease in human and animal populations. Clin Microbiol
Rev 2007;20(2):268–79.
M21_WK_XXXXX_C21.indd 524 12/18/11 12:06 PM
View publication stats
You might also like
- 610-Article Text-3639-1-10-20220823Document7 pages610-Article Text-3639-1-10-20220823Gaema MiripNo ratings yet
- JEADV Clinical Practice - 2022 - Absil - Scabies and Therapeutic Resistance Current Knowledge and Future PerspectivesDocument8 pagesJEADV Clinical Practice - 2022 - Absil - Scabies and Therapeutic Resistance Current Knowledge and Future Perspectivestravel doctorNo ratings yet
- Scabies: A Clinical Update: FocusDocument34 pagesScabies: A Clinical Update: FocusAbdulAzizNo ratings yet
- Hand, Foot and Mouth Disease: Australian Family Physician September 2003Document3 pagesHand, Foot and Mouth Disease: Australian Family Physician September 2003giselaNo ratings yet
- Scabies - Epidemiology, Clinical Features, and Diagnosis - UpToDateDocument61 pagesScabies - Epidemiology, Clinical Features, and Diagnosis - UpToDateJorge ArcentalesNo ratings yet
- Oral Medicine - Update For The Dental Practitioner Lumps and SwellingsDocument9 pagesOral Medicine - Update For The Dental Practitioner Lumps and SwellingsGowriNo ratings yet
- Extensive Mucocutaneous Verruca Vulgaris Case ReportDocument4 pagesExtensive Mucocutaneous Verruca Vulgaris Case ReportRaswijayanti RusliNo ratings yet
- Document From BenjaminfjodDocument21 pagesDocument From BenjaminfjodBenjamin VanlaltlansangaNo ratings yet
- Dracunculiasis: The 'Guinea Worm' DiseaseDocument7 pagesDracunculiasis: The 'Guinea Worm' DiseaseSePeHR SHNo ratings yet
- ScabiesDocument13 pagesScabiespompas pNo ratings yet
- Measles PDFDocument3 pagesMeasles PDFdrpranandhaNo ratings yet
- Rare Genital Disseminated Superficial Porokeratosis in Immunocompetent ManDocument3 pagesRare Genital Disseminated Superficial Porokeratosis in Immunocompetent ManMostafaAhmedNo ratings yet
- Varicella Zoster Virus Infection: July 2015Document19 pagesVaricella Zoster Virus Infection: July 2015nickNo ratings yet
- Biology, diagnosis and management of sarcoptic mange in animals and occasionally humansDocument3 pagesBiology, diagnosis and management of sarcoptic mange in animals and occasionally humansradityaNo ratings yet
- Complicated MeaslesDocument13 pagesComplicated MeaslesFarica Armane AquinoNo ratings yet
- Scabies Norwegian Presenting As Erythroderma in HIV A Case ReportDocument4 pagesScabies Norwegian Presenting As Erythroderma in HIV A Case ReportfakhrunnisaNo ratings yet
- Oral Tuberculosis: Case ReportDocument2 pagesOral Tuberculosis: Case ReportMauriceNo ratings yet
- Skin Infections in Australian Aboriginal Children: A Narrative ReviewDocument7 pagesSkin Infections in Australian Aboriginal Children: A Narrative Reviewyusak sampeNo ratings yet
- Guidelines For Management of Monkeypox DiseaseDocument23 pagesGuidelines For Management of Monkeypox DiseaseMinerva Medical Treatment Pvt LtdNo ratings yet
- How To Manage ScabiesDocument13 pagesHow To Manage ScabiesDaniela SerbanNo ratings yet
- Infectious Diseases in Pediatric Otolaryngology - Infections of The External EarDocument14 pagesInfectious Diseases in Pediatric Otolaryngology - Infections of The External EarGading AuroraNo ratings yet
- Scabies: Diagnostic and Therapeutic Update: Robert N. RichardsDocument7 pagesScabies: Diagnostic and Therapeutic Update: Robert N. RichardsanantaNo ratings yet
- Insight Into ScabiesDocument3 pagesInsight Into ScabiesVicky Pérez KlalaNo ratings yet
- Scabies ResistenDocument10 pagesScabies ResistenHana MelissaNo ratings yet
- Norwegian Scabies A Challenging Dermatologic ConditionDocument2 pagesNorwegian Scabies A Challenging Dermatologic Conditionenda sitepuNo ratings yet
- Foot and Mouth DiseasesDocument3 pagesFoot and Mouth Diseaseseutamène ramziNo ratings yet
- Warts and Their Look-Alikes, How To Identify and Treat Them - Clinical Review - James H. HerndonDocument8 pagesWarts and Their Look-Alikes, How To Identify and Treat Them - Clinical Review - James H. HerndonYuldashNo ratings yet
