You might also like
- Total Spanish Course: Learn Spanish With The Michel Thomas Method: Beginner Spanish Audio Course - Michel ThomasDocument5 pagesTotal Spanish Course: Learn Spanish With The Michel Thomas Method: Beginner Spanish Audio Course - Michel Thomasguhofyki0% (1)
- Open World First B2 Students BookDocument257 pagesOpen World First B2 Students BookTuan Anh Bui88% (8)
- Homeo Eye DiseaseDocument15 pagesHomeo Eye DiseaseAlbena Trifonova100% (3)
- Romanian Association of Drilling Contractors ACFRDocument83 pagesRomanian Association of Drilling Contractors ACFRFuBasho33% (3)
- Halftrack Track Chains InstructionsDocument4 pagesHalftrack Track Chains Instructionsddlevy0% (1)
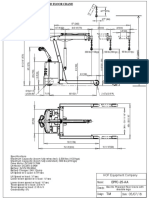
- Electric floor crane adjustable legsDocument1 pageElectric floor crane adjustable legsprabhakaran.cNo ratings yet
- 10.1136@bjophthalmol 2019 315441Document8 pages10.1136@bjophthalmol 2019 315441연화화양No ratings yet
- Glaucoma - State of The Art and Perspectives On TreatmentDocument17 pagesGlaucoma - State of The Art and Perspectives On TreatmentbarbaraNo ratings yet
- HHS Public Access: Role of Cataract Surgery in The Management of GlaucomaDocument13 pagesHHS Public Access: Role of Cataract Surgery in The Management of GlaucomaayuNo ratings yet
- Glaucoma REVIEW - JAMADocument11 pagesGlaucoma REVIEW - JAMAGermano Freire Bezerra FilhoNo ratings yet
- JCM 11 02895Document13 pagesJCM 11 02895Jocho NeavesNo ratings yet
- GlaucomaDocument11 pagesGlaucomaerkalemNo ratings yet
- Glaucoma and Ocular HypertensionDocument6 pagesGlaucoma and Ocular HypertensionsoniasistNo ratings yet
- Improving Care of Chronic Open Angle Glaucoma: FeatureDocument7 pagesImproving Care of Chronic Open Angle Glaucoma: FeatureDhea Fitri HandayaniNo ratings yet
- The Pathophysiology and Treatment of Glaucoma PDFDocument22 pagesThe Pathophysiology and Treatment of Glaucoma PDFNurul Dwi LestariNo ratings yet
- LXII Edward Jackson Lecture: Open Angle Glaucoma After VitrectomyDocument12 pagesLXII Edward Jackson Lecture: Open Angle Glaucoma After VitrectomyZhafirah BahriNo ratings yet
- Glaucoma Nursing Care and Hypertension Risk FactorsDocument13 pagesGlaucoma Nursing Care and Hypertension Risk FactorsShaimaa AliNo ratings yet
- RF GlaucomaDocument6 pagesRF Glaucomamaandre123No ratings yet
- POAG Article Yumori CadoganDocument7 pagesPOAG Article Yumori CadoganAndro SinagaNo ratings yet
- Differences in Structural Parameters in Patients With Open-Angle Glaucoma, High Myopia and Both Diseases Concurrently. A Pilot StudyDocument14 pagesDifferences in Structural Parameters in Patients With Open-Angle Glaucoma, High Myopia and Both Diseases Concurrently. A Pilot Study钟华No ratings yet
- The Safety of Orthokeratology-A Systematic ReviewDocument8 pagesThe Safety of Orthokeratology-A Systematic ReviewBAYUNo ratings yet
- Idemiology of MyopiaDocument14 pagesIdemiology of MyopiaWing Yan LamNo ratings yet
- Prevalence of Glaucoma in North Costal Andhra PradeshDocument7 pagesPrevalence of Glaucoma in North Costal Andhra PradeshIJAR JOURNALNo ratings yet
- Evaluation of a glaucoma patient articleDocument11 pagesEvaluation of a glaucoma patient articleameehasanahNo ratings yet
- Glaucoma 9Document13 pagesGlaucoma 9Sheila Kussler TalgattiNo ratings yet
