You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Auerbachs Wilderness Medicine 2 Volume Set 7th EditionDocument61 pagesAuerbachs Wilderness Medicine 2 Volume Set 7th Editionmatthew.grasso983100% (48)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Prayer Before MeetingDocument1 pagePrayer Before MeetingjayNo ratings yet
- QUIZ: Formation of The Solar System: Mark Your Answers On The Scantron ProvidedDocument10 pagesQUIZ: Formation of The Solar System: Mark Your Answers On The Scantron ProvidedjayNo ratings yet
- Action Research Ritche 2015 On Pedagogic Instruction in Physics Second Copy Submitted Ti Sir Aa..Document12 pagesAction Research Ritche 2015 On Pedagogic Instruction in Physics Second Copy Submitted Ti Sir Aa..jayNo ratings yet
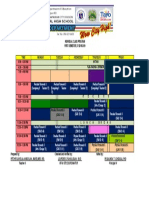
- Class Program 2017-2018Document2 pagesClass Program 2017-2018jayNo ratings yet
- INDIVIDUAL CLASS PROGRAM Division Practical Research 2 For Mam LourdesDocument1 pageINDIVIDUAL CLASS PROGRAM Division Practical Research 2 For Mam LourdesjayNo ratings yet
- Prak8 - Brosur Obat Ventolin PDFDocument25 pagesPrak8 - Brosur Obat Ventolin PDFWAODE YUMNA ULTAMIL KARNONo ratings yet
- Histopathological Aspects of Psoriasis and Its Uncommon VariantsDocument12 pagesHistopathological Aspects of Psoriasis and Its Uncommon VariantsIkaNo ratings yet
- Kode Icd 10 Poli GigiDocument5 pagesKode Icd 10 Poli GigiPoppy Novita Ritonga100% (1)
- What Are The Symptoms of Back PainDocument4 pagesWhat Are The Symptoms of Back PainPotchie PFIZERNo ratings yet
- Tension PneumothoraxDocument5 pagesTension PneumothoraxKay BristolNo ratings yet
- A. D. TBI, Rehabilitation of Traumatic Brain InjuryDocument68 pagesA. D. TBI, Rehabilitation of Traumatic Brain InjuryRupali Raut100% (1)
- AdenomaDocument4 pagesAdenomaPark JiminNo ratings yet
- IndicesDocument4 pagesIndiceshosam ahmedNo ratings yet
- Colonoscopy: Dr. Aries Budianto, SPB (K) BDDocument52 pagesColonoscopy: Dr. Aries Budianto, SPB (K) BDRisal WintokoNo ratings yet
- Morning Report: Supervisor: Dr. Ratih Barirah, SP - OGDocument7 pagesMorning Report: Supervisor: Dr. Ratih Barirah, SP - OGPradipta ShivaNo ratings yet
- J of Oral Rehabilitation - 2023 - Manfredini - Standardised Tool For The Assessment of BruxismDocument51 pagesJ of Oral Rehabilitation - 2023 - Manfredini - Standardised Tool For The Assessment of BruxismRhamon MendonçaNo ratings yet
- Respiratory FailureDocument39 pagesRespiratory FailureMuntasir BashirNo ratings yet
- High Risk Neonatal Nursing CareDocument40 pagesHigh Risk Neonatal Nursing Careha,hr124100% (1)
- Lasers in GlaucomaDocument33 pagesLasers in GlaucomaAnumeha Jindal100% (1)
- NCPDocument3 pagesNCPKorina FranciscoNo ratings yet
- Golden Rules in OncologyDocument76 pagesGolden Rules in OncologyDragonNo ratings yet
- Reflection Drug EducationDocument1 pageReflection Drug Educationanoncat -No ratings yet
- D Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsDocument6 pagesD Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsMrudula SureshNo ratings yet
- Orem Based Brain Rehab Clinic Is The First in The State To Offer Innovative GyroStim Neuro TherapyDocument2 pagesOrem Based Brain Rehab Clinic Is The First in The State To Offer Innovative GyroStim Neuro TherapyPR.comNo ratings yet
- Midterm Study Guide (OMND 7070) (WK 1-5)Document10 pagesMidterm Study Guide (OMND 7070) (WK 1-5)Bridget MasonNo ratings yet
- Cardiology Flash CardsDocument5 pagesCardiology Flash CardsRodrigo FonsecaNo ratings yet
- Six LevelsDocument3 pagesSix LevelsDoktormin106No ratings yet
- Haematological Side Effects of Antiepileptic Drug Treatment in Patients With Epilepsy,, Nrowy 2011Document8 pagesHaematological Side Effects of Antiepileptic Drug Treatment in Patients With Epilepsy,, Nrowy 2011Mohammed Abdullah AlqaadNo ratings yet
- 1 How Can You Maintaining Your Personal HygieneDocument8 pages1 How Can You Maintaining Your Personal Hygieneanupa bhattaraiNo ratings yet
- MRCPCH 2 Questions For May 2015Document4 pagesMRCPCH 2 Questions For May 2015Saadia JavaidNo ratings yet
- Brain CancerDocument24 pagesBrain CancerChyna Marielle MonteroNo ratings yet
- Lesson 2 3 Feedback DiaryDocument5 pagesLesson 2 3 Feedback DiaryDon Aldrich SantosNo ratings yet
- New 5Document37 pagesNew 5rishi gupta100% (1)
- Monthly Census of Chemotherapy Administration-Surgery-1Document13 pagesMonthly Census of Chemotherapy Administration-Surgery-1myvi317No ratings yet