- Chickenpox 1Document7 pagesChickenpox 1Nica Joy CandelarioNo ratings yet
- Darier Disease A Fold (Intertriginous) DermatosisDocument5 pagesDarier Disease A Fold (Intertriginous) Dermatosisdaniel ayllonNo ratings yet
- 408 2022 Article 528Document8 pages408 2022 Article 528nathanaellee92No ratings yet
- Ls2 Elem Las21 To-Las67-MergedDocument47 pagesLs2 Elem Las21 To-Las67-MergedJaypee AturoNo ratings yet
- Scabies Clinical Manifestations and Diagnosis 2015 Polish Annals of MedicinDocument4 pagesScabies Clinical Manifestations and Diagnosis 2015 Polish Annals of MedicinAbrahamisnanNo ratings yet
- Common Communicable Diseases GR.8 Lesson 3RD QDocument54 pagesCommon Communicable Diseases GR.8 Lesson 3RD QAiza May RosasNo ratings yet
- Feline calicivirus infection ABCD guidelines on prevention and managementDocument10 pagesFeline calicivirus infection ABCD guidelines on prevention and managementDevy Kartika HadiNo ratings yet
- Scabies Handbook v2011Document32 pagesScabies Handbook v2011Magdalena Corry Mega ChristinNo ratings yet
- ShimoseDocument6 pagesShimoseIsabella Puspa DewiNo ratings yet
- Special: Noma: Life Cycle of A Devastating Sore - Case Report and Literature ReviewDocument6 pagesSpecial: Noma: Life Cycle of A Devastating Sore - Case Report and Literature ReviewEl Defensor Teas: 100 NaturalNo ratings yet
- Viral Diseases With Rashes LastDocument46 pagesViral Diseases With Rashes LastHasan kahhalehNo ratings yet
- Herpes ZosterDocument6 pagesHerpes ZosterJimmy JNo ratings yet
- A Brief Note On: Chicken PoxDocument29 pagesA Brief Note On: Chicken PoxRemesh ChandranNo ratings yet
- Monkey PoxDocument29 pagesMonkey PoxMalavika A GNo ratings yet
- ScabiesDocument8 pagesScabiesJessica Dumayas Dela RosaNo ratings yet
- SDS PaperDocument11 pagesSDS PaperJaxen NormanNo ratings yet
- Communicable Diseases GR.8 HealthDocument40 pagesCommunicable Diseases GR.8 HealthAiza May RosasNo ratings yet
- CUTANEOUS Tuberculosis - AjmDocument3 pagesCUTANEOUS Tuberculosis - Ajmfredrick damianNo ratings yet
- High Fever, Maculopapular Rash, Perianal Desquamation, and Conjunctivitis in A 3-Year-Old BoyDocument8 pagesHigh Fever, Maculopapular Rash, Perianal Desquamation, and Conjunctivitis in A 3-Year-Old BoyTri ApriastiniNo ratings yet
- Diagnosis, Prevention and Treatment of Scabies: A ReviewDocument5 pagesDiagnosis, Prevention and Treatment of Scabies: A ReviewSince Ivanna RumbiakNo ratings yet
- Prevalence of scabies and impetigo worldwide: a systematic reviewDocument8 pagesPrevalence of scabies and impetigo worldwide: a systematic reviewMuhammad AmrullahNo ratings yet
- Lancet ArticleDocument11 pagesLancet ArticlemikhaelyosiaNo ratings yet
- ScabiesDocument9 pagesScabiesLycopersicum EsculentumNo ratings yet
- Konjungtivitis GonoreDocument2 pagesKonjungtivitis Gonorefk unswagatiNo ratings yet
- Patient Care Pathogen Reservoir Mode of Transmission: Viral Infections of HumansDocument21 pagesPatient Care Pathogen Reservoir Mode of Transmission: Viral Infections of HumansMark Vincent JanoyogNo ratings yet
- Clinical Features of Viral Exanthems: Sarajane Ting, Rosemary NixonDocument6 pagesClinical Features of Viral Exanthems: Sarajane Ting, Rosemary NixonJustine Frances CabalayNo ratings yet
- Psoriasis: Common DermatosesDocument7 pagesPsoriasis: Common DermatoseslaluneNo ratings yet
- Management and Treatment of Herpes Simplex Keratitis: June 2016Document8 pagesManagement and Treatment of Herpes Simplex Keratitis: June 2016debbyNo ratings yet
- VariselaDocument5 pagesVariselaalrisimanungkalit27No ratings yet
- TetanusDocument105 pagesTetanusbubujuhumNo ratings yet
- Common Child and AdolescentDocument23 pagesCommon Child and AdolescentValeria BeltranNo ratings yet
- Penyebab Virus - Flaviridae (Dengue)Document32 pagesPenyebab Virus - Flaviridae (Dengue)Bendy Dwi IrawanNo ratings yet