- Epidemiology of Glaucoma - The Past, Present, and Predictions For The FutureDocument9 pagesEpidemiology of Glaucoma - The Past, Present, and Predictions For The FutureFiska FianitaNo ratings yet
- Nur Ulfah - Prevalence of Sign and Symptoms of Dry Eye After Refractive SurgeryDocument11 pagesNur Ulfah - Prevalence of Sign and Symptoms of Dry Eye After Refractive Surgerybudi haryadiNo ratings yet
- Weinreb Fisiopatologia y Tto Del Glaucoma 2014 3Document22 pagesWeinreb Fisiopatologia y Tto Del Glaucoma 2014 3Jessica Paola Numpaque LoaizaNo ratings yet
- Update On Normal Tension Glaucoma: Review ArticleDocument10 pagesUpdate On Normal Tension Glaucoma: Review ArticleVlady BordaNo ratings yet
- Weinreb 2014Document11 pagesWeinreb 2014José Adrian Espejel GuzmánNo ratings yet
- Anti-VEGF Treatment Is The Key Strategy For Neovascular Glaucoma Management in The Short TermDocument8 pagesAnti-VEGF Treatment Is The Key Strategy For Neovascular Glaucoma Management in The Short TermhellowNo ratings yet
- Revisi Ke-3 Journal Glaucoma (Group 12)Document12 pagesRevisi Ke-3 Journal Glaucoma (Group 12)TaschiaNo ratings yet
- The Pathophysiology and Treatment of GlaucomaDocument11 pagesThe Pathophysiology and Treatment of GlaucomaelisaNo ratings yet
- Normal Tension Glaucoma: A Different Disease?: Kuldev SinghDocument3 pagesNormal Tension Glaucoma: A Different Disease?: Kuldev SinghRasha Mounir Abdel-Kader El-TanamlyNo ratings yet
- Resiko Jatuh GlaukomaDocument5 pagesResiko Jatuh GlaukomayohanaNo ratings yet
- 1 s2.0 S2667376222000130 MainDocument8 pages1 s2.0 S2667376222000130 MainelfiahNo ratings yet
- Ni Hms 436399Document18 pagesNi Hms 436399Devanti EkaNo ratings yet
- Acute Closed Angle Glaucoma: AuthorsDocument4 pagesAcute Closed Angle Glaucoma: AuthorsRova OktavaniNo ratings yet
- Glaucoma Case ReportDocument9 pagesGlaucoma Case Reportsuci caraswatiNo ratings yet
- Glaucoma Fisiopatologia Review 14Document11 pagesGlaucoma Fisiopatologia Review 14rbarcellonaNo ratings yet
- Prevalence of Blindness in Patients With Uveitis: Original ResearchDocument4 pagesPrevalence of Blindness in Patients With Uveitis: Original ResearchMuhammad RaflirNo ratings yet
- What We Have Learned From The Ocular Hypertension TreatmentDocument8 pagesWhat We Have Learned From The Ocular Hypertension TreatmentASHOK KUMAR SINGHNo ratings yet
- Red Eye: A Guide For Non-Specialists: MedicineDocument14 pagesRed Eye: A Guide For Non-Specialists: MedicineFapuw Parawansa100% (1)
- Joanna KonopinskaDocument12 pagesJoanna KonopinskaKarel de KlerkNo ratings yet
- Endpd PDFDocument29 pagesEndpd PDFNaveen AgrawalNo ratings yet
- A Rare Complication of Combined Oral Contraceptives (Cocs) : Optic NeuritisDocument3 pagesA Rare Complication of Combined Oral Contraceptives (Cocs) : Optic NeuritisGufront MustofaNo ratings yet
- Uveitis 2Document9 pagesUveitis 2srihandayaniakbarNo ratings yet
- Etiology and Features of Eyes With Rubeosis Iridis Among Korean Patients: A Population-Based Single Center StudyDocument8 pagesEtiology and Features of Eyes With Rubeosis Iridis Among Korean Patients: A Population-Based Single Center StudynuhajazminNo ratings yet
- Global Magnitude of Visual Impairment Caused by UnDocument9 pagesGlobal Magnitude of Visual Impairment Caused by UnRuby KhanNo ratings yet
