You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Emotionally Focused Therapy - ManualDocument37 pagesEmotionally Focused Therapy - ManualEdy-Claude Okalla Bana67% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Practical Guide To Strategic Planning in Higher EducationDocument59 pagesA Practical Guide To Strategic Planning in Higher EducationPaLomaLujan100% (1)
- Electronic Data ProcessingDocument8 pagesElectronic Data ProcessingJayvee Puntalba Calinog100% (1)
- The Top 100 Common Usage ProblemsDocument4 pagesThe Top 100 Common Usage ProblemsJayvee Puntalba Calinog100% (2)
- Argumentatvie Essay FinalDocument4 pagesArgumentatvie Essay Finalapi-242418017No ratings yet
- Formal Observation Report 1 1Document8 pagesFormal Observation Report 1 1api-535562565No ratings yet
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document5 pagesDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogNo ratings yet
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document4 pagesDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogNo ratings yet
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document4 pagesDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogNo ratings yet
- Jayvee Calinog OJT AMA Time StampDocument4 pagesJayvee Calinog OJT AMA Time StampJayvee Puntalba CalinogNo ratings yet
- Attendance - Small SundayDocument1 pageAttendance - Small SundayJayvee Puntalba CalinogNo ratings yet
- Social InequalityDocument55 pagesSocial InequalityJayvee Puntalba Calinog100% (1)
- Network TopologyDocument7 pagesNetwork TopologyJayvee Puntalba CalinogNo ratings yet
- Phase 3 GuideDocument28 pagesPhase 3 GuideYufei ChenNo ratings yet
- Introduction To Stage Management - PowerPointDocument21 pagesIntroduction To Stage Management - PowerPointKylie Howell100% (1)
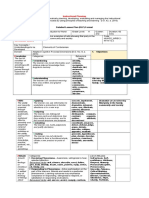
- Lesson Plan No.2Document7 pagesLesson Plan No.2Carlo CalumbaNo ratings yet
- Safety and Health Handbook: Faculty of Electrical EngineeringDocument23 pagesSafety and Health Handbook: Faculty of Electrical EngineeringHe StoppableNo ratings yet
- Answer Sheet in Tle-9: RD RDDocument2 pagesAnswer Sheet in Tle-9: RD RDJaideHizoleSapulNo ratings yet
- Mentor Critique Form Nick Filled OutDocument1 pageMentor Critique Form Nick Filled Outapi-660578780No ratings yet
- Time MethodDocument100 pagesTime MethodManea SilviuNo ratings yet
- Enc 1101 - Unit Project - Final 1Document30 pagesEnc 1101 - Unit Project - Final 1api-267948590No ratings yet
- Human Development Essay AP PsychDocument2 pagesHuman Development Essay AP PsychKiley MaloneyNo ratings yet
- Recruit, Selection and PlacementDocument35 pagesRecruit, Selection and PlacementNazmul HasanNo ratings yet
- Latest Free Study Material For NEET Exams 2020Document3 pagesLatest Free Study Material For NEET Exams 2020Disha PublicationNo ratings yet
- Education System Serbia PDFDocument23 pagesEducation System Serbia PDFTatjana Pop-AntoskaNo ratings yet
- The Teacher and The Community DeveloperDocument3 pagesThe Teacher and The Community DeveloperHelen Grace Galdo100% (4)
- FutebolDocument447 pagesFutebolflaviodomi100% (2)
- InterventionDocument13 pagesInterventionEmma Manio Pascual100% (1)
- DLP 2Document5 pagesDLP 2Baby YanyanNo ratings yet
- Frontrunner 2 SyllabusDocument2 pagesFrontrunner 2 SyllabusDavid WilliamsNo ratings yet
- Rural Study PDFDocument47 pagesRural Study PDFSabita BhagabatiNo ratings yet
- ResourcesDocument2 pagesResourcesapi-663319599No ratings yet
- Eapp DLL Week 6 (Matatag)Document4 pagesEapp DLL Week 6 (Matatag)Daisy CadienteNo ratings yet
- Globalisation and Historiography of National Leaders Symbolic Representations in School Textbooks 1st Edition Joseph ZajdaDocument54 pagesGlobalisation and Historiography of National Leaders Symbolic Representations in School Textbooks 1st Edition Joseph Zajdaerik.torres368100% (10)
- 7th Grade LetterDocument3 pages7th Grade Letterapi-263447784No ratings yet
- Andhra Pradesh Grama - Ward SachivalayamDocument1 pageAndhra Pradesh Grama - Ward Sachivalayammamatha suneelNo ratings yet
- CSTP 3 Ocampo 09Document9 pagesCSTP 3 Ocampo 09api-635281515No ratings yet
- Criteria of A Good CurriculumDocument11 pagesCriteria of A Good CurriculumFides Hope Camille Rojo67% (3)
- Filipino Values MonthDocument3 pagesFilipino Values MonthAaron ArasaNo ratings yet