- Critical Appraisal of Qualitative Studies: Was A Qualitative Approach Appropriate?Document5 pagesCritical Appraisal of Qualitative Studies: Was A Qualitative Approach Appropriate?Peregrine Albertus Ricco AzaliNo ratings yet
- Critical Appraisal of Qualitative Studies: Was A Qualitative Approach Appropriate?Document5 pagesCritical Appraisal of Qualitative Studies: Was A Qualitative Approach Appropriate?Peregrine Albertus Ricco AzaliNo ratings yet
- Insect and Allergic ReactionDocument7 pagesInsect and Allergic ReactionGesta Qurrotu AyuninnataNo ratings yet
- Critical Appraisal #2 (Descriptive)Document13 pagesCritical Appraisal #2 (Descriptive)T.A.BNo ratings yet
- DTSCH Arztebl Int-115 0012-DikonversiDocument25 pagesDTSCH Arztebl Int-115 0012-DikonversizeniafadilaNo ratings yet
- DTSCH Arztebl Int-115 0012-DikonversiDocument25 pagesDTSCH Arztebl Int-115 0012-DikonversizeniafadilaNo ratings yet
- FentonDocument1 pageFentonzeniafadilaNo ratings yet
- Insect and Allergic ReactionDocument7 pagesInsect and Allergic ReactionGesta Qurrotu AyuninnataNo ratings yet
- Dapus ReferatDocument3 pagesDapus ReferatzeniafadilaNo ratings yet
- Ii Evaluation of The Allergic ReactionDocument19 pagesIi Evaluation of The Allergic ReactionzeniafadilaNo ratings yet
- Designsolutions 2010springDocument68 pagesDesignsolutions 2010springjkarpitskiyNo ratings yet
- Power of The Pinch Pinch Lower Lid BlepharoplastyDocument6 pagesPower of The Pinch Pinch Lower Lid BlepharoplastyBFF BotoxNo ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- Human Population and EnvironmentDocument4 pagesHuman Population and Environmentmonkeybike88No ratings yet
- NCM 101 Vital Signs PPT BSN 1a Group 1Document138 pagesNCM 101 Vital Signs PPT BSN 1a Group 1Brian Anthony100% (1)
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- Low Endotoxin Recovery (LER) in Drug Products - Original - 31428Document2 pagesLow Endotoxin Recovery (LER) in Drug Products - Original - 31428Putri DozanNo ratings yet
- Babu Jagjivan RamDocument24 pagesBabu Jagjivan RamAnonymous qFWInco8cNo ratings yet
- A Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshDocument15 pagesA Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshEditor IJTSRDNo ratings yet
- Cricket Academy Head Coach RoleDocument4 pagesCricket Academy Head Coach Roletauseef1716No ratings yet
- Hum. Reprod.-1999-Tesarik-1318-23Document6 pagesHum. Reprod.-1999-Tesarik-1318-23Meilana Sapta DNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- RaweDocument34 pagesRaweSonuNo ratings yet
- Media Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty SiraitDocument15 pagesMedia Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty Siraitnimas ayu kusumaningrumNo ratings yet
- Display PDFDocument8 pagesDisplay PDFSri BalajiNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- CV 2020Document3 pagesCV 2020api-519861494No ratings yet
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)
- The Works of Alan OpenshawDocument38 pagesThe Works of Alan OpenshawAlan OpenshawNo ratings yet
- Professional Growth and DevelopmentDocument154 pagesProfessional Growth and DevelopmentNina Anne Paracad100% (3)
- Soal Bahasa Inggris Kelas 5Document8 pagesSoal Bahasa Inggris Kelas 5imam hambaliNo ratings yet
- Umftgm 2017 MarissiensisDocument148 pagesUmftgm 2017 MarissiensisAdriana VillarrealNo ratings yet
- A Critical Review of The Effect of Working Conditions On Employee PerformanceDocument11 pagesA Critical Review of The Effect of Working Conditions On Employee PerformanceStephanie Bacunawa0% (1)
- Should Homework Be Banned From School?Document7 pagesShould Homework Be Banned From School?Chuyên ĐỗNo ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Organon of Medicine All Years 2marks Question Viva Questions AnswersDocument12 pagesOrganon of Medicine All Years 2marks Question Viva Questions Answersabcxyz15021999No ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- Head To Toe Patient AssessmentDocument2 pagesHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet