You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Basic CementingDocument49 pagesBasic CementingRobert Salimifard100% (2)
- Bartholins Gland Squamous Cell Carcinoma A Rare VDocument5 pagesBartholins Gland Squamous Cell Carcinoma A Rare VWalida FadillahNo ratings yet
- Bartholins Gland Carcinomas A 20 Plus-Year ExperiDocument4 pagesBartholins Gland Carcinomas A 20 Plus-Year ExperiWalida FadillahNo ratings yet
- Neodymium-YAG Iridotomy in Closure Glaucoma: Preliminary StudyDocument5 pagesNeodymium-YAG Iridotomy in Closure Glaucoma: Preliminary StudyWalida FadillahNo ratings yet
- Accepted Manuscript: Diabetes Research and Clinical PracticeDocument28 pagesAccepted Manuscript: Diabetes Research and Clinical PracticeWalida FadillahNo ratings yet
- FullDocument10 pagesFullWalida FadillahNo ratings yet
- Mortality After Incident Cancer in People With and Without Type 2 DiabetesDocument6 pagesMortality After Incident Cancer in People With and Without Type 2 DiabetesWalida FadillahNo ratings yet
- Molecules 16 02075 v2 PDFDocument9 pagesMolecules 16 02075 v2 PDFWalida FadillahNo ratings yet
- Kerala Ayurveda Kendra-MenuDocument6 pagesKerala Ayurveda Kendra-MenuPartheebanNo ratings yet
- Narrative Report v.1Document4 pagesNarrative Report v.1Crisyl Lipawen100% (1)
- Subject Taken NotesDocument3 pagesSubject Taken NotessuriyasureshNo ratings yet
- Día de MuertosDocument12 pagesDía de MuertosAlejandra RodriguezNo ratings yet
- Dulegaunda Lamagaun 20 TH November 2018Document132 pagesDulegaunda Lamagaun 20 TH November 2018Deepak YadavNo ratings yet
- Seem Collaborative Standards For Mathematics (CCSS)Document63 pagesSeem Collaborative Standards For Mathematics (CCSS)RejieNo ratings yet
- Your Wellness IntelligenceDocument1 pageYour Wellness Intelligencelackua100% (1)
- 64 YoginisDocument180 pages64 YoginisJaideep Singh100% (5)
- Tutorial - 1 - Heat Transfer Simulation Using Altair SimLabDocument17 pagesTutorial - 1 - Heat Transfer Simulation Using Altair SimLabklausoshoNo ratings yet
- Common Model Exam Set-XV (B) (2079-4-14) QuestionDocument16 pagesCommon Model Exam Set-XV (B) (2079-4-14) QuestionSameer KhanNo ratings yet
- Navera - Belligerence As Argument The Allure of The War Metaphor in Philippine Presidential SpeechesDocument16 pagesNavera - Belligerence As Argument The Allure of The War Metaphor in Philippine Presidential SpeechesJolo RianNo ratings yet
- Energy Worker Transition Provisions in The Clean Energy Jobs ActDocument956 pagesEnergy Worker Transition Provisions in The Clean Energy Jobs ActKelsey LandisNo ratings yet
- z482 E3b en (3a2)Document2 pagesz482 E3b en (3a2)Gerencia General ServicesNo ratings yet
- Hitachi L-2100Document98 pagesHitachi L-2100nohnaimer69No ratings yet
- CSR Report AdiDocument10 pagesCSR Report AdiadieothmanNo ratings yet
- Psychological TestingDocument9 pagesPsychological Testingpedro augusto calixto nascomentoNo ratings yet
- Fixed PointDocument580 pagesFixed PointMichael AdrianNo ratings yet
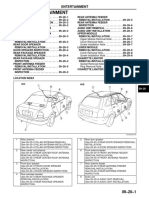
- EntertainmentDocument9 pagesEntertainmentSebastian SirventNo ratings yet
- Airport Board Game Come Fly With MeDocument2 pagesAirport Board Game Come Fly With MeJaqueline CairesNo ratings yet
- Essential Immediate Newborn CareDocument33 pagesEssential Immediate Newborn CareShenaNo ratings yet
- Egress Modelling of Pedestrians For The Design of Contemporary Stadia John Gales Full ChapterDocument51 pagesEgress Modelling of Pedestrians For The Design of Contemporary Stadia John Gales Full Chaptergeorge.reese767100% (7)
- Russuff SSM BeverlyDocument4 pagesRussuff SSM Beverlyazila taibNo ratings yet
- 11Document25 pages11Suraj KumarNo ratings yet
- Chemical, Biological, Radiological, Nuclear (CBRN) DefenseDocument19 pagesChemical, Biological, Radiological, Nuclear (CBRN) DefenseMarco R PaguiriganNo ratings yet
- Native Philippine ProductsDocument13 pagesNative Philippine ProductsJereza Joy LastreNo ratings yet
- Heating Vent Lighting SE7542Document48 pagesHeating Vent Lighting SE7542sairajNo ratings yet
- Specification of Cat 320cDocument28 pagesSpecification of Cat 320cDan AbellaNo ratings yet
- Participatory Community Forest Management in The GambiaDocument25 pagesParticipatory Community Forest Management in The GambiaEbrima S. DemNo ratings yet
- LM6501 User ManualDocument35 pagesLM6501 User Manualapi-37978960% (1)