- Bmri2015 742792 PDFDocument13 pagesBmri2015 742792 PDFLina Shabrina QoribNo ratings yet
- Bmri2015 742792Document13 pagesBmri2015 742792Potencia SalasNo ratings yet
- Aos0091 0406Document7 pagesAos0091 0406maandre123No ratings yet
- Approach To Optic Neuritis - An UpdateDocument11 pagesApproach To Optic Neuritis - An UpdateAlexandros GidarakosNo ratings yet
- 1 SMDocument7 pages1 SMAriNo ratings yet
- Trends in The Therapeutic Drug Delivery System For The Management of Glaucoma A ReviewDocument8 pagesTrends in The Therapeutic Drug Delivery System For The Management of Glaucoma A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- HHS Public Access: Advances in Dry Eye Disease TreatmentDocument25 pagesHHS Public Access: Advances in Dry Eye Disease TreatmentjojdoNo ratings yet
- Case Study 1Document28 pagesCase Study 1Sean Carl TubilNo ratings yet
- Nutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFDocument64 pagesNutritional Supplementation in The Treatment of Glaucoma - A Systematic Review 2018 PDFjvprasad100% (1)
- Review: Definition of Glaucoma: Clinical and Experimental ConceptsDocument9 pagesReview: Definition of Glaucoma: Clinical and Experimental ConceptsYunguo YuNo ratings yet
- Eye 2011154 ADocument7 pagesEye 2011154 AAmba PutraNo ratings yet
- Questions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Document13 pagesQuestions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Afni YunitaNo ratings yet
- Myopia Control: A Review: Jeffrey J. WallineDocument6 pagesMyopia Control: A Review: Jeffrey J. WallineChristine Yohana SianturiNo ratings yet
- Nursing Practice Review Ophthalmology: in This Article..Document7 pagesNursing Practice Review Ophthalmology: in This Article..intan juitaNo ratings yet
- Update On Normal Tension Glaucoma: Review ArticleDocument5 pagesUpdate On Normal Tension Glaucoma: Review ArticleNur Rakhma AkmaliaNo ratings yet
- ABSTRAKDocument1 pageABSTRAKDony Dwi PutraNo ratings yet
- 1Document2 pages1Dony Dwi PutraNo ratings yet
- BHP Wetlab FixDocument14 pagesBHP Wetlab FixDony Dwi PutraNo ratings yet
- BHP Wetlab FixDocument14 pagesBHP Wetlab FixDony Dwi PutraNo ratings yet
- ABSTRAKDocument1 pageABSTRAKDony Dwi PutraNo ratings yet
- ABSTRAKDocument1 pageABSTRAKDony Dwi PutraNo ratings yet
- OkDocument1 pageOkDony Dwi PutraNo ratings yet
- BHP Wetlab FixDocument14 pagesBHP Wetlab FixDony Dwi PutraNo ratings yet
- Dur EngDocument29 pagesDur EngDony Dwi PutraNo ratings yet
- Management of Secondary Angle Closure Glaucoma: Jocgp JocgpDocument8 pagesManagement of Secondary Angle Closure Glaucoma: Jocgp JocgpDony Dwi PutraNo ratings yet
- List of Doctors by Name and SpecialtyDocument11 pagesList of Doctors by Name and SpecialtyDony Dwi PutraNo ratings yet
- List Penerima SertifikatDocument6 pagesList Penerima SertifikatDony Dwi PutraNo ratings yet
- BHP Wetlab FixDocument14 pagesBHP Wetlab FixDony Dwi PutraNo ratings yet
- Laporan Kasus-Low Vision Dengan NystagmusDocument9 pagesLaporan Kasus-Low Vision Dengan NystagmusDony Dwi PutraNo ratings yet
- OkDocument1 pageOkDony Dwi PutraNo ratings yet
- List Penerima SertifikatDocument6 pagesList Penerima SertifikatDony Dwi PutraNo ratings yet
- Jurnal GlaukomaDocument13 pagesJurnal GlaukomaDony Dwi PutraNo ratings yet
- Papan Nama POLIDocument2 pagesPapan Nama POLIDony Dwi PutraNo ratings yet
- Energy Imbalance-Obesity: Fakultas Kedokteran Universitas Brawijaya DR Bambang PrijadiDocument42 pagesEnergy Imbalance-Obesity: Fakultas Kedokteran Universitas Brawijaya DR Bambang PrijadiDony Dwi PutraNo ratings yet
- BHP Wetlab FixDocument14 pagesBHP Wetlab FixDony Dwi PutraNo ratings yet
- XDocument2 pagesXSophiaFrancescaEspinosaNo ratings yet
- Nutrition: DR Hiten KalraDocument81 pagesNutrition: DR Hiten KalraAmit SagarNo ratings yet
- MGT-01 (14.03.23) - QPDocument19 pagesMGT-01 (14.03.23) - QPSrinivas VakaNo ratings yet
- SAP On ASE Development UpdateDocument16 pagesSAP On ASE Development Updatebetoy castroNo ratings yet
- 2 - ARM Cotex-M3 - IntroductionDocument124 pages2 - ARM Cotex-M3 - IntroductionNghĩa VũNo ratings yet
- Procurement Policy For Bank Group Funded OperationsDocument28 pagesProcurement Policy For Bank Group Funded OperationsNiyi FunminiyiNo ratings yet
- Quintin Kynaston School Wikipedia.Document3 pagesQuintin Kynaston School Wikipedia.John_Adam_St_Gang_QKNo ratings yet
- Regulatory Guide 1.71Document5 pagesRegulatory Guide 1.71Siis IngenieriaNo ratings yet
- Literatur Riview Tentang Faktor Penyebab Klaim Tidak Layak Bayar BPJS Kesehatan Di Rumah Sakit Tahun 2020Document8 pagesLiteratur Riview Tentang Faktor Penyebab Klaim Tidak Layak Bayar BPJS Kesehatan Di Rumah Sakit Tahun 2020Maulida LutfiaNo ratings yet
- Recommended Reads by David PerellDocument3 pagesRecommended Reads by David PerellRonit MandalNo ratings yet
- Turkey GO (896-22)Document1 pageTurkey GO (896-22)shrabon001No ratings yet
- Coastal Boards Co Is A Merchandising Business The Account BalancesDocument1 pageCoastal Boards Co Is A Merchandising Business The Account BalancesFreelance WorkerNo ratings yet
- Mad-Lib ExerciseDocument2 pagesMad-Lib Exercisejbk23100% (2)
- Most Popular Bootstrap Interview Questions and AnswersDocument6 pagesMost Popular Bootstrap Interview Questions and Answershassan TariqNo ratings yet
- What Is Your Future Plan EssayDocument3 pagesWhat Is Your Future Plan Essayafhbexrci100% (2)
- MUET Registration for Malaysian University TestDocument1 pageMUET Registration for Malaysian University TestLaila HaliliNo ratings yet
- NEBULIZATIONDocument2 pagesNEBULIZATIONMae ValenzuelaNo ratings yet
- Chapter 11Document3 pagesChapter 11Kristine TiuNo ratings yet
- Saint Patrick's Day CelebrationsDocument96 pagesSaint Patrick's Day CelebrationsRicardo Jackichan Barzola LopezNo ratings yet
- AdinaDocument542 pagesAdinaSafia SoufiNo ratings yet
- Navigating Indonesia's E-Commerce - Omnichannel As The Future of Retail - SIRCLO - KIC 2021Document144 pagesNavigating Indonesia's E-Commerce - Omnichannel As The Future of Retail - SIRCLO - KIC 2021Suci RamaDaniNo ratings yet
- Beyond Investment: The Power of Capacity-Building SupportDocument44 pagesBeyond Investment: The Power of Capacity-Building SupportLaxNo ratings yet
- Experiment # 6 Heat of Solution Uy, Angelica A., Uson, Ma. Agatha Beatrice, Vargas, Louise ErikaDocument7 pagesExperiment # 6 Heat of Solution Uy, Angelica A., Uson, Ma. Agatha Beatrice, Vargas, Louise ErikaAngelica UyNo ratings yet
- Sokkia MagnetDocument9 pagesSokkia Magnetbbutros_317684077No ratings yet